Article Text

Abstract
Objectives Studies from western countries show that dentists are vulnerable to work-related musculoskeletal disorders (WMSDs) of the neck and upper extremities, but little is known about their epidemiology among members of this rapidly growing profession in China. This study aims to investigate the prevalence of WMSDs and identify potential risk factors associated with their occurrence in the dental profession in China.
Setting and participants A cross-sectional survey was carried out in 52 different hospitals in a large metropolitan city in China. A total of 304 questionnaires were distributed to respondents identified via stratified random sampling and 272 dentists (121 females and 151 males) completed the survey. The response rate was 89.5%.
Outcomes Visual analogue score was used to record neck and upper limb musculoskeletal symptoms on a body chart. Work-related risk factors, including physical and psychosocial factors, were accounted for in the regression analysis.
Results 88% of the dentists reported at least one musculoskeletal disorder and 83.8% suffered from neck pain. In the multivariate analyses, working hours per day were associated with neck pain (OR=1.43; 95% CI 1.03 to 1.98). Inability to select the appropriate size of dental instrument was associated with shoulder (OR=2.07; 95% CI 1.00 to 4.32) and wrist/hand (OR=2.47; 95% CI 1.15 to 5.32) pain. As for psychosocial factors, high job demand was associated with symptoms in the shoulder (OR=1.09; 95% CI 1.00 to 1.18), elbow (OR=1.11; 95% CI 1.03 to 1.19) and wrist/hand (OR=1.09; 95% CI 1.02 to 1.17). Regular physical exercise was associated with decreased neck pain (OR=0.37; 95% CI 0.14 to 1.00).
Conclusions The prevalence of WMSDs among Chinese dentists is high. Specifically, long working hours, inability to select the appropriate size of dental instrument and high job demand are the most significant risk factors.
- OCCUPATIONAL & INDUSTRIAL MEDICINE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
This study was carried out with dentists working in 52 different hospitals in a large Chinese metropolitan city, selected by stratified random sampling. The response rate of 89.5% of this multicentre survey allows a relatively precise population estimate. The study reveals a high prevalence of work-related musculoskeletal disorders (WMSDs) in the dental profession in China.
-
The results provide up-to-date evidence on the associations between physical factors and WMSDs. Long working hours were associated with neck pain and inability to select the appropriate size of the dental instrument was associated with shoulder and wrist/hand pain.
-
The study also shows that high job demand was associated with neck and upper limb WMSDs. A healthy lifestyle, including regular exercise, was found to be associated with reduced occurrence of neck pain.
-
The content validity of the survey instrument used in this study was tested thoroughly and steps were taken to maximise response, and minimise error and information bias.
-
The study is not a nationwide general population survey across China, which limits its generalisability. Given the cross-sectional design, the longitudinal effect of physical and psychosocial risk factors on dentists’ WMSDs could not be obtained.
Introduction
Dentistry is a rapidly growing occupation in China, with numbers increasing from 36 378 dentists in 2000 to more than 120 000 in 2013.1 However, little attention has been paid to occupational health hazards in the dental profession in China. While work-related musculoskeletal disorders (WMSDs) have been frequently reported in the dental profession across different countries,2–6 knowledge of the phenomenon among Chinese dentists is lacking. A study conducted in New Zealand reported a 1-year WSMD prevalence among 57% in the neck, 54% in the lower back and 52% in the shoulder among the dentist population.5 Similar results were found by Thornton et al6 who discovered that 48% of dentists in the US suffered from neck pain, 44% in the back, 31% in the shoulder and 20% in the hands. These studies show consistently high frequencies worldwide of neck and shoulder disorders among dentists, which may interfere with daily activities and normal life. In a Dutch study, among those dentists having disability insurance, 7% required extended sick leave and 30% of these had not returned to work more than a year later. It was estimated that nearly half of these Dutch dentists might have to retire prematurely due to poor health and work-related illness.7
Dentists are prone to suffer from cumulative disorders due to constant exposure to occupational health hazards. While working, dentists usually assume uncomfortable static postures and maintain their head in a rotated position, with the neck flexed and shoulders/upper arm abducted, or sustain other awkward positions for a long period.3 ,8–10 Holding a static awkward posture for long periods can lead to chronic muscular fatigue, discomfort or pain. Even worse, continual static loading on muscles and joints may result in adaptive alterations in the normal structures of soft tissues, such as shortening or other pathological effects.11 ,12 Dentists are also exposed to psychological stress when dealing with patients due to the need to work with high concentration and precision, which is associated with an elevated risk of developing WMSDs.13 As is already known, stress can increase muscle tension and cause pain, especially in the trapezius muscle.8 ,11 ,13 Dentists also face the psychosocial risk factors of high job demands, lowjob control and limited social support.14 Personal characteristics such as gender, height and insufficient rest periods can increase the risk of developing WMSDs.15 Physical inactivity during leisure, and work and family overload can also increase these odds.16
In Western countries, attention to and awareness of WMSDs in the dental profession has increased substantially due to the elevated number of musculoskeletal symptoms significantly affecting the health of dentists.6 ,17 ,18 However, in China, even though the population amounts to 1.3 billion people, there is still a lack of research about the prevalence of WMSDs in this rapidly growing occupational sector or the possible work-related risk factors for Chinese dentists. Therefore, investigating the prevalence of work-related neck and upper extremity symptoms among dentists in China is of crucial importance. Identifying the factors associated with the occurrence of these musculoskeletal symptoms can help to develop ergonomic recommendations for the dental profession in China. This study, therefore, aims to investigate the prevalence of WMSDs and identify potential risk factors for occurrence in the dental profession in China.
Methods
Design
A cross-sectional survey of a stratified random sample of dentists was conducted in a set of hospitals in Guangzhou, China. The criteria for hospital selection were based on location and hospital grade, with 52 of a total of 117 pooled hospitals being included. There are altogether 117 hospitals that have a department of dentistry in the urban area of Guangzhou city which has been divided into six specific administrative districts. Hospitals in China are classified as First Class Tertiary Hospital, Second Class Hospital and Third Class Community Health Centre. According to the distribution of different classes of hospitals in each specific district, the 52 hospitals included in the present study were randomly selected proportionally from the six administrative districts in Guangzhou.
An investigative team consisting of 17 physiotherapy students was formed to distribute the questionnaires to dentists. The role of the investigators was to supervise the respondents to complete the questionnaire after a brief introduction to the study, to secure informed consent and to explain any item in the questionnaire to respondents, if necessary.
Questionnaire
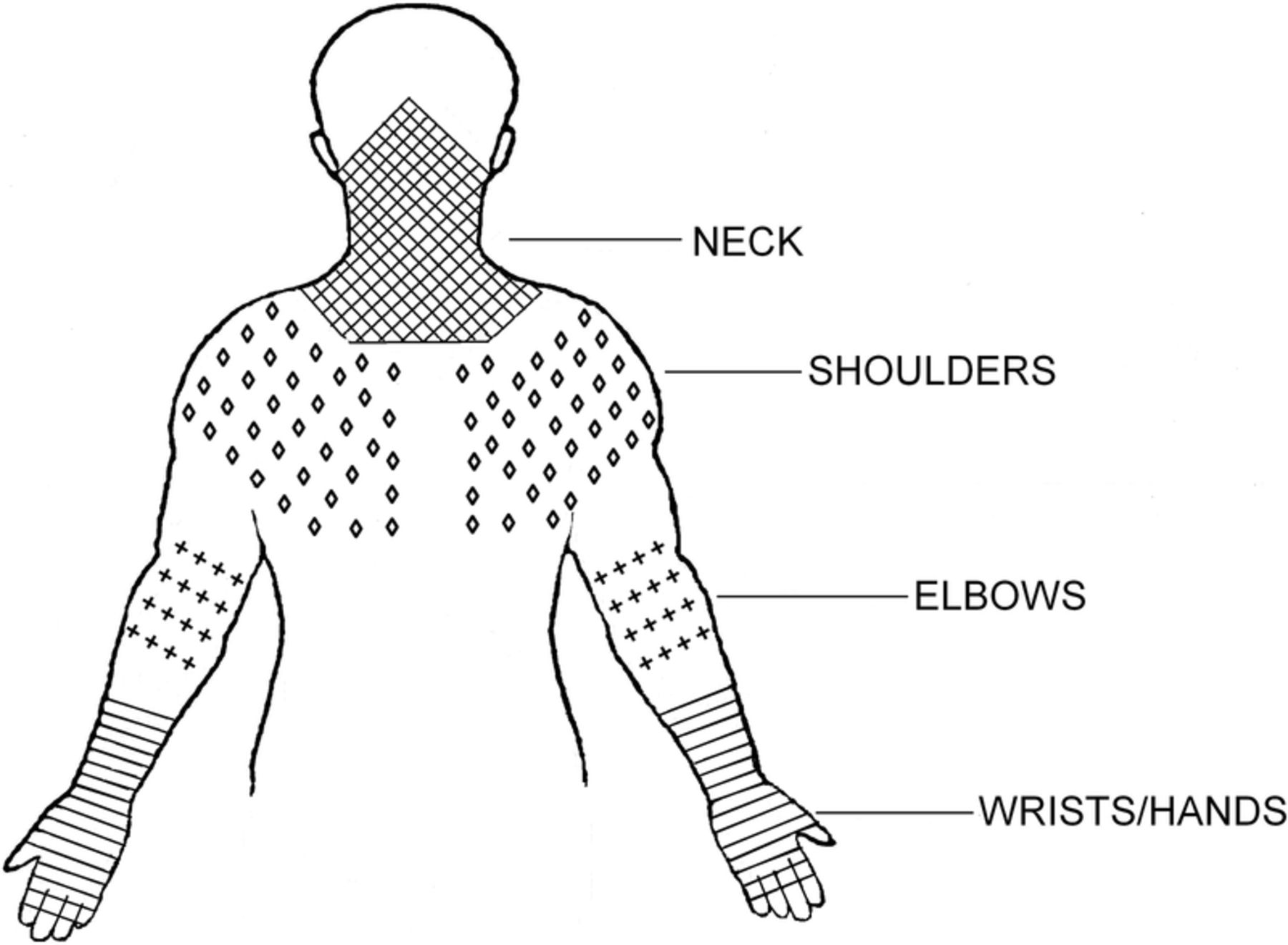
A total of 304 questionnaires were distributed and 272 dentists (121 females (44.5%) and 151 males (55.5%)) returned completed surveys, giving a response rate of 89.5%. The 62-item questionnaire was specially developed for this study and its content validation was carried out based on previous literature.19–22 The first section included demographic questions about gender, age, educational level and job title. Section two concerned personal lifestyle factors, such as smoking, sleep quality, exercise frequency and medical history. For example, frequency of physical exercise was determined by the question “How many times do you exercise every week?” Sections three and four dealt with working conditions —including duration of employment, working hours, patient workload, working posture, use of dental instruments, etc. For example, appropriate use of dental instruments was determined by the questions “Do you deliberately choose the size of dental instruments?” (response options yes/no), and “Please write down the diameter of the tools you handle the most.” The fifth section focused on the presence of WMSDs, including the body region(s), intensity and the consequences of the symptoms. Using a drawing modified from the Standardized Nordic Questionnaire,23 respondents were asked to identify body regions where they suffered from musculoskeletal symptoms and a numerical scale ranging from 0 to 10 was used to evaluate the intensity of symptoms in each region over the past 12 months. The body chart used is illustrated in figure 1 below. Section six examined job-related psychosocial factors to explore the level of job demand, job control and stress at work. High job demand was related to items such as working fast and hard, excessive amounts of work and insufficient time to complete all duties. These questions were scored using a 5-point Likert scale ranging from ‘almost never’ to ‘always’, yielding a summed score for job demands. The final section concerned prophylactic activities or treatment received for WMSDs.
{kind=link}
The body chart indicating different musculoskeletal regions modified based on the Standardised Nordic Questionnaire.23
Statistical analysis
Descriptive statistics were used to explore the individual characteristics of all dentists surveyed and a χ2 test used to compare differences between genders. A logistic regression was then performed to evaluate the influence of individual characteristics, physical work conditions and psychosocial factors on the occurrence of neck and upper limb musculoskeletal disorders. ORs with 95% CIs were calculated as measures of association. A univariate logistic regression analysis was carried out for the initial selection of potential risk factors for WMSDs at the significance level p<0.10. All independent variables that showed a significant association with the musculoskeletal symptoms in the univariate regression were included in the multivariate logistic regression model. These analyses were conducted separately for each region (neck, shoulder, elbow and wrist/hand). All data analyses were conducted using SPSS V.17.0 (SPSS Inc, Chicago, Illinois, USA) and all hypotheses were established at the significance level p=0.05.
Results
Baseline characteristics
Table 1 shows the demographic characteristics of the participants. As noted earlier, 272 dentists with a mean age of 34.7±8.9 years (range: 20–60) participated in the survey. In terms of job titles, the majority (about 73%) were at the level of dentist-in-charge or below. Over 60% held a bachelors’ degree or above, with about 10% holding a masters’ degree and 6% a doctorate degree.
Demographic characteristics of the surveyed dentists
The dentists surveyed had worked in dentistry for an average of 11.6 years. The mean number of hours worked per week was 40.5 h. Seventy-nine percent dealt with 5–15 patients per day. Over 90% spent 10–60 minutes on one patient. Approximately 73.8% of the respondents had adjusted their operating posture while working, but 26% did not change posture nor carry out any other adjustment. Over 60% of the dentists took regular physical exercise, with an average frequency of 2.2 times per week; 2.2% rarely exercised or did so only occasionally while 35% reported that they did not do any kind of regular exercise. About 19% of respondents smoked, with more males than females doing so (p<0.001).
Prevalence of musculoskeletal symptoms
The results of the Nordic Questionnaire-based items showed a higher prevalence of symptoms of pain in the neck and shoulder regions compared with the distal regions of elbow and wrist/hand. Neck pain was the most prevalent musculoskeletal symptom in the past 12 months, as reported by 83.8% of the surveyed dentists, with a mean pain intensity of 4.45 on a scale of 0–10. Among this group, 88% of respondents with neck pain thought the symptom was related to work and was aggravated after work. The 12-month prevalence of shoulder symptoms on either side was about 73.5% (12.9% for the left shoulder, 30.5% for the right side, and 40.1% for both sides); 44% had experienced wrist/hand disorders and elbow symptoms were reported by 30%. In terms of symptom severity, significantly higher pain intensities were reported on the right side compared to the left for the shoulder, elbow and wrist/hand regions. The majority of respondents reported symptoms on the dominant side (62%) and 23% reported symptoms on both sides. Descriptive statistics showed a significantly higher prevalence of shoulder pain among female dentists compared with males (see table 1).
Comorbidity in neck and upper extremities was common, with a total of 88% of respondents reporting at least one musculoskeletal disorder and 75% at least two. Dentists with neck pain more often reported shoulder pain (87%) and wrist/hand symptoms (51%). More than 20% of the surveyed dentists reported a reduction in work activities due to their musculoskeletal disorders and 25% had reduced their leisure activities because of the symptoms. About 39% of the respondents had sought out medical care at least once due to musculoskeletal symptoms and 57% of those with neck pain had sought help for symptom relief. Table 2 shows the musculoskeletal symptoms for the different regions with prevalence and mean symptom scores.
Prevalence of neck and upper extremity musculoskeletal symptoms in the previous 12 months
Association between risk factors and musculoskeletal symptoms
In univariate analyses, patient-related workload (time spent per patient) was significantly associated with the occurrence of neck pain, shoulder and wrist/hand disorders. Selection of a dental instrument of an incorrect size was significantly related to shoulder, wrist/hand symptoms and comorbidity. However, no significant association was found between the diameter of tools and musculoskeletal symptoms. Gender was associated with the occurrence of shoulder pain. Age as well as years of employment was associated with shoulder and wrist symptoms. In terms of psychosocial factors, job demand was associated with the development of WMSDs in neck, shoulder, elbow and wrist/hand regions. Healthy lifestyle, in the form of regular exercise, appeared to be related to a reduced occurrence of neck, elbow and wrist/hand pain as well as comorbid symptoms. Smoking was related to the occurrence of wrist/hand and comorbid pain (OR=0.41 and 0.48, respectively). Table 3 presents the univariate analyses for neck and upper limb musculoskeletal symptoms over the past 12 months.
Univariate analyses for neck and upper extremity symptoms in the past 12 months
The multivariate analyses showed that the number of working hours per day was significantly associated with the occurrence of neck pain (OR=1.43; 95% CI 1.03 to 1.98). The inability to select the appropriate size of dental instrument was significantly related to symptoms of shoulder (OR=2.07; 95% CI 1.00 to 4.32), wrist/hand pain (OR=2.47; 95% CI 1.15 to 5.32) and comorbidity (OR=2.56; 95% CI 1.25 to 5.27).
In terms of psychosocial factors, the multivariate logistic regression analysis showed that job demand was associated with WMSDs in the shoulder, elbow and wrist/hand (OR>1; 95% CI 1.00 to 1.18; 1.03 to 1.19; 1.02 to 1.17, respectively). Job demand was also associated with comorbidity of WMSDs (OR=1.11; 95% CI 1.03 to 1.20) in dentistry work. In terms of lifestyle factors, regular exercise was associated with reduced odds of suffering work-related neck symptoms. The results of the multivariate analyses on risk factors for the presence of neck and upper limb symptoms are shown in table 4.
Multivariate analyses for neck and upper extremity symptoms in the past 12 months
Discussion
This study shows there is a high prevalence of neck and upper extremities pain over the past 12 months among Chinese dentists. These findings were associated with longer working hours, the inability to deliberately select the size of the dental instrument and higher job demand.
The prevalence of neck pain among 83.8% respondents is much higher than the 48% of dentists reported in the USA by Thornton et al,6 and the 50% in New Zealand by Samotoi et al.5 The prevalence of shoulder pain among 76% was also higher than the 53.3% among dentists in Queensland, Australia.4 More female dentists suffered from shoulder symptoms than males. However, gender was not statistically significant in the multivariate analysis of shoulder pain. Comorbidity in WMSDs is also a common finding.24 In this study, 75% of respondents had at least two musculoskeletal symptoms, compared with 35% in Alexopoulos et al's24 study. Respondents with neck pain were more likely to report other upper limb symptoms. In particular, there was a relatively strong association between neck, shoulder and hand/wrist pain. Eighty-seven percent of the dentists with neck pain also suffered shoulder pain and 51% had experienced wrist/hand symptoms. Our study also found that the prevalence of musculoskeletal disorders was higher on the right side than the left for the shoulder (30.5% vs 12.9%), elbow (13.6% vs 3.3%), and wrist/hand (23.9% vs 4.8%). A higher prevalence of right-sided versus left-sided pain has also been observed in other occupational groups such as office workers.25 The mean score for symptoms on the right hand/wrist region was significantly higher than for the left side (3.77±2.35 vs 1.63±1.74, p<0.05). This could be explained by the predominance of right-handed respondents and therefore, the symptoms occurred on the dominant side. Presumably, the underlying reason is related to exposure to right-handed manipulation position in their daily work.
The high occurrence of WMSDs among the dentist population has consequences for their work and normal daily lives.7 ,26 The present survey found that over 20% of the respondents had reduced their workload due to WMSDs and 25% spent less time on everyday leisure activities because of their symptoms. Further, more than half of the dentists reporting neck symptoms had sought out medical treatment and/or symptom relief. Computer workers, who have a similar sedentary working posture, have been found to have a comparable prevalence of 65.7% for musculoskeletal symptoms in the neck.27 Another study showed that the prevalence of neck and upper extremity WMSDs in clerical workers was around 60%.28 Possible risk factors contributing to the high prevalence of neck and upper extremity disorders have been reported in previous studies.3 ,8–10 ,24 Similar to research in other countries, significant associations between work-related physical factors and the occurrence of musculoskeletal symptoms were identified in the present study. Daily working hours were significantly associated with the presence of neck pain (OR=1.43; 95% CI 1.03 to 1.98). These respondents worked for more than 40 h/week on average, with a mean of 5.4 days/week and 7.5 h/day. Long working hours is considered to be correlated with job demand,24 which means that dentists have to maintain static and/or awkward postures for prolonged periods contributing to musculoskeletal overload and pain. It has also been suggested that a tight work schedule has been shown to lead to an elevated risk of developing neck and upper limb WMSDs, and working for more than 2 hours without a break has been strongly associated with neck symptoms among computer users.27 ,28 Prolonged use of small dental instruments is likely to be a special occupational hazard for WMSDs in dentists.29 ,30 In the current study, 44% reported work-related wrist/hand symptoms, which is approximately twice that reported by previous studies, that is 26%24 and 22%.2 In our multivariate analysis, the inability to select the size of the dental instrument to be used was significantly associated with the development of wrist/hand symptoms (OR=2.47; 95% CI 1.15 to 5.32). In clinical practice, dental scaling and endodontic treatment tasks require dentists to pull and/or rotate instrumental tools, which requires precision in hand/finger movement and a high level of pinch force.30 ,31 Moreover, they have to hold their wrist in an awkward position in order to get and maintain access to different areas within the mouth.30 The precise and accurate use of various small dental instruments hence poses an elevated risk for dentists in terms of developing wrist/hand disorders. Handling small instruments requires awkward arm and shoulder positions to reach specific regions within the mouth, which inevitably increases load on the shoulder. Inappropriate working postures across different body regions may explain the relationship between tool sizes and increased risk of comorbidity (OR=2.56; 95% CI 1.25 to 5.27). However, we found no significant association between the diameter of the dental instruments used and the prevalence of WMSDs. It would be useful for future studies to investigate the possible correlation between different tool sizes and musculoskeletal symptoms so as to shed light on the specific size of working tools for dentists that may increase their likelihood of developing WMSDs.
With regard to psychosocial factors, the practice of dentistry was perceived as requiring high levels of mental demand and high control over the job, a perception shared by Swedish dentists.32 Dentists with upper extremity WMSDs considered their psychosocial environment and general health to be significantly poorer than those without such disorders, though the effect of psychosocial work characteristics seemed to make a less significant contribution to the final WMSD-risk factor model.33 According to other studies, high job stress and non-work-related stress are also associated with upper extremity WMSDs.34 ,35 The results of this study are consistent with this, demonstrating an association between job demand and work-related shoulder, elbow and wrist/hand symptoms in the past 12 months. Most of the respondents in this study (87%) reported that they had to endure pain to complete their work. Among this group, approximately 30% were in pain often or always during their working days. High job demand may increase the need for recovery.24 However, the majority (75%) of these dentists reported that they had very little opportunity to rest due to high job demand. Other evidence36 suggests that mental workload can adversely affect physical capacity (in terms of fatigability and recovery). Furthermore, high job demand was associated here with comorbidity in the present results (OR=1.11; 95% CI 1.03 to 1.20), consistent with the results of a previous study.24 The psychosocial element of high job demand may interact with physiological factors to affect musculoskeletal disorders directly and indirectly.37 Previous findings38 support such an interaction between physiological and psychosocial factors in the WMSD aetiology model. Furthermore, individual differences in muscular capacity may affect fatigability and recovery and thus, the risk of developing WMSDs. Physical activities during leisure may decrease the odds of developing WMSDs in the working population.16 ,39 This study has also identified a significant association between regular exercise and lower occurrence of neck pain. Those dentists who exercised (2.2 times per week on average) were less likely to have neck pain compared with those who did not. Regular exercise may provide dentists with a break from their strenuous workload, and refresh and strengthen their bodies while also providing mental relaxation from the high psychosocial demands of the job. These effects probably interact to contribute to a better health status and a decreased risk of musculoskeletal symptoms.39 However, in the present study, more than 30% of dentists reported that they did not do any kind of exercise regularly; 2.2% rarely exercised or did so only occasionally. This indicates that inactive leisure activities remain part of many dentists’ lifestyle. Future studies should investigate whether regular exercise may be a vital factor to help Chinese dentists prevent the development of WMSDs.
Smoking is regarded as a possible risk for the development of neck and upper extremity disorders among different employee populations.40–42 A prevalence rate ratio (PRR) of 1.2 (95% CI 1.1 to 1.3) has been found for neck/shoulder symptoms in smokers versus those who had never smoked.40 In contrast, we found ORs of 0.41 (95% CI 0.22 to 0.79) and 0.48 (95% CI 0.25 to 0.93) for the effect of smoking on wrist/hand and comorbid pain, respectively, in the univariate analysis. However, when work-related physical and psychosocial factors were included in the multiple logistic regression models, these associations were no longer statistically significant, indicating that the univariate analysis had been influenced by confounding.
There are both strengths and limitations to the present study. It was carried out among dentists in 52 different hospitals in a large Chinese metropolitan city with various hospitals, advanced health and medical services and numerous medical professionals. This improves the generalisability of the results for dentists working in major cities in China. The response rate was high (89.5%), which also minimises response bias. The high prevalence of WMSDs found in this study should highlight the need for dental professionals and society in general to improve the working environment of Chinese dentists. Specific occupational health education programmes, including ergonomic workplace adaptation, refined work organisation and psychosocial coping skills, should be implemented to prevent the severe risks to health in this occupation. Other potential risk factors such as workstation adjustability and BMI, which have been shown to be associated with WMSDs among computer workers, were not examined in this study.28 It would be valuable and informative if specific details could have been collected in terms of the different performing procedures of dentists during work using more direct observational and objective measurement tools, such as RULA, which was absent in the present study due to a tough balance to obtain as much information as possible. Future studies are warranted to add to this part of useful investigation. Given the importance of workstation environments for both computer workers and dentists, this would be worthy of further exploration. Given the limitations of this cross-sectional study, further research using a prospective design is recommended to clarify the longitudinal effect of both physical and psychosocial risk factors on the development of WSMDs in dentists.
Conclusions
This study has identified an alarmingly high prevalence of neck and upper extremity WMSDs among dentists in China, much higher than that in the western countries. The symptoms of neck pain increased with the number of working hours per day. The inability to select the appropriate size of dental instruments was associated with higher odds of shoulder, wrist/hand and comorbid pain. High job demands were associated with higher odds of pain in all the body regions investigated. Both physical workload and psychosocial stress factors need to be taken into account when considering preventative measures. A multidisciplinary approach with primary prevention, early intervention and continuous education about the potential effects of dentistry-related risk factors should be employed.
Acknowledgments
The authors thank the research team from the Department of Rehabilitation Sciences of Sun Yat-sen University for carrying out the data collection for this survey.
References
Footnotes
-
Contributors YW was involved in conception and design of the study and revising the manuscript for important theoretical content. BF took part in acquisition of data and drafting the manuscript. QL analysis and interpretation of data acquired; GS participated in interpretation of data acquired and revising the manuscript. LLA was involved in critical revision of the manuscript for significant content.
-
Funding This study was supported by The Youth Teaching Staff Fund of Sun Yat-sen University (Project No.:13YKPY38) and The Sun Yat-sen University Students’ Research Fund.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethics Committee of Sun Yat-sen University.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.