Article Text

Abstract
Objectives To conduct a systematic review of randomised controlled trials (RCTs) examining the use of social media to promote healthy diet and exercise in the general population.
Data sources MEDLINE, CENTRAL, ERIC, PubMed, CINAHL, Academic Search Complete, Alt Health Watch, Health Source, Communication and Mass Media Complete, Web of Knowledge and ProQuest Dissertation and Thesis (2000–2013).
Study eligibility criteria RCTs of social media interventions promoting healthy diet and exercise behaviours in the general population were eligible. Interventions using social media, alone or as part of a complex intervention, were included.
Study appraisal and synthesis Study quality was assessed using the Cochrane Risk of Bias Tool. We describe the studies according to the target populations, objectives and nature of interventions, outcomes examined, and results and conclusions. We extracted data on the primary and secondary outcomes examined in each study. Where the same outcome was assessed in at least three studies, we combined data in a meta-analysis.
Results 22 studies were included. Participants were typically middle-aged Caucasian women of mid-to-high socioeconomic status. There were a variety of interventions, comparison groups and outcomes. All studies showed a decrease in programme usage throughout the intervention period. Overall, no significant differences were found for primary outcomes which varied across studies. Meta-analysis showed no significant differences in changes in physical activity (standardised mean difference (SMD) 0.13 (95% CI −0.04 to 0.30), 12 studies) and weight (SMD −0.00 (95% CI −0.19 to 0.19), 10 studies); however, pooled results from five studies showed a significant decrease in dietary fat consumption with social media (SMD −0.35 (95% CI −0.68 to −0.02)).
Conclusions Social media may provide certain advantages for public health interventions; however, studies of social media interventions to date relating to healthy lifestyles tend to show low levels of participation and do not show significant differences between groups in key outcomes.
- Lifestyle
- Diet
- Exercise
- Social Media
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
This article was conducted following rigorous systematic review methodology; 11 databases were searched, not limited by language or publication type, and study selection, data extraction and quality assessment were all completed independently, in duplicate.
-
This review is limited by methodology of included studies; there was poor reporting of methods for sequence generation, allocation concealment and blinding of participants, personnel and outcome assessment.
-
Social media use is constantly evolving, resulting in difficulties in defining the interventions and ensuring the use of up-to-date sources.
Introduction
Overweight and obesity are characterised by abnormal or excessive fat accumulation that may impair health.1 Body mass index (BMI) is the common measure for body fat. In adults, a BMI greater than 24 is indicative of overweight status and a BMI greater than 29 indicates obesity.2 There is no universal agreement on the classification of obesity in children, but the use of growth charts and reference curves have been suggested.2 BMI does not account for factors such as lean muscle composition or waist circumference, but at a population level it is a good indicator of weight status.2
Overweight and obesity are global problems, affecting developed and developing countries. In 2008, the WHO estimated that more than 1.4 billion adults worldwide, aged 20 years and older, were overweight, and, of those, over 700 million were obese.1 These conditions lead to a variety of chronic diseases such as cardiovascular disease and type 2 diabetes, which pose a large burden on health systems.2
While there are pharmacological and surgical options for treatment of excessive weight, they are typically reserved for extreme situations. Lifestyle interventions involving changes in diet and physical activity levels are most commonly advocated for prevention and treatment,2 particularly decreasing calories and augmenting energy expenditure through increased exercise. Other dietary changes such as increasing fruit and vegetable consumption and decreasing sugary beverage intake are also advocated.
While there have been many studies examining the use of computer and Internet-based interventions promoting healthy diet and exercise,3–7 social media offers a new group of tools whose efficacy as an intervention for lifestyle modifications is just beginning to be evaluated. Social media can be defined as a group of online applications that allow for the creation and exchange of user-generated content, and which can be divided into five different types: (1) collaborative projects (eg, Wikipedia), (2) blogs or microblogs (eg, Wordpress and Twitter), (3) content communities (eg, YouTube), (4) social networking sites (eg, Facebook) and (5) virtual gaming or social worlds (eg, Second Life).8 These tools are a part of what was, in 2004, termed Web V.2.0: the utilisation of the World Wide Web as a platform where content is continuously modified by all users in a collaborative fashion.8
Many benefits of social media have been advocated. Social media provides a cost-effective way to increase user interaction, provide peer-to-peer support and widen access to health interventions.9 However, there are concerns about reliability and quality control of disseminated information. As social media gains in popularity as a health intervention,10 it is important to understand the impact it is having on users.
Our objective was to conduct a systematic review of randomised controlled trials (RCTs) examining the use of social media to promote healthy diet and exercise in the general population to identify (1) how social media is being used as an intervention and (2) whether it is effective.
Methods
This systematic review followed established methods for systematic reviews11 and builds on a scoping review conducted by our group on the use of social media among patients and caregivers.10
Search strategy
A research librarian with extensive experience in systematic reviews developed the search strategy, which involved 11 databases: MEDLINE, CENTRAL, ERIC (all via the Ovid platform), PubMed (hosted by the National Library of Medicine), CINAHL, Academic Search Complete, Alt Health Watch, Health Source, Communication and Mass Media Complete (all via the EBSCO platform), Web of Knowledge, and ProQuest Dissertation and Thesis. The databases were searched from 2000 to April 2013; the search was run on 3 May 2013. The starting date of 2000 corresponded to the establishment of Web V.2.0. References of included studies were also scanned for relevant literature. The search was not restricted by language or publication status. The search strategy for MEDLINE is appended; the searches for other databases are available from authors on request.
Eligibility criteria
RCTs of social media interventions promoting healthy diet and exercise behaviours in the general population were eligible for this review. Interventions using social media, alone or as part of a complex intervention, were included based on Kaplan and Haenlein's8 classifications. We included electronic discussion boards as they involve the sharing of user-generated content. Any outcomes related to lifestyle behaviour change were considered for inclusion in this review. We excluded studies where interventions were targeted to populations with specific medical conditions such as diabetes, metabolic disorder, cardiovascular disease or eating disorders.
Study selection
Two reviewers independently screened all titles and abstracts. The full texts of ‘relevant’ or ‘unclear’ articles were subsequently evaluated for eligibility by two independent reviewers. Discrepancies were resolved through consensus.
Data extraction
Data extraction was completed by one reviewer using a standardised form in Microsoft Excel 2007 (Microsoft, Redmond, Washington, USA) and verified by a second reviewer. The data extraction form was piloted by all reviewers on a set of studies prior to use. Extracted data included study characteristics, population characteristics (target population, age and gender distribution, and setting), intervention characteristics (simple vs complex, description of intervention), outcome measures (primary and secondary), results and authors’ conclusions.
Quality assessment
Study quality was assessed using the Cochrane Risk of Bias Tool11 which examines sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting and other sources of bias. Risk of bias assessment was performed independently in duplicate, and differences between reviewers were resolved through consensus. Risk of bias assessments are described by study and for the review overall; results are discussed in light of some of the common limitations identified in the included set of studies.
Data synthesis
Evidence tables were developed that describe the studies according to the target populations, objectives of interventions, the nature of interventions, outcomes examined and general results and conclusions. We extracted data on the primary and secondary outcomes examined in each study. When there were greater than two study arms in the intervention, we extracted data from the arm with the least intervention (eg, standard care, wait-list control, active intervention without social media component) as the control group. When there were multiple comparison groups involving social media, we extracted data for the group with the fewest co-interventions in an attempt to examine the specific impact of social media.
In order to present results in a consistent manner for all studies, we calculated effect sizes (or standardised mean difference (SMD)) with 95% CIs for the primary outcomes of each study. We did not pool the results as the primary outcome varied across studies; however, we displayed the information graphically to examine the magnitude of effect of the social media interventions.
Studies comparing the same social media tool as one component in the intervention and control groups were not included in the meta-analysis, but were used for descriptive purposes. Where the same outcome was assessed in at least three studies, we combined data in a meta-analysis. For continuous outcomes, we used SMD to standardise results to a common scale.11 For continuous variables, final scores were used; we divided by the standard deviation (SD) of the final value (or baseline SD when the final SD was not given). All results and analyses are presented with 95% CIs. A random effects model was used to combine results as it incorporates statistical heterogeneity that cannot readily be explained.11 We quantified heterogeneity using the I2 statistic.11 We conducted subgroup analyses to examine potential sources of heterogeneity. A priori subgroups included characteristics of the populations (ie, children vs adults) and nature of the comparator (ie, another active intervention vs no-intervention control group). We made a post hoc decision to examine duration of follow-up as a potential explanation for heterogeneity in study findings. We planned to assess for publication bias visually and graphically in the meta-analysis with the most contributing studies using Egger test.12 The Egger test is a linear regression test, evaluating the null hypothesis that the funnel plot is asymmetric. When the p value is high, there is no evidence of asymmetry.
Statistical calculations were performed using Reference Manager V.5.2 (The Nordic Cochrane Centre, Copenhagen, Denmark).
Results
Figure 1 shows the flow of studies through the selection process. Twenty-two randomised RCTs were included in this review. Descriptions of included studies can be found in table 1. Fifteen studies were based in the USA,15–18 21–23 ,25 ,26 ,28 ,29 ,31–34 four in Australia13 ,14 ,19 ,27 and three in other countries.20 ,24 ,30 Sixteen studies intervened in an adult population13–15 19–21 ,23 ,24 ,26–28 30–34 and six in children and youth populations up to the age of 25. 16–18 ,22 ,25 ,29 Overweight or obesity were inclusion criteria in 13 studies.13 ,14 ,17 ,20 ,21 ,23 ,26–28 31–34 Six studies targeted women exclusively16 ,18 ,28 ,29 ,33 ,34 while only one solely targeted men.27
Characteristics of included studies

Flow diagram of study selection.
How social media is being used
The objectives of these studies were to modify behaviour. While interventions varied greatly, this was generally attempted through implementation of a complex intervention utilising discussion boards as the social media element. The distribution of social media tools used in the studies can be seen in figure 2. Interventions typically included online learning modules and self-report diaries of weight, physical activity or dietary behaviours along with a social support component using social media. A description of all interventions and comparisons can be found in table 1. Only three studies did not use discussion boards as the exclusive social media component of the intervention: one study used Facebook,16 one used Facebook and Twitter25 and one used a social networking platform within the study website in addition to discussion boards.14 The duration of the study interventions ranged from 3 months to 2 years.
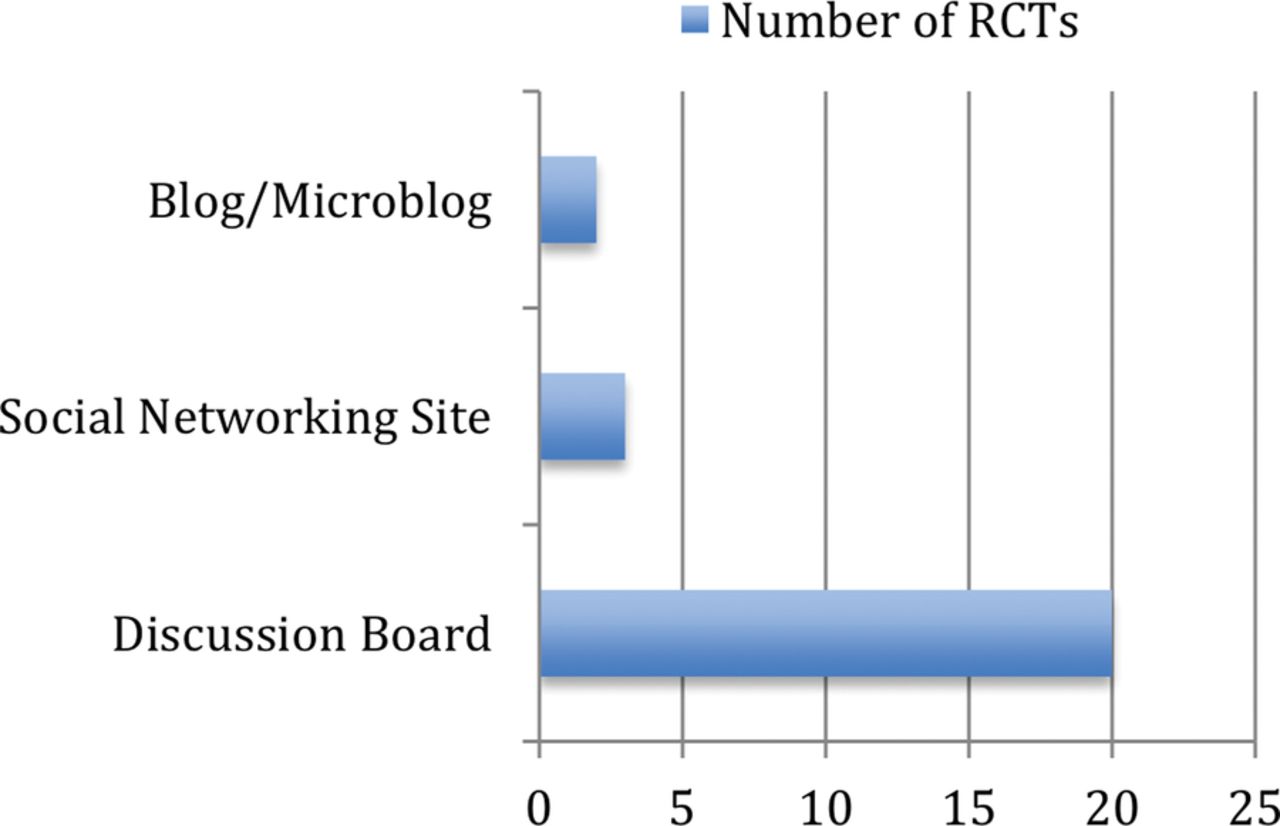
Usage of different social media types in randomised controlled trials of interventions for eating and physical activity behaviours.
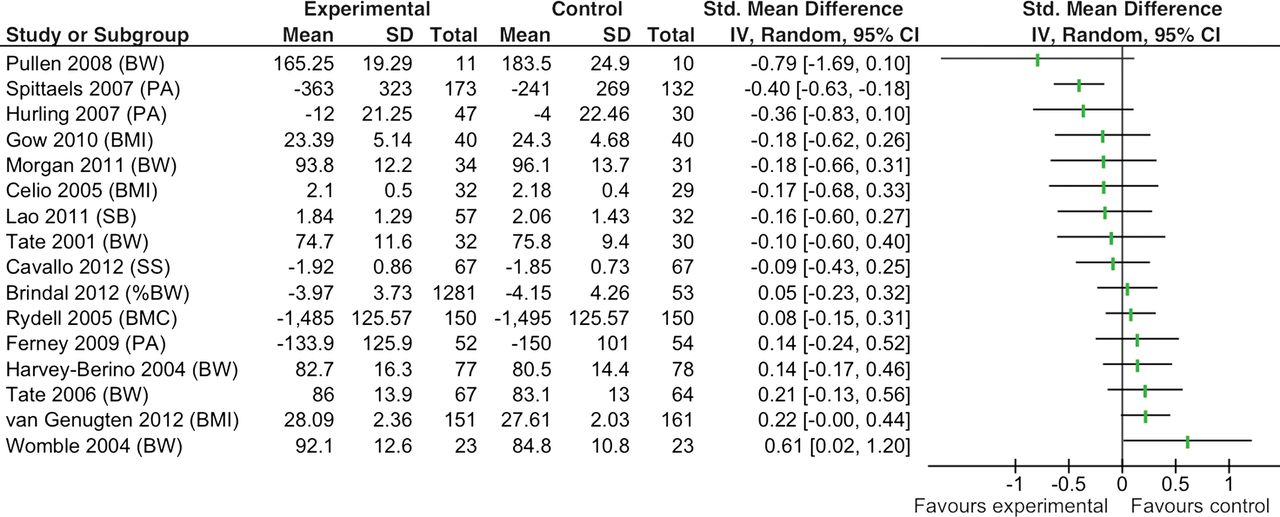
There were a variety of comparison groups (table 1). Four studies had a no-intervention comparator such as a wait-list control22 ,25 ,29 ,30 and 12 studies had an alternate intervention not using social media.14 ,16 ,17 ,19 ,20 ,23 ,24 ,27 ,28 ,31 ,32 ,34 Examples of alternate interventions included access to a non-interactive, information-based website, in-person instruction from a therapist or research assistant or a paper-based manual. Six studies employed social media in the control intervention groups, augmented with additional support or therapy in the intervention group.13 ,15 ,18 ,21 ,26 ,32 ,33 These studies were not included in the statistical comparisons but were used to answer the first research question of how social media is being used. There were 16 studies included in meta-analyses (figures 3⇓⇓–6). Common outcome measures included weight measures or BMI, physical activity levels and dietary measures such as total energy consumed or dietary fat levels.

Effect sizes of primary outcomes. BMC, bone mineral content; BMI, body mass index; BW, body weight; PA, physical activity; SB, sweetened beverage intake; SS, social support.

Forest plot of social media for physical activity.

Forest plot of social media for change in weight.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of social media for change in dietary fat.
Recruitment for these studies was carried out on a voluntary basis and the populations enrolled were fairly homogenous. Of the 15 studies targeting both genders, greater than 70% of participants were women in 10 studies.13–15 ,19 ,21–23 ,26 ,31 ,32 Measures of socioeconomic status were not consistent between studies, but participants were generally well educated. The majority of participants in 12 studies had some form of postsecondary education.15–18 ,21 ,23 ,26 ,29–33 Greater than 70% of participants were Caucasian in 11 studies.13 ,15 ,16 ,18 ,21 ,24 ,26 ,28 ,29 ,31 ,33
Usage of the online interventions was typically low. All studies saw a decrease in programme usage throughout the intervention period and 12 studies had attrition rates of greater than 20%.13 ,14 ,20 ,21 ,23 ,25–28 ,30 ,31 ,34 Many studies used intention-to-treat analysis, but of the 12 studies with attrition rates greater than 20%, only five14 ,20 ,27 ,30 ,34 used this analysis method. The majority of studies acknowledged the feasibility of social media interventions and 13 studies13–15 ,19 ,20 ,23 ,24 ,27–32 recommended further research to elucidate ways to determine optimal intensity of intervention and to increase participation.
Quality assessment
The Cochrane Risk of Bias Tool11 was applied to all 22 studies; none were excluded based on quality assessment. All studies were rated as unclear or high risk of bias (table 2). Sequence generation and allocation concealment were poorly reported. Most studies had high risk of bias due to incomplete outcome data and attrition being unaccounted for. Other biases included baseline imbalances and analysis of individual participants despite group randomisation.
Risk of bias of included studies
Effectiveness of social media
Overall, no significant differences were found for primary outcomes (figure 3). The median effect size was 0.095 in favour of the intervention and ranged from 0.79 in favour of the intervention to 0.61 in favour of the comparator group. Subgroup analysis by population (children/youth vs adults) and comparison group (active vs no intervention) did not show any significant differences. Two of the individual studies showed a significant difference in their primary outcome; in one study, the primary outcome was physical activity, while in the other study, the primary outcome was body weight. In the first case, there was a significant difference in favour of the social media intervention; however, in the other case, a greater difference was observed in the comparison groups. Detailed results of the author's conclusions can be found in table 3. Authors’ conclusions were either positive in 10 studies13 ,17–19 ,21 ,22 ,24 ,28 ,30 ,31 or neutral in 12 studies14–16 ,20 ,23 ,25–27 ,29 ,32–34; in 12 studies, authors recommended future research.13–15 ,19 ,20 ,23 ,24 ,28–32
Results for primary outcomes and conclusions of included studies
Outcomes commonly assessed across studies included physical activity levels, weight and dietary fat intake. Changes in physical activity (SMD 0.13 (95% CI −0.04 to 0.30), 12 studies; figure 4) and weight (SMD 0.00 (95% CI −0.19 to 0.19), 10 studies; figure 5) were not significantly different between participants in the social media and control groups. Pooled results from five studies showed that dietary fat consumption decreased significantly among participants exposed to social media (SMD −0.35 (95% CI −0.68 to −0.02); figure 6). The pooled effect size was small to moderate; however, there was substantial heterogeneity across studies (I2=66%). Differences in comparison groups may have contributed to this heterogeneity. There was no indication of publication bias (p=0.44).
Discussion
This comprehensive systematic review of the literature shows that social media is being commonly used as an intervention to affect a variety of outcomes related to healthy diet and exercise. Most of the current research have been conducted in the USA with overweight or obese adult populations. Discussion boards are the most commonly used form of social media. This technology is most often used as a part of complex interventions that employ other techniques such as learning modules, online self-report journals and even in-person support.
Our results did not show a significant difference between social media interventions and alternate or no intervention controls in promoting healthy diets and behaviours. Meta-analyses of physical activity levels and change in weight showed no benefits from the intervention compared with the control. Pooled results of five studies showed a significant reduction in dietary fat consumption in the social media group. The effect size was moderate; however, there was significant heterogeneity between studies suggesting that the effect may vary due to other factors. Subgroup analyses showed no significant differences in the effects of the intervention according to age, or the nature of the comparator.
A lack of effect in terms of changes in weight and physical activity levels may be due to the inherent difficulty in affecting behaviour change as observed across many different types of interventions. Although initial positive changes may be seen, behaviour change in the long term is often not sustained. Our findings are consistent with evaluations examining other interventions targeting healthy behaviours to manage weight. For example, a systematic review of interventions to manage weight based on the transtheoretical model stages of change model concluded that these interventions resulted in minimal weight loss (Tuah). A systematic review of major commercial weight loss programmes in the USA showed minimal evidence to support these interventions; moreover, they found that the interventions “were associated with high costs, high attrition rates and a high probability of regaining 50% or more of lost weight in 1–2 years” (Tsai). In an overview by Kohl et al, online behaviour change strategies that were more promising included the use of tailored feedback, theory, interactivity, goal setting and a combination of online and in-person support.37 The use of these strategies in conjunction with mobile connective technology has been successful, and may also enhance the success rate when using social media interventions.38
Attrition was generally high in these studies which may introduce bias into results. However, participant loss is a common problem, and Eysenbach proposes more extensive reporting of adherence rates in Internet health interventions.39 End-user engagement during the development of the intervention is a method that could be attempted in future research to decrease attrition;40 offering financial incentives may also decrease attrition.41 Study duration and follow-up should also be increased to examine long-term effects of healthy diet and exercise interventions as regaining weight or falling into old behaviours can be a setback in the long term.
Limitations
While we used a methodologically rigorous design for our review, the validity of our results may be limited by the quality of the primary studies we included. There was poor reporting of methods for sequence generation, allocation concealment and blinding of participants and personnel and outcome assessment in the included studies. Future RCTs should take this into consideration and follow standards for designing and reporting the study (eg, CONSORT).42 In many cases, non-significant between-group findings were seen due to improvement in the intervention and control groups. This may have been a consequence of poor blinding of participants or a Hawthorne effect, whereby the participants showed a change in behaviour as a result of being studied. Measures were also typically self-reported which may have led to social desirability bias.
Recruitment for primary studies was on a voluntary basis. This may have resulted in increased participant motivation and selection bias. Losses to follow-up were very high in included studies, which can impact the validity of meta-analyses and more generally the utility of the intervention. Further, many authors commented on the challenges of adherence and keeping the participants engaged. Those considering social media as part of an intervention should not assume that the target audience will be engaged simply on the premise that social media is popular and widespread. Involving end-users from the target audience in selecting the intervention components and providing feedback during the intervention development may help optimise uptake and adherence.40 The high attrition rates also have implications on the ability to generalise results. Populations involved in these studies were also typically fairly homogenous, comprising mainly female, Caucasian participants of a higher socioeconomic status, further affecting the ability to generalise results.
The complexity of the interventions studied and the fact that social media may only play a small part, or no part, if programme adherence is low, in the intervention makes it difficult to assess the relative impact of social media.
Conclusions
Social media may provide certain advantages for public health interventions because it is popular, it can reach a large and diverse audience and may be relatively less expensive to administer and maintain. However, studies of social media interventions to date relating to healthy diet and exercise tend to show low levels of participation and adherence, and do not show significant differences between groups in key outcomes. Despite its growing popularity, there is little evidence that social media interventions demonstrate a significant benefit for improving healthy diet and exercise. As social media is an ever changing technology, future research is needed to continue to evaluate its effectiveness as a healthcare tool, particularly in combination with other modalities that show some utility such as tailored feedback and in-person support. Involving the end-users from the target audience in the selection and development of the social media intervention may optimise uptake and adherence.
Acknowledgments
The authors thank Andrea Milne for conducting the literature searches. They also thank Baljot Chahal, Annabritt Chisholm and Michelle Foisy for assistance with study selection.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors GW, MPH and LH designed the study and interpreted the data. GW coordinated the project. GW, MPH and JS screened articles and performed data extraction. BV contributed to the study design and statistical analyses. GW drafted and all authors critically reviewed the manuscript. All authors read and approved the manuscript. LH is the guarantor.
-
Funding This study was funded in part through a knowledge synthesis Grant from the Canadian Institutes of Health Research, grand number 262961 and a Knowledge-to-Action Grant from Alberta Innovates-Health Solutions, grant number AIHS KTAG 201201175.
-
Competing interests GW was funded through the University of Alberta Research Experience (U ARE) internship programme. LH holds a New Investigator Salary Award from the Canadian Institutes of Health Research.
-
Ethics approval As this review used only published materials as sources of information, no ethics approval was needed.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.