Article Text

Abstract
Objective Since conflicting results have been published on the role of tobacco smoking on the risk of endometriosis, we provide an up-to-date summary quantification of this potential association.
Design We performed a PubMed/MEDLINE search of the relevant publications up to September 2014, considering studies on humans published in English. We searched the reference list of the identified papers to find other relevant publications. Case–control as well as cohort studies have been included reporting risk estimates on the association between tobacco smoking and endometriosis. 38 of the 1758 screened papers met the inclusion criteria. The selected studies included a total of 13 129 women diagnosed with endometriosis.
Setting Academic hospitals.
Main outcome measure Risk of endometriosis in tobacco smokers.
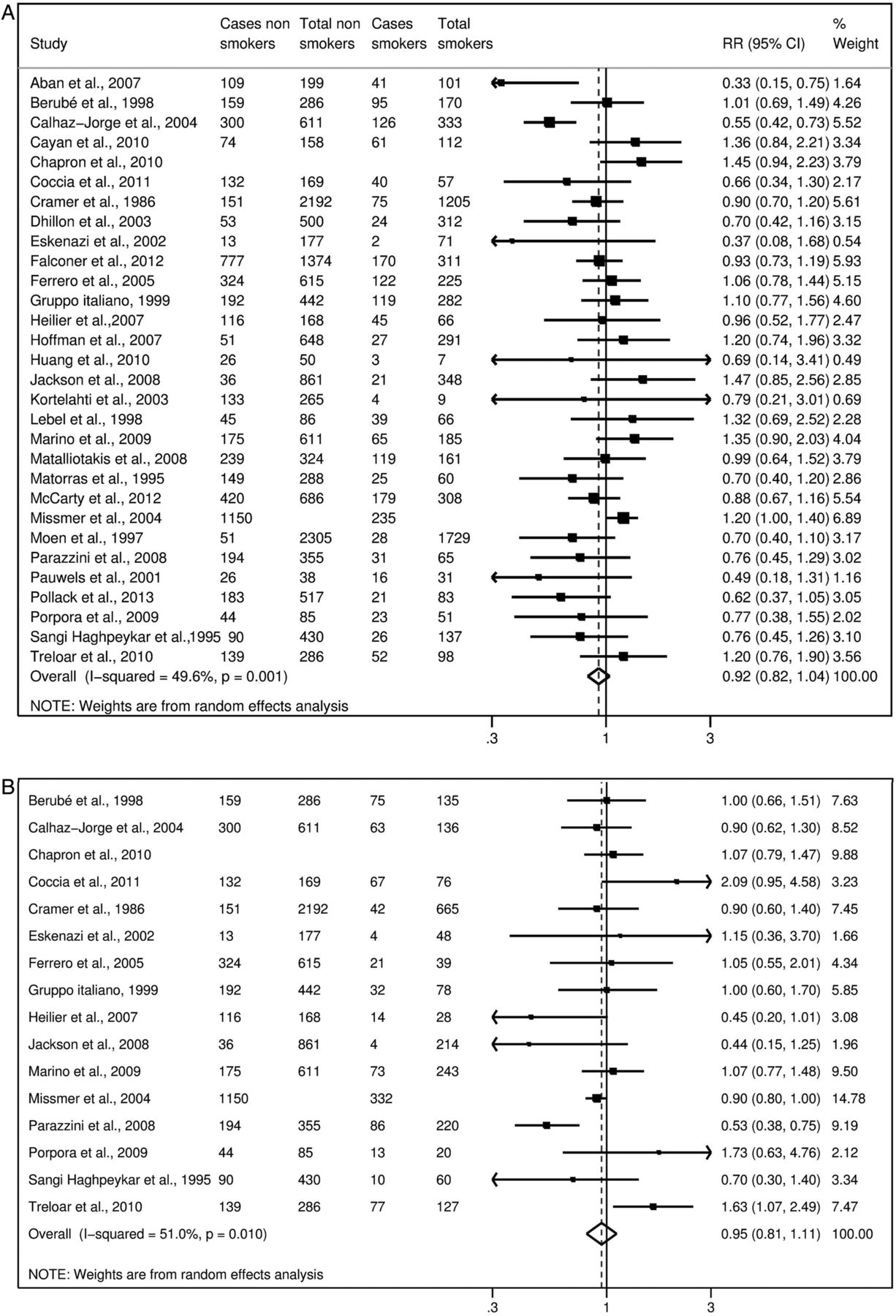
Results We obtained the summary estimates of the relative risk (RR) using the random effect model, and assessed the heterogeneity among studies using the χ2 test and quantified it using the I2 statistic. As compared to never-smokers, the summary RR were 0.96 (95% CI 0.86 to 1.08) for ever smokers, 0.95 (95% CI 0.81 to 1.11) for former smokers, 0.92 (95% CI 0.82 to 1.04) for current smokers, 0.87 (95% CI 0.70 to 1.07) for moderate smokers and 0.93 (95% CI 0.69 to 1.26) for heavy smokers.
Conclusions The present meta-analysis provided no evidence for an association between tobacco smoking and the risk of endometriosis. The results were consistent considering ever, former, current, moderate and heavy smokers, and across type of endometriosis and study design.
- GYNAECOLOGY
- EPIDEMIOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
Meta-analysis including 38 papers without any relevant asymmetry in the funnel plot.
-
The Egger's test was not statistically significant.
-
In some studies, choice of cases as asymptomatic without distinguishing factors related to endometriosis to those associated with pelvic pain or infertility.
-
In some studies, choice of controls in whom disease was not laparoscopically ruled out.
-
Tobacco smoking based on patients’ self-reported information.
Introduction
Endometriosis is an oestrogen-dependent, chronic inflammatory gynaecological condition characterised by the proliferation of functional endometrial tissue that develops outside the uterine cavity, which may cause pain and infertility.1 However, despite its relatively high prevalence, which spans from 20% in asymptomatic women2 to 30% in women with infertility,3 and 45% in women with pain symptoms,4 risk factors for this condition remain largely unknown.
Among the risk factors investigated, some studies have examined the role of tobacco smoking. In a Portuguese study investigating clinical and lifestyle factors in infertile women, current smokers had a decreased risk of endometriosis as compared to non-smokers or former smokers.5 In a case–control study from Turkey evaluating the interaction between tobacco smoking and glutathione-S-transferase gene polymorphism as a risk factor for endometriosis, an inverse association between smoking and endometriosis was observed.6 In a case–control study carried out in the USA, infertile women with endometriosis and fertile controls were compared, and a decreased risk of endometriosis was found, though limited to women who had begun smoking at an early age and were heavy smokers.7 Other studies did not find significant association.3 ,8–14
The biological plausibility potentially linking smoking and endometriosis resides in its endocrine and inflammatory mechanisms. Smoke compounds disrupt steroidogenesis, leading to impairment of E2 synthesis15 ,16 and progesterone synthesis deficiency.17–19 Moreover, smoking has a strong effect on inflammatory mediators in the pulmonary as well as extra-pulmonary environments and can further trigger inflammation associated with the disease, resulting in pro-inflammatory gene overexpression.20
A clear definition of the relation between smoking and endometriosis risk is required in order to better understand the role of oestrogens, in consideration of the potential antioestrogenic effect of smoking. Otherwise, in clinical terms, a direct association as reported in some studies6 ,7 may suggest preventive measures.
Thus, in order to investigate the possible relation between tobacco smoking and endometriosis, and to provide an overall quantitative estimate of any such relation, we combined all published data on the issue in a meta-analysis.
Materials and methods
Search strategy
We performed a PubMed/MEDLINE search of papers published between 1966 and September 2014, using the terms “tobacco” or “smoking” or “cigarette” in combination with “risk factor” or “epidemiology”, and “endometriosis”, following the MOOSE (Meta-analysis of Observational Studies in Epidemiology) guidelines21; details on the search terms are provided in online supplementary appendix. We selected only studies on humans, published as full-length papers in English. No effort was made to identify papers published in other languages or unpublished studies. Moreover, we reviewed the reference lists of the retrieved papers to identify any other relevant publications. Studies were included in the meta-analysis if: (1) they were based on case–control or cohort studies, reporting original data; (2) they reported information on the association between tobacco smoking and endometriosis, including estimates of the relative risk (RR) (approximated by the odds ratio (OR), in case-control studies), with the corresponding 95% CIs, or frequency distribution to calculate them; (3) diagnosis of endometriosis was histologically confirmed and/or clinically based. When we found more than one publication based on the same study population and data, we included only the one with most detailed information, or published most recently.
We used the Newcastle-Ottawa Scale22 to assess the quality of individual studies and performed a sensitivity analysis according to the quality of each study.
Data extraction for the meta-analysis
Two authors (FB and SC) reviewed the manuscripts and independently selected the eligible manuscripts; disagreements were resolved by discussion. From each publication we extracted the following information: country of origin; study design; number and characteristics of subjects (cases, controls or cohort size); age, if available; categories of tobacco smoking, if available; measures of association (RR or OR) of endometriosis and corresponding 95% CI for every category of tobacco smoking, or frequency distribution to calculate them; and confounding variables allowed for in the statistical analysis, if any. When more than one regression model was provided, estimates adjusted for the largest number of confounding variables were considered.
Statistical analysis
For some studies, we pooled estimates of different categories of cases or controls using the method by Hamling et al,23 which allows combining of the estimates originally shown in the paper, changing the reference category and taking into account their correlation. We obtained the summary estimates of the RR using the random effect model (ie, as weighed averages on the sum of the inverse of the variance of the log RR and the moment estimator of the variance between studies).24 We assessed the heterogeneity among studies using the χ2 test25 and quantified it using the I2 statistic, which represents the percentage of the total variation across studies that is attributable to heterogeneity rather than chance.26 Results were defined as heterogeneous for p values less than 0.10.
We computed summary estimates for ever tobacco smokers, former smokers, current smokers, moderate current smokers and heavy current smokers, as compared to never-smokers. Different cut-points for moderate and heavy smoking were chosen, depending on those shown in the papers. We also carried out a cumulative meta-analysis to determine whether the association between tobacco smoking and endometriosis changed over time. In the cumulative meta-analysis, studies are added one at a time, ordered by year of publication, and the results are pooled as each new study is added. In the graph, the vertical line corresponding to each year represents the RR and corresponding CI of the results of the meta-analysis of the studies published up to that year, rather than the results of a single study.27 Furthermore, we performed subgroup analyses according to the type of controls (fertile, infertile, both/not specified). Publication bias was evaluated using a funnel plot28 and was quantified by the Egger's test.29
Results
Figure 1 shows the flow chart of the selection of publications. The literature search yielded 1758 reports, of which 1620 were excluded after evaluation of abstract and full text, because they did not report any information on the relationship between tobacco smoking and risk of endometriosis, and 80 because they did not satisfy the inclusion criteria. Moreover, four studies were not comparable with the others, since reported estimates for lifetime smoking30 included former or light smokers in the reference category,11 included women with stage I endometriosis in the comparison group,31 or reported serum cotinine as measure of exposure to tobacco smoking (including passive smoking),32 and thus we excluded those studies from the meta-analysis.

Flow chart of the selection of studies on tobacco smoking and risk of endometriosis included in the meta-analysis.
Furthermore, we excluded 16 studies based on the same data of other included publications.33–48 Thus, in the present meta-analysis we combined data from 38 studies, including a total of 13 129 women with endometriosis (see online supplementary file table S1).3 ,5–10 ,12–14 ,49–76
Online supplementary file table S1 shows the main characteristics of the studies included in the present meta-analysis. Most publications were based on case–control studies, while nine were cohort studies in which, however, the role of smoking was evaluated at the same time of the disease diagnosis,13 ,50 ,52 ,54 ,58 ,70 ,74 except in two cases, in which smoking status was assessed at baseline.5 ,49 Of these, 16 studies were from Europe,3 ,5 ,9 ,10 ,49 ,52 ,54–57 ,60 ,62 ,66 ,68 ,69 ,71 13 from the USA,7 ,12–14 ,50 ,53 ,58 ,61 ,64 ,65 ,67 ,70 ,72 2 from Canada,8 ,63 5 from Asia6 ,51 ,59 ,74 ,75 and 2 from Australia.73 ,76
Twenty-four studies reported information on ever smokers,5 ,7–10 ,13 ,14 ,49 ,50 ,52 ,54 ,56 ,57 ,60 ,61 ,64 ,67 ,68 ,71–76 16 on former smokers5 ,7–10 ,13 ,52 ,54 ,56 ,57 ,61 ,64 ,68 ,71–73 and 30 on current smokers.3 ,5–10 ,12 ,13 ,51–59 ,61–66 ,68–73 Among these, eight reported more categories of current smokers, thus we could calculate separate estimates for moderate and heavy current smokers. We used different cut-points for various study populations, depending on those presented in the papers: thus the cut-point between moderate and heavy smokers was defined as 20 cigarettes per day in five studies,5 ,8 ,53 ,71 ,72 15 cigarettes per day in two studies13 ,58 and 10 cigarettes per day in one study.10
For some studies reporting separate estimates for different types of patients and/or controls, we computed a pooled estimate. In particular, Coccia et al52 reported separate estimates for monolateral and bilateral endometriosis, Heilier et al57 for endometriosis and deep endometriotic nodules, Parazzini et al68 for deep endometriosis, and pelvic and ovarian endometriosis, Signorello et al14 for fertile and infertile controls, and Tsuchiya et al75 for stage I/II and stage III/IV endometriosis. Moreover, Calhaz-Jorge et al5 reported separate estimates for grade I/II and grade III/IV endometriosis, as well as for any type of endometriosis, and the Gruppo Italiano per lo Studio dell'endometriosi,10 including two separate groups of cases and controls undergoing laparoscopy for pelvic pain or infertility, showed separate as well as pooled estimate; in both cases we included the combined estimates in the meta-analysis; further, Pollack et al70 included an operative cohort comprising women scheduled for laparoscopy/laparotomy and an age-matched population cohort of women who underwent pelvic MR for the detection of endometriosis, and we summed up the two groups.
Considering ever smokers or, separately, former smokers, current smokers, moderate smokers and heavy smokers, no statistically significant association emerged (figures 2⇓–4).

Study-specific and summary relative risks (RR) of endometriosis for ever smokers versus never-smokers.

Study-specific and summary relative risks (RR) of endometriosis for current (A) and former smokers (B) versus never-smokers.
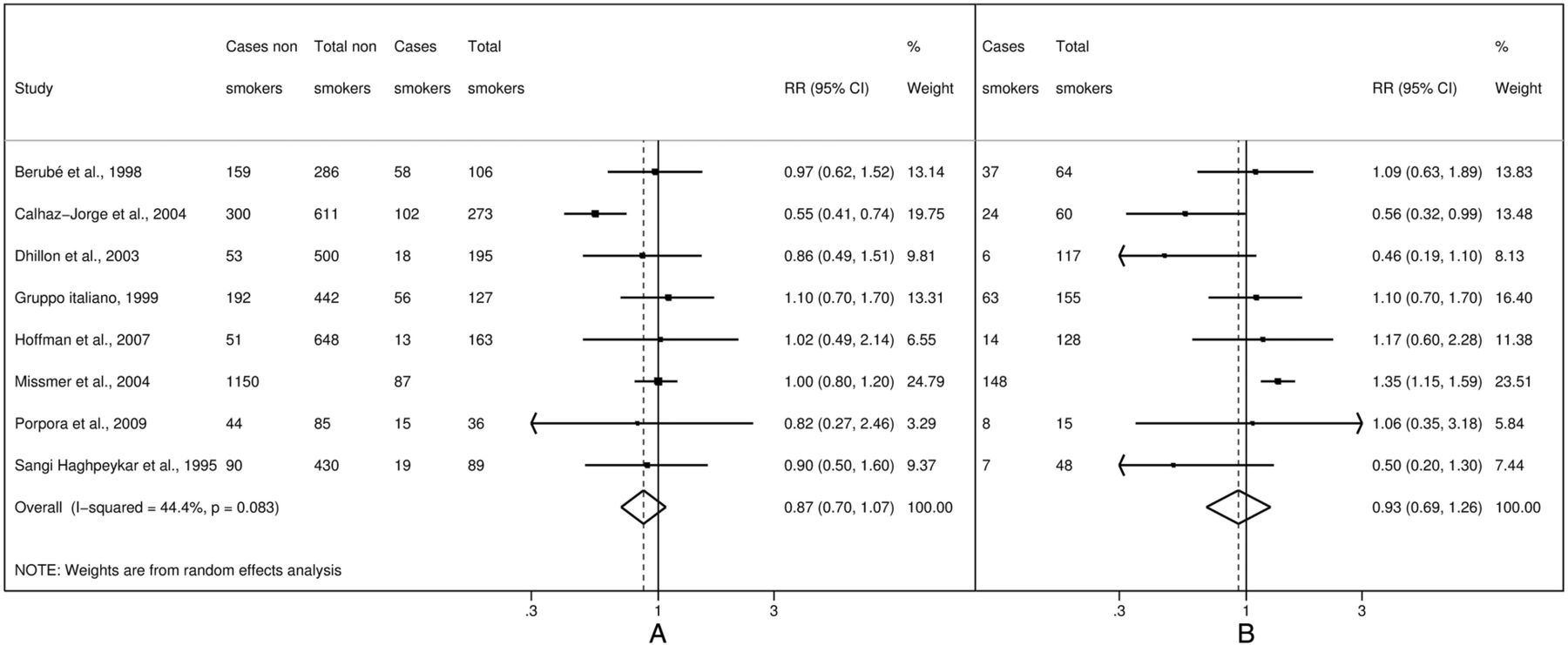
Study-specific and summary relative risks (RR) of endometriosis for moderate (A) and heavy (B) current smokers versus never-smokers.
Figure 5 shows the funnel plot for ever smokers versus non-smokers. There was no evidence of publication bias (p=0.054).

Funnel plot of studies on tobacco smoking and risk of endometriosis (RR, relative risk for ever smokers versus never-smokers).
When we restricted the analyses to nine studies reporting risk estimates adjusted for confounding variables, risk estimates were 1.01 (95% CI 0.86 to 1.19) for ever smokers, 0.94 (95% CI 0.85 to 1.03) for former smokers, 0.87 (95% CI 0.64 to 1.17) for current smokers, 0.85 (95% CI 0.60 to 1.20) for moderate current smokers and 0.90 (95% CI 0.57 to 1.43) for heavy current smokers versus never-smokers.
In subgroup analyses according to type of controls, estimates for ever smokers versus non-smokers were 1.06 (95% CI 0.89 to 1.27) for 7 studies including fertile women, 0.92 (95% CI 0.75 to 1.12) for 7 studies including infertile women and 0.95 (95% CI 0.81 to 1.12) for 14 studies including both or not specified types of controls. Moreover, when we restricted the analyses to studies with cases and controls laparoscopically or surgically confirmed, the risk estimates were 0.97 (95% CI 0.87 to 1.07) for ever smokers, 0.94 (95% CI 0.85 to 1.03) for former smokers, 0.90 (95% CI 0.77 to 1.04) for current smokers, 0.86 (95% CI 0.66 to 1.12) for moderate smokers and 0.97 (95% CI 0.70 to 1.35) for heavy smokers.
Quality score ranged between 2 and 7 (median 4.5). When we restricted the meta-analysis to 19 high-quality studies (with quality score ≥5) the pooled estimates did not materially change (data not shown). Figure 6 shows the cumulative meta-analysis of endometriosis risk for ever smokers versus non-smokers over time, from 1986 to 2014: small variations in the RR estimates emerged over time.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cumulative meta-analysis of studies on tobacco smoking and risk of endometriosis (RR, relative risk for ever smokers versus never-smokers).
Discussion
The present meta-analysis does not support an association between smoking and endometriosis risk. No association emerged considering subgroups of ever, former, current, moderate and heavy smokers, nor in sensitivity and subgroup analyses.
However, this work may be affected by limitations and biases intrinsic to the original observational studies included in the meta-analysis, as well as to the limits that we chose to apply to the bibliographic search, including the restriction to searching PubMed only and the exclusion of languages other than English. Regarding the characteristics of the observational studies, a major concern is the ascertainment of the presence or absence of endometriosis. Some studies compared symptomatic cases with asymptomatic controls, and thus could not distinguish factors related to endometriosis with those associated with pelvic pain or infertility. Moreover, generally asymptomatic controls did not undergo laparoscopy or other surgical procedures, and therefore the presence of asymptomatic endometriosis in these women cannot be ruled out. Another concern is the fact that in some studies diagnosis of endometriosis was self-reported. Thus, a misclassification of cases and controls could not be definitively excluded. However, when we restricted the analyses to women in whom laparoscopy or a surgical procedure had confirmed the presence or absence of endometriotic lesions, we still did not find any significant association between smoking and endometriosis. Further, tobacco smoking is based on patients’ self-reported information, thus some misclassification may have occurred. However, information on tobacco smoking in observational studies has been shown to be satisfactorily reproducible and valid.77–79 For most studies included in the present meta-analysis, only raw estimates were available, since tobacco smoking was not the main topic of the paper and it was only reported as a confounding variable. However, estimates from these studies were similar to those from studies specifically investigating the role of smoking, thus allowing us to rule out major publication bias on this issue. Moreover, we did not find any relevant asymmetry in the funnel plot, and the Egger's test was not statistically significant. Thus, publication bias is unlikely to have appreciably modified the relation between tobacco smoking and endometriosis. Although previous studies have reported an association between endometriosis and menstrual and reproductive factors, such as early menarche,7 ,12 longer duration of bleeding,7 intra-uterine device use,80 or a lifelong regular menstrual pattern of shorter cycles and heavy flows,7 ,12 ,72 ,81 nulliparity or low parity,14 ,30 ,38 ,82 only some studies included in the present meta-analysis have accounted for the role of these factors in the estimate of the relation between tobacco smoking and endometriosis. However, analyses based on adjusted estimates only were comparable to those based on raw estimates.
Since endometriosis is an oestrogen-dependent condition, the inverse association between smoking and endometriosis found in some studies has generally been attributed to the anti-oestrogenic effect of tobacco.83 Some authors have suggested that oestradiol might modulate the mediators of immune system molecules or those involved in tissue cell adhesion and invasion.84 ,85 Moreover, a favourable effect of smoking has been observed in other benign and malignant oestrogen-related diseases, such as endometrial cancer86 and fibroids.87 The antioestrogenic effect of smoking on these conditions could support a protective effect of smoking on endometriosis. Indeed, earlier studies tended to support some inverse association, which, however, declined over time, and accumulating evidence suggests the presence of some false-positive findings in earlier studies.88 Furthermore, tobacco smoking has been associated with female infertility,89 and thus the interpretation of the relation between smoking and endometriosis may be influenced by the role of infertility.
Despite the high prevalence of this condition, the epidemiology of endometriosis still needs to be elucidated for several reasons. Endometriosis is a complex condition in which a genetic contribution and environmental factors seem to be involved.90 Further, it is a disease characterised by an yet poorly defined phenotype. The disease stage depends on the type (cysts, implants, nodules), location (ovary, peritoneum, bladder, ureter, etc), and appearance and depth of invasion of the lesions, which can vary greatly among patients. The clinical presentation can be so variable and the lesions of such diverse morphology that none of the pathogenetic models proposed (retrograde menstruation, coelomic metaplasia, embryological origin) can fully explain the various aspects of endometriosis, and none has been recognised as an ultimately valid explanatory model for all the different forms and manifestations of the disease.90 Moreover, an invasive procedure is needed to diagnose it.90 ,91 Furthermore, published studies differ in the case and control selection and population definition, depending on the choices to consider fertile or infertile cases, and healthy controls or patients with conditions other than endometriosis. Despite these possible sources of variation, the consistency of results observed weighs against any relevant role of tobacco on endometriosis.
In conclusion, the present meta-analysis failed to identify an association between tobacco smoking and endometriosis. However, given the possible limitations of the present study, further studies are needed to evaluate, in depth, the relationship and potential effect of smoking on different type of endometriosis.
Acknowledgments
The authors thank Mrs I Garimoldi for editorial assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online table
Footnotes
-
Contributors FP conceived the idea and planned the research. FB and SC performed the statistical analysis. FB, FC, ER and VC retrieved the data. FP, FB, PV and CLV wrote the entire draft of the article and all subsequent drafts after critical review by all co-authors. All authors gave significant input in the preparation of the article and analysis. FP is the guarantor.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.