Article Text

Abstract
Objectives To: (1) determine the percentage of the population in England that have access to a community pharmacy within 20 min walk; (2) explore any relationship between the walking distance and urbanity; (3) explore any relationship between the walking distance and social deprivation; and (4) explore any interactions between urbanity, social deprivation and community pharmacy access.
Design This area level analysis spatial study used postcodes for all community pharmacies in England. Each postcode was assigned to a population lookup table and lower super output area (LSOA). The LSOA was then matched to urbanity (urban, town and fringe or village, hamlet and isolated dwellings) and deprivation decile (using the Index of Multiple Deprivation score).
Primary outcome measure Access to a community pharmacy within 20 min walk.
Results Overall, 89.2% of the population is estimated to have access to a community pharmacy within 20 min walk. For urban areas, that is 98.3% of the population, for town and fringe, 79.9% of the population, while for rural areas, 18.9% of the population. For areas of lowest deprivation (deprivation decile 1) 90.2% of the population have access to a community pharmacy within 20 min walk, compared to 99.8% in areas of highest deprivation (deprivation decile 10), a percentage difference of 9.6% (8.2, 10.9).
Conclusions Our study shows that the majority of the population can access a community pharmacy within 20 min walk and crucially, access is greater in areas of highest deprivation—a positive pharmacy care law. More research is needed to explore the perceptions and experiences of people—from various levels of deprivation—around the accessibility of community pharmacy services.
- PUBLIC HEALTH
- Pharmacies
- health services accessibility
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
Our study is the first to systematically examine whether there is an inverse care law in relation to community pharmacies and the first to analyse geographical access to services in England.
-
A key strength of this study is that we examined accessibility of community pharmacies by walking distance; the cost of driving and using public transport can be significant barriers to travel and, as such, may not give a true account of community pharmacy accessibility.
-
A possible limitation is that a 20 min walk from each community pharmacy was represented using a straight-line distance from the central point of each pharmacy's postcode to create a buffer. This assumes people walk in straight lines while, in reality, people are constrained to pathways that curve or are sometimes cut-off by barriers.
Background
The role of the community pharmacist has undergone rapid expansion in recent years with a significant emphasis now placed on delivering patient-focused services, including promoting healthy lifestyles and modification of health-related behaviours, as well as providing medicine-related activities.1 ,2 This change has been acknowledged in England through the National Health Service (NHS) contractual framework for community pharmacy, which has three distinct levels of service: essential, advanced and locally commissioned.3 The essential and advanced levels of service are provided by all community pharmacies in England and include dispensing medication and providing medicine use reviews, while the locally commissioned services are provided in response to needs of the local population. As such, many community pharmacies now offer services, commissioned by local authorities according to need, which are designed to help address public health priorities including smoking, alcohol misuse and obesity.4 These issues were identified by The Strategic Review of Health Inequalities in England (the Marmot Review) as significant modifiable risk factors for inequalities in morbidity and mortality in England.5 ,6 It is clear from the Marmot Review and other research that the way in which society is organised causes inequalities in these conditions, and inequalities in these conditions are, in turn, major contributions to overall inequalities in health, morbidity and mortality. Significantly, more people die from these conditions in disadvantaged areas compared to more affluent ones.7–9 Access to healthcare services is a well-established social determinant of health: disadvantaged areas often lack access to the level of NHS services that their health needs require (such as primary care services). This has been termed as an Inverse Care Law, as proposed by Tudor Hart in 1971, who stated “the availability of good medical care tends to vary inversely with the need for it in the population served”.10
Rural areas are often disadvantaged in accessing healthcare services such as general practitioner (GP) practices. Previous studies show that a ‘distance decay’ effect operates in accessing healthcare services in rural areas, with GP consultation rates declining as the distance from the GP surgery increases.11–13 There is a common perception that people in rural areas are more affluent and therefore healthier than their urban counterparts, with a greater ability to adapt to and access increasingly urbanised health services.14 ,15 For the older population, who tend to have greater healthcare needs accessing healthcare services may not be so easy, particularly those in rural areas where there may be a lack of suitable transport.16
Community pharmacies have, to date, been overlooked in discussions around access to care, even though they could potentially make a significant contribution to this issue as there are over 12 000 community pharmacies in England, distributed across urban/rural and deprived/affluent areas. Estimates vary with regard to the reach of this community pharmacy network, but some sources suggest over 90% of the population makes at least one visit to the pharmacy per year.17 ,18 Evidence also suggests that a range of patients—of varying age, gender and social class—visit community pharmacies every month to collect prescriptions, purchase over-the-counter medicine and obtain general healthcare advice.19 Community pharmacies therefore appear to be uniquely placed to deliver healthcare initiatives and can also be accessed without the patient needing a prior appointment. This accessibility has consistently improved in recent years with policy drivers to improve access to medicines—including the promotion of ‘self-care’—with the introduction of ‘100 hour pharmacies’, which must open 100 h per week, for every week of the year. However, it is not understood if community pharmacies offer easy and equitable access to healthcare and therefore contribute to, or ameliorate, the inverse care law. Clearly, as with other healthcare services, for community pharmacy services to be successful and to contribute to reducing inequalities in health, it is vital for these services to be available to the areas and patient populations that need them most. This study, therefore, aims to: (1) determine the percentage of the population in England that have access to a community pharmacy within 20 min walk; (2) explore any relationship between the walking distance (the accessibility) and urbanity; (3) explore any relationship between the walking distance and social deprivation and (4) explore any interactions between urbanity, social deprivation and pharmacy access. The study is the first to examine whether there is an inverse care law in relation to community pharmacies and the first to analyse geographical access to services in England.
Methods
Study design
This study explores the relationship between spatial access to community pharmacies, deprivation and urbanity using geographical information systems and generalised linear models.
Outcome
The percentage of the population that had access to a community pharmacy within a 20 min walk by lower super output area (LSOA): measured as a straight line distance from each pharmacy (1.6 km buffers) and aggregating the population by postcode within each buffer compared to the LSOA population.
Definitions
Community pharmacy: Registered with the General Pharmaceutical Council as premises for the compounding, procurement, storage and distribution of medicines and appliances; we excluded premises that were solely registered as Internet pharmacies in the analysis.
LSOA: Geographic areas in England comprising of approximately 1500 residents and 650 households. They are designed to be of a reasonably compact shape while being representative of social homogeneity.20
Urban/rural Ccassification: Categorises each LSOA into three settlement types: urban (where the population is over 10 000 people), town and fringe (part of a settlement with less than 10 000 people) or village, hamlet and isolated dwellings.21
Deprivation decile: The term ‘deprivation decile’ is used to group the population into 10 equally spaced ordinal categories according to a particular level of deprivation.
Data and variables
Data were obtained from the Fuse Geo-HealthCare Database. This database contains data on the address and postcode of each community pharmacy in England (obtained from the General Pharmaceutical Council—the independent regulator for pharmacists, pharmacy technicians and pharmacy premises in Great Britain)22; the postcode of each community pharmacy (matched to their corresponding coordinates using the Office of National Statistics postcode directory, 2012)23; the coordinates for each postcode in England (also from the Office of National Statistics postcode directory, 2012—matched to a population lookup table and the LSOA for each postcode); whether the LSOA is urban (where the population is over 10 000 people), town and fringe (part of a settlement with less than 10 000 people) or village, hamlet and isolated dwellings from the urban/rural classification (2005)21 and the Index of Multiple Deprivation score (2010) for each LSOA (from the Office of National Statistics).24 More details on the Fuse Geo-HealthCare Database are available here: https://www.dur.ac.uk/wolfson.institute/geohealth/
Analysis
The community pharmacy postcodes for England were mapped using ArcMap. The average person walks 1 mile (1.6 km) in 20 min,25 therefore 1.6 Km buffers were placed around each pharmacy to represent a 20 min walk from a community pharmacy. The population postcodes were then clipped to the pharmacy buffers. Data on the sum of the population for each LSOA overall and within each community pharmacy buffer was extracted by LSOA. The percentage of the population with access to a pharmacy within 20 min walk was then calculated by LSOA. Whether or not the LSOA was urban, town and fringe or rural and the corresponding deprivation score was attached to the data file. Deprivation deciles were also calculated. The most deprived decile (10) equates to the most deprived 10% within a population, while the least deprived decile (1) represents the 10% of a population living in the least deprived circumstances. Each data set was then mapped using Arc GIS. Tables were produced to show the percentage of the population who had access to a pharmacy within 20 min walk by deprivation decile and by urban/rural classification within the deprivation deciles. Generalised linear models were used to adjust for rurality within each deprivation decile to produce urban/rural adjusted prevalence rates of the percentage of households with access to a pharmacy within 20 min walk by LSOA and the results tabulated.
Results
Urban rural/deprivation decile access
Data for all of the LSOAs in England shows that 89.2% of the population has access to a community pharmacy within 20 min walk. In total 98.3% of the households in the urban areas are estimated to have access to a pharmacy within 20 min walk. In town and fringe, the percentage of households that have access to a community pharmacy is estimated as 79.9% while the percentage of those in the rural areas is estimated as 18.9%.
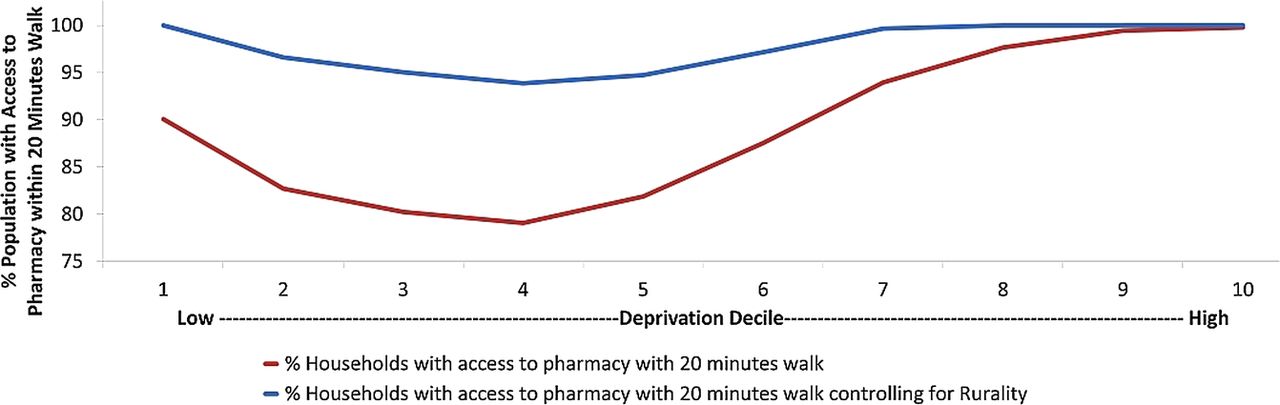
The distributions of percentages of households with access to a community pharmacy within 20 min are presented in table 1 (and shown spatially in figures 1 and 2) according to their deprivation decile and urban, town and fringe and rural areas. There is a significant non-linear association between the deprivation deciles (a u-shaped access curve, see figure 3): the least deprived and most deprived households have more access to a pharmacy than the households in the middle of the deprivation range. Overall, the inequalities in access to pharmacies in England range between 0.3% less and 20.2% less access when compared to the most deprived areas. There are higher spatial inequalities in access in rural areas with ranges of 6.7–30.4% less access in comparison to 3.5–26.2% for town and fringe, and 0.1–3.7% for urban areas—spatial inequalities in access are thus much smaller in urban areas.
The percentage of the population with access to a community pharmacy within a 20 min walk by urbanity and deprivation decile (with 95% CIs)

Map of England with LSOA stratified according to deprivation.

Map of England showing the population within 20 minutes walk of a community pharmacy.

{kind=link}
{kind=link}
{kind=link}
Percentage of the population with access to a pharmacy within 20 min’ walk by deprivation decile before and after adjusting for Urbanity.
Urban areas have the least difference between the most and least deprived LSOAs with only 3.7% less of the population having access to a pharmacy within 20 min’ walk in the least deprived LSOAs. In town and fringe LSOAs this rose to 17.9% difference, while in rural areas there was no significant difference between the least and most deprived LSOAs.
Overall, there is a clear dose—response relationship between access to community pharmacies and urbanity levels. Specifically, the urban areas have more access to community pharmacies, followed by town/fringe while the rural areas have the least access to pharmacies—regardless of deprivation.
After controlling for the effects of rurality, only two deprivation deciles have marginally below 95% of the population being able to walk to a community pharmacy within 20 min.
Discussion
Principal findings of this study
The data has shown that 89% of the population in England has access to a community pharmacy within 20 min walk. Crucially, there is a positive trend between community pharmacy accessibility and deprivation decile—with the highest access in the most deprived areas—showing there is no inverse pharmacy law for community pharmacy distribution in England. Indeed we have found evidence of a positive pharmacy care law. Populations in urban areas of England also have better access to a community pharmacy, compared to populations in town and fringe and rural areas.
Strengths and weaknesses
This study sought to explore the accessibility of community pharmacies in England by walking distance: this is a key strength. We deliberately did not seek to explore accessibility by car or by using public transport, as we feel this would not give a true picture of accessibility for patients living in more deprived areas. Indeed, as access to a car is linked to income—with households in underprivileged areas having less access26—it is conceivable that this may be more of a significant barrier for patients living in deprived areas if the pharmacy was only accessible by driving; similarly, for public transport, the cost of using such services may prove to be a barrier to households with low incomes.27 In terms of study limitations, while we believe our results are robust and have important implications for the commissioning of healthcare services from community pharmacy settings, we acknowledge that, in the analysis, we did not consider the individual services offered from each community pharmacy, which may show some local variability due to current commissioning systems. We also acknowledge that our work only explores accessibility from a geographical viewpoint and not a social perspective. Indeed, just because a community pharmacy offers a healthcare service and is within walking distance of a particular household does not necessarily mean that people perceive them as valuable or would be willing to access the service. A study exploring the perceptions and experiences of people—from various levels of deprivation—around the accessibility of community pharmacy services is therefore warranted. In terms of a methodological viewpoint, we recognise a 20-min walk from each community pharmacy was represented using a straight-line distance from the central point of each pharmacy's postcode to create a buffer. This assumes people are able to walk in any direction from that postcode and always in a straight line. In reality people are constrained to pathways that may curve, or even be cut off by barriers. A further limitation is that of the postcodes themselves. An individual postcode represents an average of 15 addresses, with the coordinates of each postcode being represented using the geographic centroid of each postcode. Particularly in rural areas, where houses are more sparsely spread, this could ostensibly mean that some households will fall outside of a pharmacy buffer, when in fact this is not the case for some addresses. Equally, however, some addresses will fall inside a buffer, so, over a large population, one would expect this issue to even out.
What is already known?
There have been several mapping studies published exploring the distribution and accessibility of community pharmacies in areas of America and Canada. For example, a study by Lin (2004) explored the accessibility of community pharmacies by elderly patients in Illinois and sought to estimate the disparity between urban and rural areas. The study found that, on average, there were 1.27 and 0.38 pharmacies per 10 000 people in urban and rural areas, respectively. In terms of accessibility, the average distance for an elderly patient was 0.9 miles in urban areas but significantly higher at 5.9 miles in rural areas.28 While Law et al,29 examined the geographical access to community pharmacies in Ontario and found over 60% of the population reside within walking distance of at least one community pharmacy. Our original work shows geographical accessibility is even higher in England. Despite studies published concerning community pharmacies in America and Canada, there has been no study published in the literature that has explored accessibility of community pharmacies in England. The recent White Paper Pharmacy in England: Building on Strengths—delivering the future, published by the Department of Health in 2008, claimed that, in England, 99% of the population can get to a pharmacy within 20 min by car and 96% by walking or using public transport.2 However, while our report supports this finding to some extent, it was not clear which methodological approach was used to obtain this result, as, to the authors knowledge, no supporting data were published outlining methodology; and—crucially—the Department of Health report did not assess how varying levels of social deprivation influence the accessibility to a community pharmacy. In addition, since the publication of the White Paper and report, many more community pharmacies have since been opened in England. Opening a new community pharmacy can be a complex process, as new applications made to NHS England are assessed against a Pharmaceutical Needs Assessment for a particular area30—with areas of the most need having a higher probability of a new application being granted. It is, however, unlikely that the control of entry criteria can fully explain our findings in relation to community pharmacy distribution, as these regulations change over time and often have exemptions (eg, up until recently 100 h community pharmacies were exempt from the criteria).
Previous research has shown that healthcare interventions delivered by community pharmacies are accessible. By way of example, several small-scale studies have compared accessibility of emergency hormonal contraception (EHC) from a community pharmacy setting to other healthcare providers. These studies have shown that women who went to a community pharmacy had more rapid access to EHC, compared to other settings, such as family planning clinics.31 ,32 Given that the effectiveness of EHC is related to how quickly it is taken after unprotected sexual intercourse this may prove to have a significant clinical benefit. Other studies, rather than explore accessibility as such, have used community pharmacies to target healthcare interventions towards ‘hard to reach’ areas. For example, Murphy et al,33 showed community pharmacies are convenient and accessible, and can provide influenza vaccination programmes in medically underserved communities, while Kellow34 successfully delivered a community pharmacy weight management programme to young adults in a rural setting. These studies demonstrate the potential for community pharmacies to deliver healthcare interventions to areas of the greatest need.
Implications for policymakers
This is the first study to systematically explore the spatial distribution of community pharmacies in England. It is also the first study that examines the relationship between accessibility of community pharmacies and social deprivation and to explore the idea of an inverse pharmacy care law. The paper shows that community pharmacies are easily accessible by the majority of the population in England, with 89% able access a community pharmacy within 20 min walk. Our study also shows that there is no inverse pharmacy law for community pharmacies in England: access to a community pharmacy is greater in areas of higher deprivation compared to more affluent areas—a positive pharmacy care law. This is a very timely finding as a recent initiative led by NHS England—the Call to Action—is seeking to develop local strategy for community pharmacy initiatives and inform strategic policy making in terms of commissioning community pharmacy services.35 Our work supports this initiative and shows that community pharmacies are uniquely placed in the community to deliver healthcare interventions. In addition, as the accessibility of community pharmacies is greatest in areas of highest deprivation, they may have an important role to play in reducing inequalities in priority public health conditions in England.
Conclusions
Community pharmacies have the potential to offer convenient and equitable access to healthcare. The vast majority of households in England—and especially those in the most deprived areas—have access to a community pharmacy within 20 min walk: a positive pharmacy care law. This potentially has major implications for the commissioning of future services from community pharmacies in England.
Footnotes
-
Contributors AT and CB conceptualised and designed the study and were involved in methodological development, analysis and interpretation. AC, AK and AH were involved in the development of the methods, data analysis and interpretation. AT led the drafting of the manuscript with input from all authors. All authors approved the final version and AT has responsibility for its final content.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement All of the primary data sources used to compile the database for this study are referenced within the manuscript. We are unable to share the study database but information related to it is available at: https://www.dur.ac.uk/wolfson.institute/geohealth/. The final raw analysed data is available by e-mailing AT (adam.todd@durham.ac.uk).