Article Text

Abstract
Objectives The present study aimed to evaluate the frequency of warning signs in younger patients with stroke with a special regard to the ‘FAST’ scheme, a public stroke recognition instrument (face, arm, speech, timely).
Setting Primary stroke care in participating centres of a multinational European prospective cross-sectional study (Stroke in Young Fabry Patients; sifap1). Forty-seven centres from 15 European countries participate in sifap1.
Participants 5023 acute patients with stroke (aged 18–55 years) patients (96.5% Caucasians) were enrolled in the study between April 2007 and January 2010.
Primary and secondary outcome measures sifap1 was originally designed to investigate the relation of juvenile stroke and Fabry disease. A secondary aim of sifap1 was to investigate stroke patterns in this specific group of patients. The present investigation is a secondary analysis addressing stroke presenting symptoms with a special regard to signs included in the FAST scheme.
Results 4535 patients with transient ischaemic attack (TIA; n=1071), ischaemic stroke (n=3396) or other (n=68) were considered in the presented analysis. FAST symptoms could be traced in 76.5% of all cases. 35% of those with at least one FAST symptom had all three symptoms. At least one FAST symptom could be recognised in 69.1% of 18–24 years-old patients, in 74% of those aged 25–34 years, in 75.4% of those aged 35–44 years, and 77.8% in 45–55 years-old patients. With increasing stroke severity signs included in the FAST scheme were more prevalent (National Institute of Health Stroke Scale, NIHSS<5: 69%, NIHSS 6–15: 98.9%, NIHSS>15: 100%). Clustering clinical signs according to FAST lower percentages of strokes in the posterior circulation (65.2%) and in patients with TIA (62.3%) were identified.
Conclusions FAST may be applied as a useful and rapid tool to identify stroke symptoms in young individuals aged 18–55 years. Especially in patients eligible for thrombolysis FAST might address the majority of individuals.
Study registration The study was registered in http://www.clinicaltrials.gov (No. NCT00414583).
- HEALTH SERVICES ADMINISTRATION & MANAGEMENT
- EPIDEMIOLOGY
- MEDICAL EDUCATION & TRAINING
- NEUROLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
The present analysis investigated clinical symptoms in young patients with stroke, participants in a unique prospectively collected population of young (18–55 years) stroke victims (Stroke in Young Fabry Patients study; sifap1). A special focus was the analysis of symptoms included in the (face, arm as well as speech and time) FAST scheme. The FAST message is a tool used in awareness campaigns to propagate clinical sign of stroke; it includes weakness of the face and arm, as well as speech and essentially time.
-
The main finding indicates that nearly one-quarter of young strokes is not targeted by the FAST scheme. However, FAST signs are more frequent in patients with acute stroke eligible for thrombolysis. This might be due to increasing stroke severity.
-
The main purpose of sifap1 was not to validate a stroke recognition instrument. The ‘FAST wording’ was primarily not covered with a specific slot in the case report form. FAST items were derived from different sources after the cerebrovascular event (eg, after employing the NIH Stroke Scale immediately after hospital admission). This limitation need to be taken into account when interpreting our results.
-
However, clustering clinical signs according to FAST the majority of patients included in the sifap1 study are targeted. Therefore, FAST may be applied as a useful and rapid tool to identify stroke symptoms in young individuals aged 18–55 years.
-
Since risk factors and aetiology profiles in the sifap1 cohort resembled those found in elderly patients with stroke, conclusions from our study may be also valid in older age groups.
Introduction
Getting patients with stroke to the acute care hospital on time is the major requirement for effective stroke therapy. Knowing warning signs of stroke is the first and most important step in a complex chain towards timely treatment management. Effective public education follows simple rules: the message must be simple to remember, effective and consistent. For this purpose different stroke recognition instruments with different symptoms and different wording have been developed,1–6 offering criteria to identify stroke for public education.1–3 7–9 They are useful for identifying strokes in public,5 ,9 for triage by ambulance paramedics,2 ,3 ,6 to guide paramedics and emergency physicians to direct patients with acute neurological signs to appropriate care for emergency room physicians1 ,2 or as a screening instrument in prehospital stroke research.6 Selection and number of alarming symptoms as well as wording differ; three to six warning signs are usually promoted. Currently many distinguished awareness campaigns to propagate the signs of stroke use the simplified FAST message,9 which adopts weakness of face, arm as well as speech and essentially time (National Health Service: ‘When stroke strikes act FAST’). Although the mnemonic FAST is most frequently adopted, there are so far no prospective multicentre studies from large cohorts, which evaluate distinct stroke signs for the use in public campaigns.
The aim of the present study is to investigate symptoms in acute young patients with stroke with a special focus on signs included in the FAST scheme in a large cohort of younger patients with stroke the Stroke in Young Fabry Patients study (sifap1) and to analyse factors which influence the usefulness in identifying cerebrovascular events (CVEs).10 This is a secondary analysis of the sifap1 data which was originally supposed to investigate the relation of juvenile stroke and a genetic disorder known as Fabry disease. Fabry disease is an X linked storage disorder which might affect the entire body. In sifap1 in 0.9% of all patients Fabry disease was identified.11
Methods
The protocol of the sifap1 study was published recently.10 Described briefly, the sifap1 study was designed as a multicenter multinational prospective observational study of young patients with stroke across Europe (table 1). A total of 5023 patients with stroke (aged 18–55 years) were enrolled in the sifap1 study, 271 patients with primary haemorrhages and 217 patients without classification of the CVE were excluded. All patients or legal representatives gave written consent to inclusion. The remaining cohort of 4535 patients was extensively analysed including detailed medical history, sociodemographics, clinical characteristics, stroke severity, laboratory values, genetics, cardiac work up as well as presenting symptoms on hospital admission. Neurological deficits were measured at the time of maximum impairment according to previous hospital-based stroke registers.12 A transient ischaemic attack (TIA) was defined as a CVE with clinical symptoms lasting <24 h. Cerebral MRI with standardised MRI sequences was a mandatory procedure. Images were assessed centrally at the Department of Neurology, Medical University of Graz, Austria, blinded to clinical and demographic data. Items according to FAST were constructed as follows:
Inclusion criteria of patients in sifap110
Face: facial palsy (minor asymmetry, partial or complete) according to NIHSS item (the scale was assessed within 48 h after admission).
Arm/paresis: left or right arm some effort against gravity, no effort against gravity or no movement according to NIHSS item (the scale was assessed within 48 h after admission) or paresis in arm or leg according to presenting symptoms (documented on inclusion in the study).
Speech: severe aphasia or mute according to NIHSS (documented on inclusion in the study), or dysarthria (mid-moderate slurring, or severe, nearly intelligible or worse) according to NIHSS (documented on inclusion in the study) or dysphasia or aphasia or dysarthria according to presenting symptoms (documented on inclusion in the study).
Based on MRI data clinical signs addressed by FAST were analysed in relation to the different vascular territories. Anterior circulation included the anterior and middle cerebral artery, the posterior circulation the vertebra-basilar territory and posterior cerebral artery.
Apart from NIHSS, the following presenting symptoms were recorded additionally in the case report form on inclusion: headache, nausea-vomiting, hemianopia, diplopia and vertigo. According to the case report form (CRF) 210 out of 1537 patients underwent intravenous thrombolysis. Information about thrombolysis was missing for 2999 patients because this item was included later and not asked for all patients. The indication for thrombolysis was left to the participating centres, according to their local structured operating procedures.
Frequencies of presenting symptoms were analysed in two modifications. At first the number of cases exhibiting FAST symptoms, that is, face palsy or problems with arm/paresis or speech were simply calculated as percentage from the whole cohort. Additionally a Venn diagram was plotted for those with at least one FAST symptom to check frequencies of combinations of symptoms.
Alternatively, the frequency of each symptom was calculated in a sequential approach. After sizing the most frequent symptom, the second frequent symptom was extracted from the remaining cases and so on. This approach allows establishing a ‘hierarchy’ of stroke signs with regard to those symptoms that most often occur aiming to identify as many as possible patients with stroke employing as few symptoms as possible to create a comprehensive public message.
To test differences in subgroups according to age, sex or severity of stroke we used multilevel logistic models to account for the heterogeneity between centres. All analyses were calculated using commercially available software: PASW Statistics 18, Release V.18.0.2 (copyright SPSS, Inc. 2009, Chicago, Illinois, USA) and SAS software, V.9.2 of the SAS System for Windows (copyright 2008 SAS Institute Inc. Cary, North Carolina, USA).
Results
Frequency of presenting symptoms
A total of 5024 patients were enrolled in the study between 2007 and 2010. A total of 4535 patients with TIA (n=1071), ischaemic stroke (n=3396) or other (n=68, refers to cerebral vein thrombosis or no documented entity) were included in the analysis. In general 76.5% of the young strokes included in sifap1 had clinical signs covered by FAST criteria. Table 2 specifies the frequency of FAST symptoms according to gender and age. Face was more frequently affected in men. FAST signs were more prevalent in older age groups; this difference becomes even more obvious in younger patients below 25 years where the capture rate of FAST signs is below 70%.
Frequency of presenting symptoms according to FAST stratified by gender and age
Figure 1 shows the frequency of combinations of FAST symptoms; 34.7% of those with at least one FAST symptom have all three symptoms; 17.3% have only arm problems or paresis; 16.6% have only speech problems and 15.7% have both arm problems/paresis and speech problems. The isolated symptom ‘Face’ is very rare (2.5%).

Venn diagram of FAST symptoms in those with at least one symptom (n=3469).
Symptoms which were registered in the sifap1 cohort but were not considered for FAST are listed in table 3. These stroke symptoms (not included in FAST) also disclosed age and gender differences: headache and nausea were more common in women even after controlling for migraine and age (results not shown), whereas hemianopia, headache, nausea and somatosensory deficits were more common in younger age groups even after controlling for migraine and sex (results not presented).
Frequency of presenting symptoms not accounted for FAST
With increasing stroke severity signs included in the FAST scheme were more prevalent (table 4). FAST signs were less frequent in TIA than in strokes (62.3% vs 81.5%). Severe strokes were nearly completely covered by FAST signs when a NIH score of at least 6 was present. FAST signs occurred in 96.7% of patients who received thrombolysis.
Sings included in the FAST scheme depending on stroke severity, TIA or stroke and eligibility for thrombolysis
Association between presenting symptoms and MRI lesions
A total of 1419 patients had no infarct in MRI, more than half of those patients (56.5%) had a TIA. From those 1419 patients only 65.1% were detected by the FAST items. For 252 patients no information about lesions in MRI was available. For patients with definite infarct lesions in MRI (n=2865) we tested the differences in occurrence of symptoms included in the FAST scheme regarding vascular territories: FAST symptoms were less frequent in patients with strokes in the posterior circulation, where only 65.2% of all cases with an apparent MRI lesion could be identified, whereas 92.4% of anterior circulation strokes matched symptoms included in the FAST criteria. There was no difference between left and right hemispheric stroke (82.9% vs 82.1%).
Hierarchy of presenting symptoms
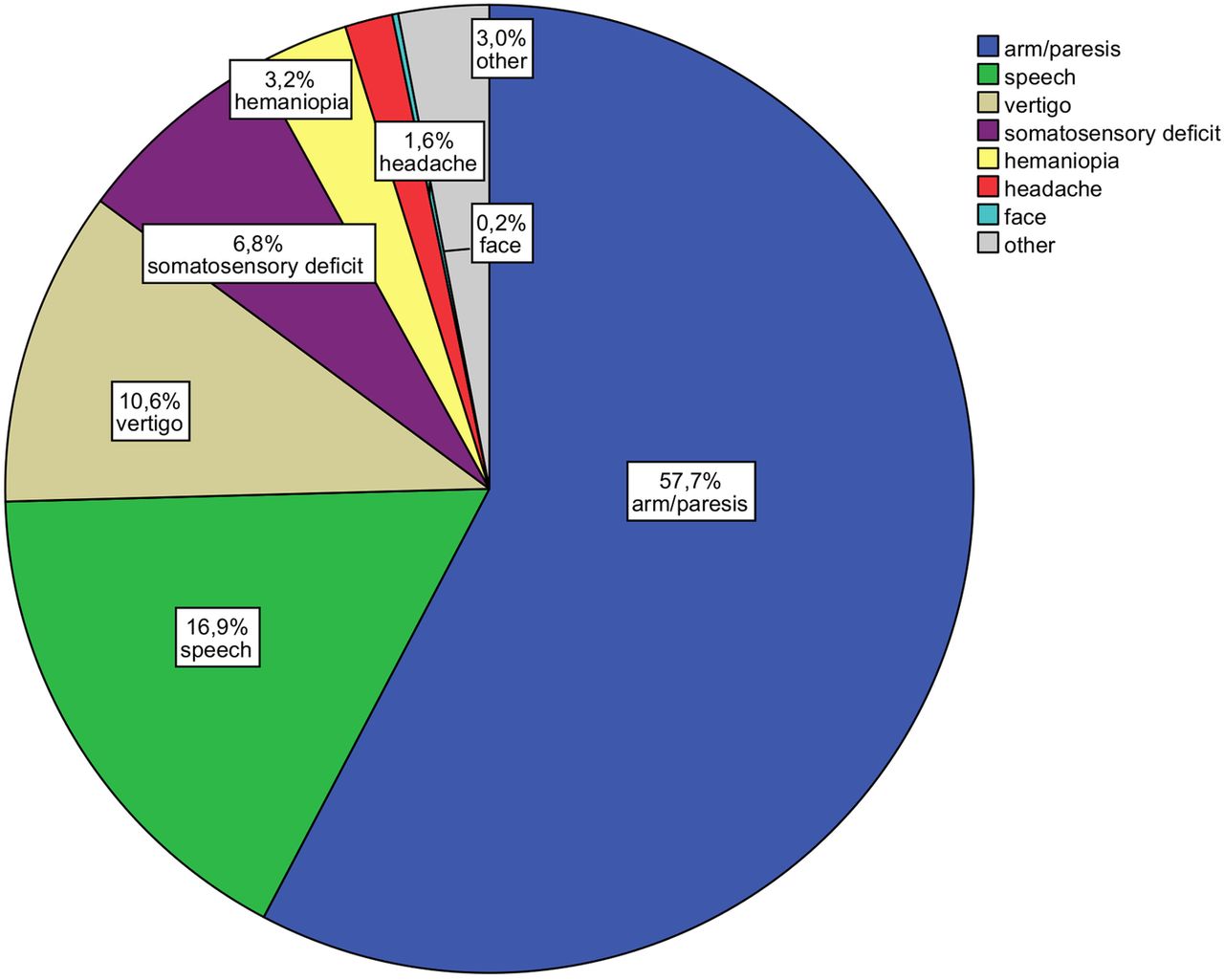
The item ‘arm/paresis’ was by far the most frequent sign in all patients with stroke (aged 18–55 years), and ‘speech’ the second (figure 2). Both items together were covering almost 75% of all recruited stroke and patients with TIA. Under hierarchic perspective the frequency of the ‘face’ item (0.2%) becomes irrelevant if the four most common signs of stroke ‘arm/paresis’ (57.7%), ‘speech’ (16.9%), ‘vertigo’ (10.6%) and ‘somatosensory deficit’ (6.8%) were prior sequentially used as selection criteria.13 ,14 Hemianopia occurred in general with a frequency of 14.4% but only 3.2% of the cases experienced this symptom independent from arm/paresis, speech, vertigo or somatosensory deficits. Common stroke signs in young patients such as headache, leg paresis and diplopia were seldom or not independently differentiated from other stroke signs.
{kind=link}
{kind=link}
Initial presenting symptoms (shown as a percentage of all cases).
Discussion
Principal findings
Frequency of presenting symptoms
In our cohort the FAST symptoms could be traced in 76.5% of all cases. This is notably less than in a previously reported study in which study nurses screened retrospectively the medical records of 3498 stroke cases who presented in an acute care hospital.4 The ‘capture rate’ in this study was 88.9% for all strokes including haemorrhage and even higher for ischaemic stroke and TIA (91.1% and 91.8%, respectively). Interestingly Kleindorfer et al4 found that cases missed by FAST tended to be significantly younger than cases with FAST symptoms (mean 68.9 vs 71.5 years). Even though Kleindorfer et al investigate a general stroke population, in our selected cohort with younger patients (median age 46 years), we observed a comparable trend with significantly fewer patients presenting with symptoms covered by FAST in younger age groups. Therefore, clinical signs included in FAST might be less prevalent in younger patients with stroke.
With respect to FAST signs there was no gender difference in stroke presentation. Other presenting symptoms such as headache, nausea/vomiting and somatosensory deficits occurred more frequently in women. This specific feature could not be explained by larger number of vertebra-basilar strokes in women. Gender differences in these symptoms were also significant when patients with TIA were excluded. In a previous study on gender differences in acute stroke symptoms a higher prevalence of symptoms termed ‘non-traditional’ (pain, mental status change, light-headedness, headache, non-neurological symptoms) could be registered in women.7 However, there were no differences observed regarding traditional symptoms such as hemiparesis, aphasia, facial weakness, hemibody numbness, which is in line with our findings.7
Clinical signs clustered according to the FAST scheme disclosed more patients with stroke with increasing stroke severity. Nearly all cases who received thrombolysis irrespective of gender were indicated by symptoms included in FAST. This is of major interest, because a recent meta-analysis indicated that women with stroke had 30% lower odds of receiving tissue plasminogen activator thought possibly to result from different symptom presentation in women.
Hierarchy of presenting symptoms
‘Arm/paresis’ and ‘Speech’ are by far the most relevant ischaemic stroke signs. ‘Face’ can be quantitatively neglected, because it occurred as an isolated symptom very rarely. Nevertheless, 34.7% of patients with at least one FAST symptom report all three FAST symptoms, meaning that ‘Face’ is rare as an isolated symptom but often accompanied by ‘Arm/Paresis’ or ‘Speech’. Similarly, headache is not relevant to identify ischaemic stroke but may characterise cases with subarachnoid haemorrhage. Remarkably, one single stroke sign (‘Arm/Paresis’) was effective enough to select 86.7% of patients in the subgroup of patients who underwent thrombolytic therapy. However, clinical signs included in the FAST scheme were absent in 23.5% of patients with stroke included in sifap1. Moreover 37.7% of patients with TIA had symptoms other than those mentioned by FAST. Sign included in the FAST scheme were also less frequent in young patients with vertebrobasilar infarctions (64.5%). This is relevant, because ‘non-FAST’ signs are frequently seen as first symptoms of progressing stroke, especially in basilar thrombosis and patients missed by FAST do not necessarily have a benign outcome.4
Other recognition instruments
The ASA Stroke Warning Signs5 emphasise the term ‘sudden’ as prefix, and add a broad spectrum of signs (weakness of face, arm or leg, confusion, trouble speaking or understanding, trouble seeing in one or both eyes, trouble walking, dizziness, loss of balance or coordination, severe headache). This extensive summary of neurological symptoms is likely to cover every brain injury. This kind of messaging takes advantage of the fact that acute onset (‘sudden’) is the most discriminating factor between stroke and non-stroke and targets 96% of all strokes and TIA but can include 47% of differential non-stroke diagnoses.1 The Cincinnati Prehospital Stroke Scale (CPSS)3 is a 3-item scale derived from a simplification of the National Institutes of Health (NIH) Stroke Scale. It evaluates facial droop and arm drift, speech is tested by asking the patient to repeat sentences. Thereby the CPSS design is very similar to FAST9 and its reproducibility has proven excellent among prehospital care providers.3 In agreement with our findings, the CPSS has also proven high validity to identify candidates for thrombolysis and strokes preferably in the anterior circulation. The Los Angeles Prehospital Stroke Screen (LAPPS)2 considers unilateral motor weakness (‘facial smile/grimace’, hand grip and arm strength/drift) as well as four screening criteria (Age >45, history of seizure disorder absent, symptoms duration less than 24 h, not wheelchair user or bedridden prior to the event) and a glucose measurement. It was designed to allow prehospital personnel to rapidly identify most common patients with stroke and exclude those unlikely to qualify for or benefit from acute interventions. Thereby patients with stroke below 45 years or with longer symptom duration were purposefully not targeted. The Melbourne Ambulance Stroke Screen (MASS)6 combines clinical signs of the CPSS with the LAPPS screening criteria. The ROSSIER scale1 lists five key signs scoring positive (asymmetric facial/arm/leg weakness, speech disturbances and visual field defect) and two items scoring negative (loss of consciousness and syncope, seizure activity) adding to a total score ranging between −2 and +5. The purpose of the ROSSIER design was to develop a simple and practical instrument for emergency room physicians in order to reduce the number of non-stroke referrals from emergency room to stroke unit.
Stroke recognition instruments must be differentiated with regard to the addressee. For public education and campaigns there is no choice but to promote a selected number of clinical signs. Additional assessments (ie, glucose measurements) to rule out non-strokes or stroke subgroups are reserved for paramedic use or for triage purposes in hospital.
Strengths and weaknesses of the study
The sifap1 study is by far the largest prospective multicenter study analysing presenting stroke symptoms in the young with broad clinical work up including MRI. Age limit up to 55 years allows exploring subgroups with increasing age including patients with risk factor and aetiology profiles resembling those found in elderly patients with stroke.10 Therefore, the findings may be extrapolated to some extent to the stroke population in general. Nevertheless there are some limitations regarding this study: The main purpose of sifap1 was not to validate a stroke recognition instrument. Therefore, ‘FAST wording’ was primarily not covered with a specific item in the CRF. Instead we asked for paresis directly after CVE and employed the NIH Stroke Scale immediately after hospital admission (median delay: one day). Assessments ruling out stroke mimics (ie, blood glucose level) influence specificity but cannot be used for public education.6 Since we excluded stroke mimics by definition, our study is not designed to calculate for positive and negative predictive values of distinct stroke signs. Moreover, there is a problem in general to calculate for false-negative diagnoses, that is, undiagnosed strokes in a population under survey. It has to be noted also, that we did not consider haemorrhage, subarachnoid haemorrhage or venous thrombosis in our calculations. Addressing all these strokes types may further add to complexity and dilute the awareness message. The FAST scheme was develop to screen for potential stroke victims in a preclinical setting.9 In contrast our patients were included after admission to a neurological department. This needs to be taken into account when interpreting our results.
Extensive MRI documentation allowed us to validate the clinical stroke diagnosis and constituted a robust additional aspect in identifying presenting symptoms in acute young patients with stroke. One-third of vertebra-basilar strokes and transient attacks could not be visualised on MRI. In these cases the appraisal of an experienced neurologist was decisive. Notably, there was no relevant difference regarding signs included in the FAST scheme comparing patients with and without proven MRI lesions.
Implications for public campaigns
Instruments that help the lay public to identify stroke in prehospital setting are elementary to trigger early treatment. Our study in patients with stroke (aged 18–55 years) proves that symptoms considered in the FAST scheme may be useful for identifying young patients with stroke. Especially young patients with stroke eligible for thrombolysis might be targeted by a FAST evaluation. In contrast, clustering only clinical symptoms according to FAST, it might be less effective in young patients with stroke with TIA and infarcts in the posterior circulation. Since risk factors and aetiology profiles in the sifap1 cohort resembled those found in elderly patients with stroke,10 conclusions from our study may be also valid in older age groups.
Design and usefulness of stroke recognition instruments depend strongly on the context and the target group to be addressed. The proper diagnosis of stroke requires profound clinical knowledge, which cannot be expected from lay persons or ambulance paramedics. On one hand simplified but specific signs are needed for public campaigns, on the other hand stroke recognition in prehospital settings cannot be simplified without losing a substantial number of patients. Obviously, signs such as ‘Vertigo’ and ‘Somatosensory Deficits’ target much more patients with stroke but coincidently capture more stroke mimics and thereby dilute the message and burden the healthcare system.
It is important to recognise that sudden neurological symptoms need expeditious referral and neurological expertise, because sudden neurological diseases other than stroke may represent emergencies as well. Messaging in public awareness programmes is therefore subject to more complex considerations. Besides catchy wording, frequency of symptoms, capture rates and positive and negative predictive values, the capacity and readiness of regional healthcare systems to cope with stroke mimics will enhance public campaigns.
Acknowledgments
The authors thank especially Kristin Brüderlein, Ines Federow, Doreen Niemann, Gesine Makowei, Frances König, Jan Burmeister, and Carla Biedermann for organisational aspects. In particular, Sabine Rösner and Susanne Zielke spent a lot of effort in realising the entire workflow. Elmar Beck (Anfomed GmbH, Möhrendorf, Germany) programmed the web-based data bank as well as hosted the data.
References
Footnotes
MK, UG and CT contributed equally.
-
Contributors The concept of the present analysis was developed by MK. MK and UG analysed the data. UG conducted the statistical analysis. MK, UG and CT were responsible for the development of the manuscript. AR initiated the sifap1 study. GJ, TT, JP, CT participated in the data acquisition. MK, UG, GJ, TT, CK, RS, PJ, BN, AR and CT were responsible for the intellectual discussion, review, analysis and interpretation of the results. MK, UG, GJ, TT, CK, RS, PJ, BN, AR and CT contributed with substantial and important intellectual content in drafting and reviewing the manuscript.
-
Funding The sifap1 study (Stroke in Young Fabry Patients, http://www.sifap.eu; http://www.clinicaltrials.gov: No. NCT00414583) has been supported partially by an unrestricted scientific grant from Shire Human Genetic Therapies.
-
Competing interests None.
-
Ethics approval The design of the study was approved by the ethics committee of the Medical Association Mecklenburg-Vorpommern (board 2), Medical Faculty, and University of Rostock. Approval of the local ethics committees was obtained in all participating centers. The study was registered in http://www.clinicaltrials.gov (No. NCT00414583).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data available.