Article Text

Abstract
Objective To assess the prevalence and risk factors of gestational diabetes mellitus (GDM) in a population known to have a high prevalence of abnormal glucose metabolism.
Methods A household random population-based cross-sectional study of 13 627 women in the childbearing age, who were subjected to fasting plasma glucose if they were not known to have been diagnosed before with any type of diabetes. GDM cases were diagnosed using the International Association of Diabetes and Pregnancy Study Group (IAPSG) criteria.
Results The overall GDM prevalence was 36.6%, categorised into 32.4% new cases and 4.2% known cases. Another 3.6% had preconception type 1 or 2 diabetes. GDM cases were older and had a significantly higher body mass index, in addition to a higher rate of macrocosmic baby and history of GDM. Monthly income, educational level, living in urban areas and smoking were not found to be significantly different between normal and GDM cases. The most important and significant risk factors for GDM were history of GDM, macrosomic baby, obesity and age >30 years. However, hypertension, low high-density lipoprotein, family history of diabetes and increased triglycerides did not show any significant effect on GDM prevalence in this cohort.
Conclusions This society is facing a real burden of abnormal glucose metabolism during pregnancy, where almost half of the pregnant women are subjected to maternal and neonatal complications. Early screening of pregnant women, especially those at a high risk for GDM, is mandatory to identify and manage those cases.
- Diabetes & Endocrinology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
Our study is a community household-based study seeking cases with abnormal glucose metabolism among pregnant women in a country ranked the seventh worldwide in terms of diabetes prevalence.
-
The new International Association of Diabetes and Pregnancy Study Group (IAPSG) criteria were used to screen for gestational diabetes mellitus (GDM) cases at a community setup rather than hospital based, especially when there are a limited number of studies that have used these criteria.
-
The studied cohort is unique because of its swift socioeconomic transition observed in the Saudi society that gives a good setup to assess different modifiable and non-modifiable risk factors for GDM and to compare this with other ethnicities.
-
One of the limitations of this study was the use of fasting plasma glucose (FPG) that was found to have lower sensitivity when compared with the oral glucose tolerance test (OGTT), although it has been recently recommended by the American Diabetes Association (ADA) in 2011 for GDM screening.
Introduction
Ever since gestational diabetes mellitus (GDM) was first recognised in 1967,1 it has been the primary focus of interest for clinicians and scientists, due to its increased risk of fetal macrosomia, neonatal hypoglycaemia, jaundice, polycythaemia, hypocalcaemia, and also its increased frequency of maternal hypertensive disorders with the need for cesarean deliveries.2 GDM, an asymptomatic disorder, is defined as glucose intolerance with the onset or its first recognition during pregnancy. It is the most common metabolic disorder accounting for almost 90% of all diabetes cases during pregnancy, and has been found to be present in approximately 7% of all pregnant women.3 Moreover, mothers with a history of GDM are at a greater risk of developing type 1 diabetes (5–10%)4 or type 2 diabetes (over 70%),5 while their offspring are more likely to be obese or to suffer from diabetes in their later life.6 The global prevalence of GDM ranges between 1% and 14% depending on the population studied and the diagnostic tests used.3 The prevalence estimates for GDM in 2007 were the following: 11.6% for Asian Indians, 10% for Vietnamese, 9.8% for Pacific Islanders and 7.9% for East Asians and while it ranged from 4% to 6% for Hispanics, it was found to be 4% in non-Hispanic African-Americans and 4.7% in non-Hispanic Caucasians.7
Even though a hospital-based study among Saudi women using the National Diabetes Data Group (NDDG) criteria8 showed the GDM prevalence to be 12.5%, no community-based study has been undertaken to look into the extent of this medical problem in the Kingdom of Saudi Arabia even after knowing that the risk factors of GDM are highly prevalent in this society.
During the childbearing period, women are subjected to increased risk of abnormal glucose metabolism with the progression of age and other general risk factors including obesity and physical inactivity. Several reproductive risk factors, namely parity, the presence of polycystic ovary, the history of GDM, macrosomic baby >4.5 kg, and the use of contraceptive drugs, have been found to significantly increase the risk of abnormal glucose metabolism in this group of women.9 ,10
Based on the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study results, the International Association of Diabetes and Pregnancy Study Group (IADPSG) recommended lowering the fasting plasma glucose threshold for the GDM diagnosis to ≥92 mg/dL (5.1 mmol/L),11 which was also adopted by the American Diabetes Association (ADA) in 2011.12 These new diagnostic criteria, as expected, resulted in a significant increase in GDM prevalence in many countries,13–15 where it had increased from 10.3% to 30.1% in Mexicans15 while reaching up to 30.5% and 37.7% in Norway and UAE.16 ,17
The aim of the present study was to investigate the prevalence of different abnormal glucose conditions among pregnant women in the Kingdom of Saudi Arabia. The prevalence of GDM and its different risk factors were also investigated using the new IADPSG diagnostic criteria.
Methods
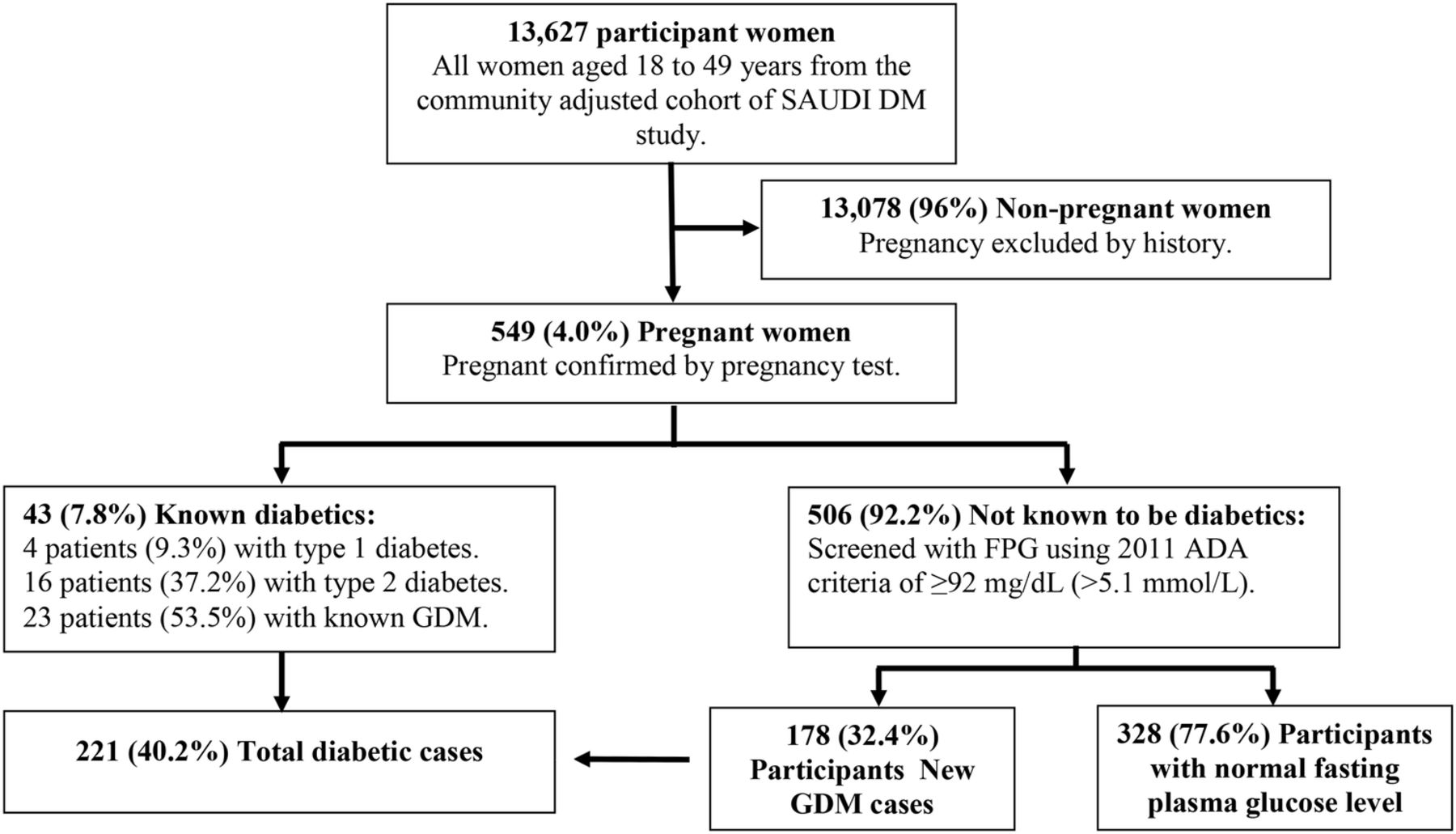
The Saudi Abnormal Glucose Metabolism and Diabetes Impact Study (SAUDI-DM study) is a household random population-based cross-sectional study conducted at a national level in the Kingdom of Saudi Arabia during the period 2007–2009. After adjusting for age, gender and geographical distribution according to the 2007 census, a total of 53 370 participants were used for the assessment of different states of abnormal glucose metabolism. Of those participants, 13 627 participants were found to be women in their childbearing age (18–49 years) as shown in figure 1, and among those women participants, 549 participants were found to be pregnant in different trimesters confirmed by their pregnancy tests, who represented 4% of the total women participants’ cohort. All the SAUDI-DM participants gave their consent to participate and were subjected to interviews. Clinical assessment of the participants, which included pregnant women, where their clinical data including age, family history of diabetes, history of GDM and macrosomic baby, educational level, monthly income, smoking status, and residency area were all collected by specially trained primary care physicians from the 13 official regions. The anthropometric parameters including weight, height, body mass index (BMI), waist-to-hip ratio and blood pressure were all measured by trained nurses.

Sample selection of childbearing age pregnant women from of the Saudi Abnormal Glucose Metabolism and Diabetes Impact Study (SAUDI-DM) cohort classified according to abnormal glucose metabolism status.
Pregnant women who were not known to be suffering from diabetes were tested for FPG and lipids profile after overnight fasting for at least 10 h and 3 days of usual activity and diet. Using the IADPSG criteria, pregnant women were diagnosed with GDM if FPG was ≥92 mg/dL (5.1 mmol/L).
All the blood samples collected using vacuum tubes containing sodium fluoride were transported to the Strategic Center for Diabetes Research laboratory in Riyadh. Blood glucose assessment was performed using the glucose oxidase–peroxidase methodology, serum cholesterol assessment was performed using the cholesterol oxidase–peroxidase methodology, and high-density lipoprotein (HDL), low-density lipoprotein and triglyceride assessments were performed using the direct glycerokinase oxidase–peroxidase methodology as provided by Mindray (B5BS-200) chemistry analyser reagent (China).
Statistical analysis
All data were analysed using SPSS V.17. Descriptive analyses and frequency tables were performed using this programme for all variables. The χ2 test was used for categorical variables, while the t test was used for continuous variables. OR with 95% CI were used for assessing the risk factor using univariate analysis. p Value of <0.05 was used as the level of significance.
Results
Table 1 describes the characteristics of the study population. Of the selected cohort containing Saudi pregnant women, 43 participants were women with known diabetes (7.8%), of which 4 participants (9.3%) were found to be patients with type 1 diabetes, 16 participants (37.2%) were found to be patients with type 2 diabetes, and 23 participants (53.5%) were found to be with GDM. And among the remaining 506 women not known to be suffering from diabetes, 178 (32.4%) were found to be new GDM cases. The studied cohort was divided into three age groups: the first group is between 18 and 29 years of age with a total number of 264 (48.1%). The second age group is between 30 and 39 years, totalling to 212 (38.6%), while the third group is between 40 and 49 years with a total number of 73 (13.3%).
Baseline clinical and biochemical characteristics of the selected cohort, newly diagnosed gestational diabetes mellitus (GDM) and normoglycaemic pregnant participants
When comparing the clinical characteristics of GDM cases with the clinical characteristics of pregnant women without diabetes, the GDM cases were found to be significantly older (33.26±7.63 years) (p<0.0001) and more obese as presented by their body weight (73.94±14.83 kg) and BMI (30.27±5.57 kg/m2) (p<0.0001). There was no significant difference between the two groups in their mean height and waist-to-hip ratio (p=0.176). The GDM cases had a significantly higher mean systolic blood pressure (SBP) at 114.02±11.61 mm Hg (p=0.002) and a low diastolic blood pressure at 72.71±8.81 mm Hg (p=0.160). And as expected, the mean FPG was found to be significantly higher in GDM cases at 6.55 (±2.21) mmol/L when compared with the mean FPG of the normal women at 4.21±0.65 mmol/L (p<0.0001). Lipids showed no significant difference between the two groups with the exception of mean HDL, which was found to be lower in the GDM cases at 1.07±0.32 mmol/L when compared with the mean HDL for normal women at 1.15±0.32 mmol/L (p=0.025). The percentage of women with positive family history of diabetes was not found to be significantly different between the GDM cases and normal women (p=0.451), while it was found to be significantly higher for the history of GDM and macrocosmic baby >4.5 kg among GDM cases at 12.49% vs 3.66% (p<0.0001) and 11.44% vs 3.66% (p<0.0001), respectively, when compared with normal women. Educational level showed no significant difference in percentage between the two groups, while the percentage of women with monthly income <4000 SR was found to be significantly higher among normal women (p=0.02). Smoking or living in urban areas also showed no significant difference between the two groups (p=0.811 and p=0.601).
Figure 2 demonstrates the prevalence of different types of abnormal glucose metabolism in the selected cohort of Saudi pregnant women aged 18–49 years. Type 1 diabetes was found in 0.7% of the total sample, while type 2 was reported in 2.9% of the total sample. 4.2% of the total sample were known cases of GDM and 32.4% of the total sample were newly discovered GDM cases. The overall prevalence of abnormal glucose metabolism showed an age specific increase with a significant difference from 31.8% to 43.9% and 60.3% in the age groups 18–29, 30–39 and 40–49 years respectively. The prevalence of newly discovered GDM cases showed an increase from 28.0% to 35.4% and 39.7% in the three groups, respectively. This was also observed in the prevalence of known GDM cases from 1.9% in the age group 18–29 years to 4.7% in the age group 30–39 years and peaking at 11% in the age group 40–49 years. The prevalence of known patients with type 1 and 2 diabetes was 0.8% and 1.1% for the age group 18–29 years, 0.5% and 3.3% for the age group 30–39 years and 1.4% and 8.2% for the age group 40–49 years. The ratio of known to unknown GDM cases was calculated to be1:15, 1:8 and 1:4 for the age groups 18–29, 30–39 and 40–49 years, respectively.

The prevalence of abnormal glucose metabolism in pregnant Saudi women aged 18–49 years.
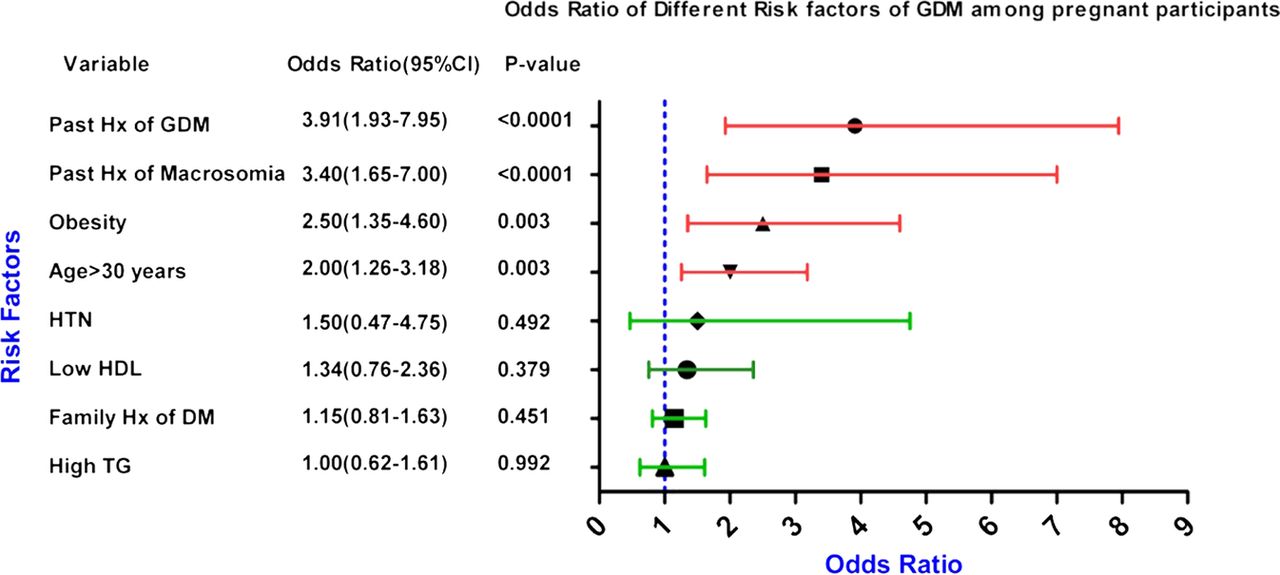
Figure 3 shows the OR (95% CI) , where the history of GDM was found to be a highly significant risk factor with OR 3.91 (95% CI) (1.93 to 7.95) (p<0.0001). It was followed by the history of macrosomic baby weighing >4.5 kg that had OR (95% CI) of 3.40 (1.65 to 7.00) (p<0.0001). Obesity was the third significant risk factor with OR (95% CI) 2.50 (1.35 to 4.60) followed by age >30 years, where the OR (95% CI) was 2.00 (1.26 to 3.18), both with a significant p value (p=0.003). Other risk factors, which include hypertension, low HDL, and family history of diabetes, showed a non-significant increased risk for GDM presented by OR (95% CI) (1.50 (0.47 to 4.75), 1.34 (0.76 to 2.36), and 1.15 (0.81 to 1.63)), respectively. Lastly, the high triglycerides showed no significant risk for GDM.

{kind=link}
{kind=link}
{kind=link}
OR for gestational diabetes mellitus risk factors among Saudi pregnant participants.
Discussion
This study investigated the occurrence of abnormal glucose metabolism during pregnancy using a community-based rather than a traditional hospital based setup. A study with this setup provides a better image of the extent of this medical problem, especially when using the new diagnostic criteria to identify GDM cases at a community level. This study shows the importance of subjecting women to GDM screening, particularly when it is known that only 4.2% of pregnant women were picked up by the health system (known GDM cases). The current survey picked up another 32.4% of GDM cases; this would mean that only one of every nine GDM cases was detected by the antenatal screening, which also clearly demonstrates that there are many undiagnosed GDM cases at the community level. Another crucial finding of this study was that the overall GDM prevalence was 36.6%, threefold higher than what was reported earlier,8 but similar to the findings of studies from other ethnicities using these criteria,15 which is most likely due to the lower cut-off value of the new criteria used and the high prevalence of overweight and obesity reflected by a high mean BMI in the studied cohort. This may be coupled with the fact that such a community-based study would identify more GDM cases, especially in a society where diabetes prevalence is found to be increasing over the past three decades.18 The patients with pre-existing types 1 and 2 diabetes in this study represent 3.6% of all pregnancies, which was three times more than what had been reported in North America19 and is most likely a reflection of the high prevalence of abnormal glucose metabolism in our population.
This studied cohort showed that the mean age for GDM Saudi pregnant women was higher than what had been earlier reported in other studies involving the Chinese and Indian populations,20 ,21 which could be the result of cultural factors that encourage women to get pregnant even at an older age, in addition to high parity.22 This may also have contributed to the higher prevalence of GDM in this cohort with the mean age of GDM cases found to be significantly higher than the normal cases. Another explanation for the higher prevalence of GDM in our cohort is provided by the presence of high mean BMI when compared with the studies involving Caucasian and Asian populations.23 ,24 More than 50% of GDM cases had a family history of diabetes that was not significantly different from normal cases and this could be explained by the high prevalence of diabetes and high consanguinity rates in our society.25 As expected and seen from other studies,21 ,26 the history of GDM and macrosomic baby was found to be higher in GDM cases than in normal pregnant women, where it was almost four times higher in our GDM cohort. Neither education nor monthly income showed any significant increase in GDM cases, with the exception of monthly income less than 4000 SR that was found to be associated with a decreased percentage of GDM cases. Surprisingly, both smoking and living in urban areas showed no significant difference between the two groups, which could be evidently explained on the basis of cultural effects, where smoking is not culturally acceptable for women in Saudi Arabia, and on the basis of high socioeconomic status that has eliminated the difference between urban and rural areas in the Kingdom.
Consistent with many studies27 and as expected, the prevalence of preconception diabetes, known GDM and newly discovered GDM cases showed a significant increase with age, peaking at age more than 40 years. This could be explained by the effect of age progression and muliparity in our society.23 The ratio of the previously known to newly discovered GDM cases decreased with the progression of age, which could be explained by the fact that older women were subjected to screening more than younger women as also observed by other researchers.27
This study also shows that, history of GDM increased the risk for GDM significantly, which was found to be much lower than what had been observed in the studies involving Persian, Indian and Caucasian populations,21 ,26 which could be an effect of the nature of the study sample, with our sample being community based and the rest being hospital based. History of macrosomia was the second risk factor found to increase GDM cases in the Saudi pregnant women, close to what had been reported in other ethnicities.21 ,28 Obesity and being more than 30 years of age, known to be important risk factors for diabetes in general, significantly increased the risk for GDM, as reported earlier in many ethnicities.20 ,23 Hypertension, low HDL, family history of diabetes and high triglycerides were all found to be non-significant risk factors for GDM in this study. Hypertension and low HDL increased the risk for developing GDM in this population but not to a significant level similar to the Caucasians,23 while positive family history of diabetes had a minimal non-significant increase, which could have resulted from high consanguinity rates and family history of diabetes in the general population.25 Although high triglyceride was known to be a risk factor for GDM,23 this study showed no effect of this risk factor, which could be due to the high mean triglycerides in normal and GDM cases.
This study derives strength from being a community-based household survey representing a normal distribution cohort that was randomly selected. One of the limitations of this study was the use of FPG which was found to have lower sensitivity when compared with the oral glucose tolerance test,29 although it has been recently recommended by the ADA for GDM screening.12 Another limitation of this study was the exclusion of pregnancy by history alone, which may have excluded some pregnant women in their early pregnancy in addition to the lack of obstetrical and diet history. Although this study involved special ethnicity, the results could be generalised at an international level, especially when looking at risk factors.
Conclusions
Around 40% of Saudi pregnant women suffer from either pre-existing diabetes or GDM secondary to the increased prevalence of its risk factors in this society. A limited number of GDM cases are picked up by the health system indicating the weak antenatal screening and thereby warranting an extensive public and medical staff education. The GDM risk factors that are significant in this society include: history of GDM and macrosomic baby, obesity and age more than 30 years that should be considered for early screening of pregnant women. Public awareness programmes for reducing modifiable risk factors like obesity would contribute to decreasing the prevalence of GDM and prenatal mortality.
Acknowledgments
The authors would like to acknowledge the staff at the University Diabetes Center and the staff of the primary care centers from the Ministry of Health for their collaboration in conducting the study.
References
Footnotes
-
Contributors All the authors have contributed towards the conduct of the study and preparation of the manuscript. KAR designed the study, wrote the manuscript, designed figures and interpreted data, and approved the final version to be published. HAAM supervised the field work in different health sectors in relation to this project. TAK provided training to the research physicians and did the statistical analysis. AMY researched data, wrote the manuscript, and critically revised the article. AHAS analysed data, developed figures, interpreted data and approved the final version to be published. KS handled and analysed blood samples, revised the article critically and approved the final version to be published. NAA researched data, analysed data and approved the final version to be published.
-
Funding This study was funded by the University Diabetes Center at King Saud University, Ministry of Health and the Tawuniya Company for health insurance.
-
Competing interests None.
-
Ethics approval This study has been approved by the Institutional Review Board (IRB) at the College of Medicine, King Saud University.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.