Article Text

Abstract
Objective To evaluate the safety profile of nicergoline compared with placebo and other active agents from published randomised controlled trials.
Design Systematic review and meta-analysis of nicergoline compared with placebo and other active agents across various indications.
Data sources MEDLINE, Medline-in-process, Cochrane, EMBASE, EMBASE alerts, Cochrane Central Register of Controlled Trials (CENTRAL), Cochrane Database of Systematic Reviews (CDSR) and Cochrane Methodology Register (CMR) for all the randomised controlled trials, open-label or blinded, in adults treated with nicergoline. Studies published until August 2013 were included.
Review method 29 studies were included for data extraction. The studies included in this review were majorly from European countries and mostly in cerebrovascular disease (n=15) and dementia (n=8).
Results The treatment withdrawals were comparatively lower in the nicergoline group as compared with the placebo group (RR=0.92; 95% CI 0.7 to 1.21) and other active comparators (RR=0.45; 95% CI 0.10 to 1.95), but the difference was non-significant. Incidence of any adverse events (AEs) was slightly higher (RR=1.05; 95% CI 0.93 to 1.2) while incidence of serious AEs was lower (RR=0.85; 95% CI 0.50 to 1.45) in the nicergoline compared with placebo group. Frequency of anxiety was significantly lower in nicergoline as compared with placebo (p=0.01). Other AEs including diarrhoea, gastric upset, dizziness and drowsiness were less frequent in the nicergoline group when compared with placebo/active drugs, but the difference was non-significant. Frequency of hypotension and hot flushes was slightly higher in the nicergoline group but the difference was non-significant. None of the studies reported any incidence of fibrosis or ergotism with nicergoline treatment.
Conclusions Nicergoline is an ergot derivative, but its safety profile is better than other ergot derivatives like ergotamine and ergotoxine. This systematic review and meta-analysis suggests that nicergoline has a good safety profile. None of the studies included in this systematic review reported any incidence of fibrosis or ergotism with nicergoline.
- Meta-analysis
- Nicergoline
- Ergot derivatives
- Fibrosis
- Ergotism
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
First meta-analysis on nicergoline to understand the adverse clinical profile.
-
Critical in wake of recent European Medicines Agency's (EMEA) view of blanket limitation on use of all ergot derivatives.
-
Limited by the availability of long-term (more than 2 years) and high-dose studies for cognitive impairment.
Background
Nicergoline is a semisynthetic ergot derivative which has been registered in over 50 countries and has been used for more than four decades for the treatment of cognitive, affective and behavioural disorders in older people.1 During the time it has been in use, the rationale for its clinical use has evolved. Initially regarded as a vasoactive drug, it was mainly prescribed for cerebrovascular disorders. Although cholinergic deficits are the major current targets for pharmacological intervention in Alzheimer's dementia, a wide variety of other neurotransmitter changes can be identified in the disease.
Nicergoline has been demonstrated to increase the availability of acetylcholine through an increased release from cholinergic terminals and a selective inhibition of acetyl cholinesterase.2 Nicergoline may also enhance norepinephrine and dopamine turnover in some areas of the brain.3 Nicergoline has a positive effect on the signal transduction system stimulating the phosphoinositide pathway which is specifically impaired in Alzheimer's dementia.4 Other useful actions of nicergoline in dementia are an increase of phosphoinositide-protein kinase C (PKC) translocation which helps in combating β-amyloid deposition and in retarding the reduction in nerve-growth factor which may help in preventing the loss of cholinergic neurons.4
The side effects of nicergoline are usually limited to nausea, hot flushes, mild gastric upset, hypotension and dizziness. At high dosages bradycardia, increased appetite, agitation, diarrhoea and perspiration have been known to occur. Nicergoline has a better safety profile compared with ergot derivates which are associated with increased risk of fibrosis (formation of excess connective tissue that can damage organs and body structures) and ergotism (symptoms of ergot poisoning, such as spasms and obstructed blood circulation) with these medicines.
Nicergoline is not associated with either fibrosis or ergotism; however, concerns about its safety have been raised, especially after the European Medicines Agency's (EMEA) restriction on nicergoline, because it is an ergot derivative.5 Most of the available literature suggests that the adverse events (AEs) with nicergoline are mild and transient. Hence, a systematic review of literature and meta-analysis was conducted to compare the safety profile of nicergoline with placebo and other active comparators.
Methods
Search strategy
A comprehensive search strategy was designed to retrieve relevant clinical data from published literature. The following databases were examined since inception up to 16 August 2013; MEDLINE, Medline-in-process, EMBASE, EMBASE alerts, Cochrane Central Register of Controlled Trials (CENTRAL), Cochrane Database of Systematic Reviews (CDSR) and Cochrane Methodology Register. Medical subject headings (MeSH terms) and free keywords like “randomised controlled trial”, “Nicergoline”, “Adverse effects”, “toxicity” and “side effects” were used (see online supplementary appendix 1). This review was not restricted to studies conducted in the English language and hence studies published in other languages were also included and translated for data extraction.
Selection criteria
To meet the study objective, we predecided on inclusion criteria which include randomised controlled trials (RCTs) reporting AEs in patients undergoing nicergoline treatment for psychiatric disorders. To be included in the analysis, a trial had to fulfil the following criteria: (1) randomised trials which could be open-label, single-blind or double-blind, parallel group studies; (2) use of nicergoline for Alzheimer's disease, dementia or cognitive disorders; (3) use of nicergoline as one of the interventions; (4) studies comparing nicergoline with ergot derivatives, placebo or other active agents were included and (5) studies should report safety and tolerability data for nicergoline.
Studies were excluded if: (1) they presented data on children only; (2) study design was not of interest; (3) disease was other than of interest; (4) study was not presenting safety and tolerability outcomes and (5) full text could not be sourced.
Data extraction
Bibliographic details and abstracts of all citations retrieved by the literature search were downloaded into Endnotes V.X3. Cochrane methodology was used to conduct this systematic review. All studies were screened by two independent reviewers with discrepancies resolved by a third reviewer.
Study quality and risk of bias
The Jadad score was used to assess the quality of included studies. Risk of bias in the individual studies included for meta-analysis was assessed using the Cochrane risk assessment tool.6
Outcomes assessed
In most of the included studies, safety evaluation included monitoring of AEs, vital signs, haematology and blood chemistry. Haematology and blood chemistry were assessed at baseline and at the last assessment. Tolerability evaluation included monitoring of treatment-emergent AEs (elicited or observed); physical examination including ECG recording; vital signs, haematology and blood chemistry testing. Withdrawals, due to any reason or due to AE, were reported.
The data from these studies were pooled for total withdrawals, withdrawals due to AEs, incidence rates for any AEs, serious AEs (SAEs) and specific AEs including anxiety, constipation, diarrhoea, hot flushes, itching, gastric upset, hypotension, headache, dizziness, insomnia, drowsiness and fatigue. Only studies which presented data for same comparators were included in direct meta-analysis for each outcome.
Statistical analysis
Comparison of safety and tolerability outcomes was made between interventions by pooling data from studies using a direct meta-analysis technique. Only head-to-head comparisons between interventions were included for meta-analysis. Review Manager (RevMan V.5.1) software was used for meta-analysis of the available data. Dichotomous outcomes were summarised as risk (relative) ratios.
Results
Study selection
A trial flow of the review process (as per PRISMA statement) is presented along with manuscript (figure 1). The search of the literature yielded 437 separate references. Owing to the overlap of coverage between the databases, 96 of the references were found to be duplicates. A total of 341 citations were reviewed for abstract screening (first pass). Following the first pass of the citations, 56 potentially relevant references were identified. Full-text reports of these citations were obtained for more detailed evaluation. Following detailed examination of the reports, 26 citations were excluded. Thirty studies met inclusion criteria; however, one of them was a secondary publication which was linked to its primary publication. Finally, a total of 29 references reporting trials were extracted. Table 1 presents an overview of the study methods in included studies. Fifteen studies were not included in meta-analysis as data from these could not be pooled. These were studies reporting stand-alone AEs, or for stand-alone comparators.
Study methods for included randomised controlled trials

PRISMA flow for included studies.
Baseline characteristics
Most of the included studies were in cerebrovascular disease (n=15), followed by dementia (n=8). Two studies were for Alzheimer’s disease and four were in other disease areas. The mean age of included patients ranged from 4817 to 81 years32 across the studies. The percentage of male patients ranged from 17.9%32 to 76.7%26 in the nicergoline group and was comparable with the control group in all studies. The number of patients randomised in these studies ranged from 1631 to 34634. The treatment/study duration ranged from 6 days31 to 24 months11 across included studies with most studies with duration ≥3 months (n=17). The daily dose of nicergoline used was ≤30 mg/day in 16 studies and was reported to be 60 mg/daily in 12 studies.
Critical appraisal
Included studies were critically appraised using the Jadad scale which is a standard scale used for evaluating the quality of randomised trials in systematic reviews. Methods used to generate random allocation sequences were reported in only nine of the included studies and were judged as adequate. The Jadad score was ≥3 in 20 studies and less than 3 in 9 studies. The majority of the studies were good quality studies as per the Jadad scale. All of the included studies reported comparable baseline characteristics between treatment groups being studied.
Risk of bias assessment
The risk of bias was low in the individual studies that were included for meta-analysis. The method used to generate the allocation sequence was reported in sufficient detail to allow an assessment in most of the studies. None of the included studies reported any inadequate method. The method used for allocation concealment was not reported by any of the included studies. The method used for blinding was adequate in most of the studies reporting it. Studies of withdrawals and patients’ inclusion for outcome assessments were similar within study groups.
Withdrawals
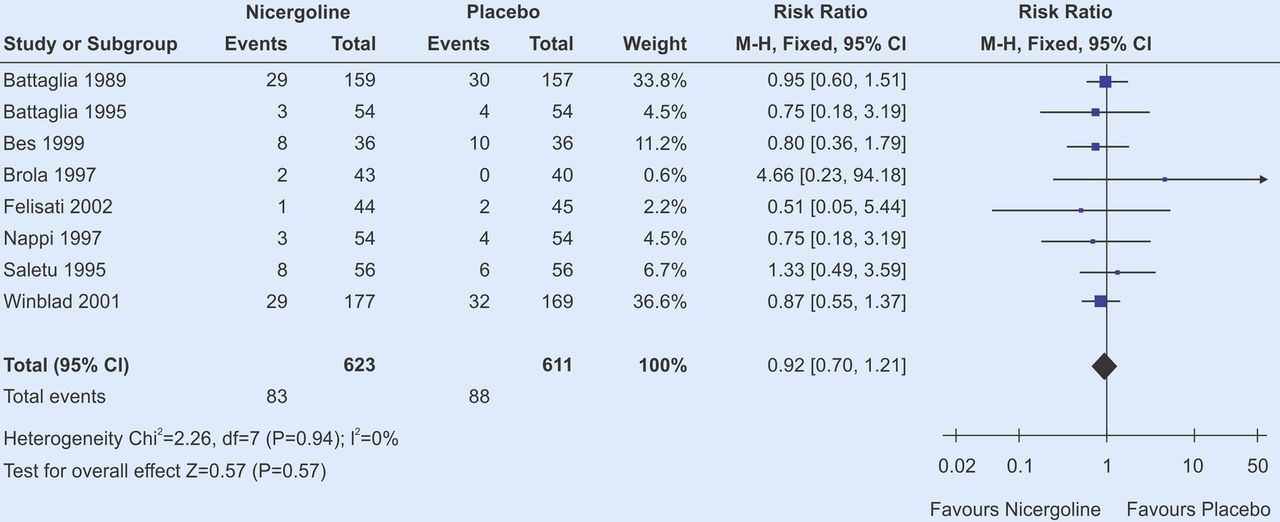
Total withdrawals with nicergoline ranged from 0%22 ,25 to 22.2%11 and from 0% to 27.8% with other comparator drugs/placebo. Six studies reported a lower number of patient withdrawals from the nicergoline group as compared with other comparator/placebo groups. Withdrawals due to AE were similar in the nicergoline group as compared with other groups across the studies (figure 2).
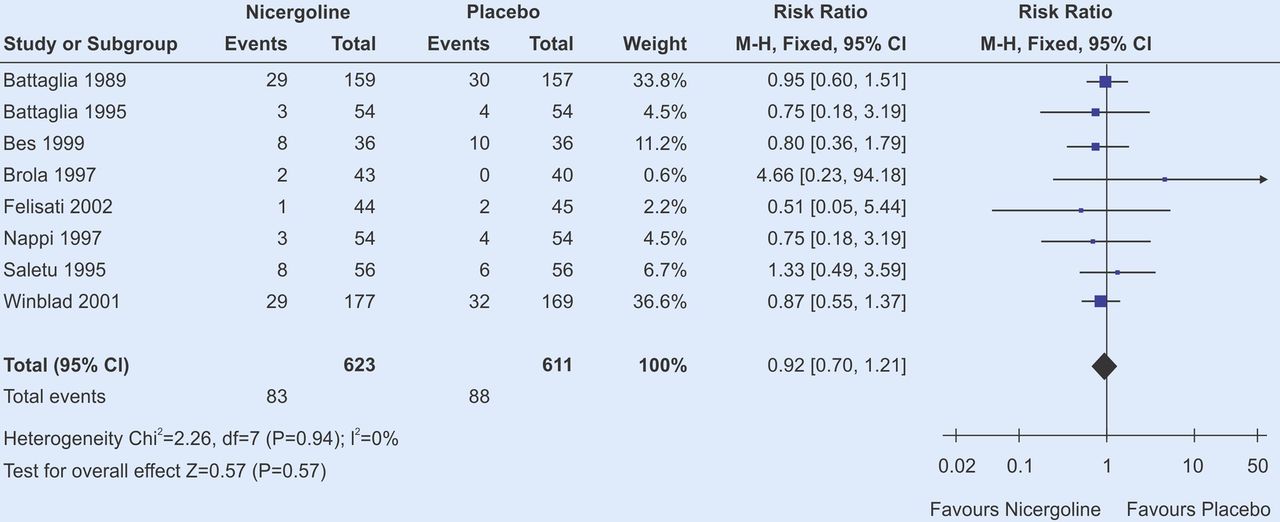
Results of meta-analysis, all withdrawals: nicergoline versus placebo.
The meta-analysed risk ratios between nicergoline and the other comparators and their corresponding 95% CIs for study withdrawals are shown in tables 2. Results of meta-analysis showed a non-significant lower rate of withdrawals from nicergoline compared with placebo (p=0.57) and other active agents (p=0.28). For withdrawals due to AE, the withdrawal rate was slightly higher with nicergoline when compared with placebo but the difference was only apparent and non-significant (p=0.7).
Meta-analysis of withdrawal rate across included studies
Adverse events
There were adequate data to perform meta-analysis for safety outcomes including any AE, SAE, diarrhoea, hot flushes, gastric upset, itching, hypertension, headache, dizziness, anxiety, insomnia, drowsiness and fatigue (see online supplementary table S1). However, there was no reference to cases with fibrosis and/or ergotism.
The meta-analysed risk ratios between nicergoline and other comparators and their corresponding 95% CIs for study withdrawals and safety outcomes are shown in tables 2 and 3, respectively. Results of meta-analysis showed a non-significant lower rate of withdrawals from nicergoline compared with placebo (p=0.57) and other active agents (p=0.28). For withdrawals due to AE, the withdrawal rate was slightly higher with nicergoline when compared with placebo but again the difference was non-significant (p=0.7).
Meta-analysis of overall AEs
The risk of any AE was similar with nicergoline compared with placebo (10 studies), ergot derivatives and other active comparators, all comparisons being non-significant. Risk of any SAE was slightly lower in the nicergoline group compared with placebo, but was non-significant. A significantly lower risk of agitation/anxiety was reported with nicergoline as compared with placebo (p=0.01). Nicergoline was associated with a lower risk of diarrhoea as compared with placebo or ergot derivatives, with both comparisons being non-significant. The incidence of dizziness was similar in the nicergoline group as compared with placebo or other active agents. A comparatively lower risk of drowsiness was reported with nicergoline compared with placebo but the difference was non-significant. Risk of gastric upset was similar in the nicergoline and placebo groups.
Higher risk of fatigue was associated with nicergoline compared with active comparators including ergot derivatives but the difference was non-significant. Higher risk of hot flushes was reported with nicergoline compared with other comparators. Risk of headache and hypotension was higher with nicergoline compared with placebo. Higher risk of insomnia and itching was reported with nicergoline. For none of the AEs, where risk was higher for the nicergoline group, was any significant difference observed compared with the other intervention or placebo (figure 3).

{kind=link}
{kind=link}
{kind=link}
Results of meta-analysis, any adverse events: nicergoline versus placebo.
Of the 14 studies included in the qualitative analysis, no incidence of AEs was reported in 8 studies during the entire study duration, while remaining studies reported excellent or good tolerability in nicergoline treated patients. None of these studies reported any incidence of ergotism or fibrosis with nicergoline.
Discussion
Nicergoline is a potent and selective α-1A adrenergic receptor antagonist.36 Nicergoline is reported to enhance catecholaminergic turnover,3 stimulate cholinergic neurotransmission,4 stimulate the phosphoinositide pathway,3 promote cerebral metabolic activity37 and has neuroprotective and antioxidant properties.38 Nicergoline is used clinically to improve the apathy and affective disorders caused by cerebral infarction (such as reduced mental alertness, inattention, impairment of recent memory, hypobulia, depression, etc). It is useful in the treatment of acute and chronic peripheral circulation disorders (such as obliterative vascular disease of the limbs, Raynaud's syndrome and other peripheral circulation dysfunction symptoms). Nicergoline has also been prescribed for the treatment of vascular dementia, especially for the improvement in cognitive dysfunction and memory, and to reduce the severity of this disease.
In addition, studies have been reported showing the usefulness of nicergoline in conditions such as posthaemodialysis pruritus, tinnitus and vertigo, ocular conditions such as arterial obstructions, venous thrombosis, diabetic retinopathies, senile macular degenerations, papilla ischaemic oedema and central serous chorioretinopathies. Dosages for known conditions are usually administered at 5–10 mg three times a day, however antiaging preventative purposes may limit this to 5 mg once or twice a day. Higher doses of up to 60 mg/day have also been prescribed in clinical practice but have been associated with increased risk of AEs.4
The EMEA's Committee for Medicinal Products for Human Use (CHMP), in its recommendations, has suggested that ergot containing medicines, including nicergoline, should no longer be used to treat conditions involving blood circulation problems (such as peripheral artery disease, Raynaud's syndrome and retinopathies of vascular origin), memory and sensation problems and migraine headaches. This recommendation has been supported by the EMEA citing that these ergot derivatives have a high likelihood of causing SAEs such as fibrosis and ergotism.5 However, in this recommendation, the EMEA suggests that healthcare professionals can continue prescribing nicergoline and other ergot derivatives in dementia (including Alzheimer's disease) and acute migraine.
Nicergoline has proven efficacy in the treatment of senile dementia of Alzheimer type and multi-infarct dementia.1 ,32 Also, nicergoline has shown efficacy in conditions like posthaemodialysis pruritus,39 tinnitus and vertigo.40 Nicergoline has a positive effect on cognition and behaviour in addition to an effect on clinical global impression in older patients with mild-to-moderate cognitive and behavioural impairment of various clinical origins including chronic cerebrovascular disorders and Alzheimer's dementia.1
Nicergoline has been reported to cause central nervous system disturbances including diaphoresis, sleep disturbances, fainting, agitation, drowsiness, dizziness, insomnia, restlessness, flushing and increased appetite.8 ,22 Cardiovascular events like temporary rise in blood pressure, syncope, bradycardia and hypotension have been reported with nicergoline in a few studies.18 ,41
Nicergoline has been known to cause minor gastrointestinal side effects such as heartburn and abdominal pain, gastric pain, pyrosis, vomiting and diarrhoea. Various studies have reported other minor effects with nicergoline including hot flushes, dizziness, ejaculation failure and interstitial nephritis.42 ,43
Results of this meta-analysis showed the comparable safety profile of nicergoline with other active agents (including ergot derivatives) and placebo. The withdrawal rates and withdrawal due to AEs were similar with nicergoline compared with placebo and active agents. Incidence of any AE when compared with placebo and ergot derivatives was slightly higher in the nicergoline group but the difference was non-significant. Significantly lower rates of anxiety were reported with nicergoline compared with placebo (p=0.01). Incidence of AEs such as diarrhoea, dizziness, drowsiness, gastric upset and fatigue was slightly lower with nicergoline as compared with placebo but the difference was non-significant for all comparisons.
Nicergoline was associated with higher rates of hot flushes, headache, hypotension, insomnia and itching. None of the comparisons showed a significant difference, but some of these AEs are probably because of the vasodilation action of nicergoline. Higher doses of nicergoline (60 mg/day) were associated with higher rates of AEs compared with the 30 mg/day dosing, but the difference was not significant. None of the studies included in this meta-analysis reported any incidence of fibrosis or ergotism with nicergoline.
In its current recommendation, the EMEA has overlooked the efficacy and safety profile of nicergoline and has cautioned against its use in conditions with blood circulation problems, memory and sensation problems and migraine headaches. The CHMP at EMEA suggested a ban on use of ergot derivatives as they have been associated with fibrosis and ergotism. The EMEA has probably considered the safety profile of all ergot derivatives as similar. The CHMP review has reported highest incidence of fibrosis and ergotism with dihydroergotamine and suggests incidence of these AEs with other ergot derivatives as well.
EMEA has suggested that echocardiography should be performed within 3–6 months of starting treatment with ergot derivatives and subsequently at 6–12-month interval.44 In the current meta-analysis, most of the included studies were >3 and up to 24 months in duration and none of the included studies reported any incidence of fibrosis or ergotism with nicergoline. There is no evidence in literature to suggest any incidence of fibrosis and ergotism with nicergoline.
The strengths of this systematic review include the clear definition of the research question, adherence to an explicit research protocol that was developed prior to the analysis, the comprehensive nature of the data search (employing electronic databases and manual bibliography searches resulting in the inclusion of all relevant publications), consensus between two reviewers of all data elements prior to entry into the database and the quality control review of every element of this report. In addition, the quality of the studies and manuscripts used to provide data was relatively high. Only RCTs were included in this systematic review/meta-analysis. The main limitation of this meta-analysis is the scarcity of head-to-head trials to compare the safety of nicergoline with other ergot derivatives. Another possible limitation of this review could be the publication timeframe of the included studies. Most of the studies were published in the 1980s and 1990s. There were hardly any trials published in recent years on safety evaluation for nicergoline.
Conclusions
This systematic review and meta-analysis has included the evidence to date with regard to tolerability and safety of nicergoline as reported by RCTs. Nicergoline is categorised under ergot derivatives. However, the AEs with nicergoline are mild and transient unlike other ergot derivatives (ergotamine and ergotoxine) which have been associated with fibrosis and ergotism.
The results from this systematic review/meta-analysis suggest that nicergoline has a comparable safety profile as placebo and other active comparators. None of the studies included in this systematic review reported any incidence of fibrosis or ergotism with nicergoline. The evidence generated by this review suggests that despite being an ergot derivative, nicergoline is a safe and well-tolerated drug. This systematic review/meta-analysis concludes that nicergoline is a safe option for therapeutic management in patients with dementia and cerebrovascular disorders.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
- Data supplement 2 - Online table
Footnotes
-
Contributors AG carried out the searches in various databases. AG and JX carried out the filtration of citation and data extraction. MF and TN helped to draft the manuscript and reviewed it. All authors read and approved the final manuscript.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement In addition to the manuscript, the corresponding author also has initial results of publication analysis. That explains the reason for inclusion and exclusion of individual studies. If readers require additional data on the analysis or the medical merits of the molecule, they can write to amitgarg.pharm@gmail.com.