Article Text

Abstract
Objective To synthesise the evidence on implementing family involvement in the treatment of patients with psychosis with a focus on barriers, problems and facilitating factors.
Design Systematic review of studies evaluating the involvement of families in tripartite communication between health professionals, ‘families’ (or other unpaid carers) and adult patients, in a single-family context. A theoretical thematic analysis approach and thematic synthesis were used.
Data sources A systematic electronic search was carried out in seven databases, using database-specific search strategies and controlled vocabulary. A secondary manual search of grey literature was performed as well as using forwards and backwards snowballing techniques.
Results A total of 43 studies were included. The majority featured qualitative data (n=42), focused solely on staff perspectives (n=32) and were carried out in the UK (n=23). Facilitating the training and ongoing supervision needs of staff are necessary but not sufficient conditions for a consistent involvement of families. Organisational cultures and paradigms can work to limit family involvement, and effective implementation appears to operate via a whole team coordinated effort at every level of the organisation, supported by strong leadership. Reservations about family involvement regarding power relations, fear of negative outcomes and the need for an exclusive patient–professional relationship may be explored and addressed through mutually trusting relationships.
Conclusions Implementing family involvement carries additional challenges beyond those generally associated with translating research to practice. Implementation may require a cultural and organisational shift towards working with families. Family work can only be implemented if this is considered a shared goal of all members of a clinical team and/or mental health service, including the leaders of the organisation. This may imply a change in the ethos and practices of clinical teams, as well as the establishment of working routines that facilitate family involvement approaches.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
Can inform policies and guidelines on family involvement so that they impact on routine practice.
-
Is novel in covering a wide range of family involvement practices, highlighting common barriers, problems and facilitating factors.
-
Synthesises rich qualitative data from professionals, patients and families.
-
Could not include subgroup and quality analyses, due to the high correspondence between type of family involvement practice and methodology.
-
May be conceptually limited as extant research has focused on perspectives of staff involved in family work and few studies are available on families’ views.
Background
The process of deinstitutionalisation of mental healthcare in the western world has led to families and others in the community shouldering the psychosocial burden of care and informally adopting the role previously provided by professionals in healthcare services.1–3 The adoption of protected terms such as ‘carer’ in the UK and ‘caregiver’ in the USA is a response to the substantial, yet ‘non-professional’ role that individuals in a close relationship have in supporting a person receiving mental health treatment. The term may include parents, partners, siblings, children, friends or other people significant to the individual: essentially, anyone who provides substantial support without being paid. The term carer can be problematic, being considered by some to have connotations of dependency and of minimising the significance of the relationship.4 Also, many ‘carers’ do not self-identify as such, and consider their caring role as being within the traditional responsibilities expected of them. To avoid confusion when referring to family-directed initiatives, the single term ‘families’ will be adopted throughout this review and broadly applies to a person's social network, not excluding their non-blood relatives.
‘Family involvement’ in mental health services can take different forms, depending on the level of need and availability of services. Generally, it can be conceived on a spectrum from more basic functions to specialised interventions, the minimal level including the provision of general information on the mental health service and assessments. On a more complex and specialised level, services can offer families psychoeducation, consultation, family interventions (FIs) and therapies.5 There are both strong economic and moral imperatives to establish meaningful involvement and true collaborative working between families and health professionals. These are recognised by international government policies and psychiatric guidelines stipulating that families should be supported and actively involved in psychiatric treatment.6–11 Families can encourage engagement with treatment plans, recognise and respond to early warning signs of relapse12 and assist in accessing services during period of crisis.13–15 Family involvement can lead to better outcomes from psychological therapies16 and pharmacological treatments,17 fewer inpatient admissions, shorter inpatient stays and better quality of life reports by patients.18–21
However, despite the vast evidence base for FI22–28 and family psychoeducation,29 research suggests that family involvement is often not implemented in routine mental healthcare. There is an abundance of both quantitative and qualitative studies into experiences of inpatient care reporting that families feel marginalised and distanced from the care planning process. Common themes across international studies indicate that families feel isolated, uninformed, lack a recognised role and are not listened to or taken seriously.1 ,30–43 Families also commonly report feeling that confidentiality is used by professionals as a way to not share information.39 ,44 Family Intervention as a treatment approach is startlingly under-implemented, with extremely low numbers of families actually receiving it in clinical services.11 ,45–47 It is the case that for many, contact between professionals and families remains limited to telephone calls during crisis periods.48
Why is family involvement in treatment so under-applied? There has been much debate about the reasons (eg,22 ,49–51) and some suggest they are linked to general problems of implementing new evidence-based practices in clinical services.29 Other proposed barriers are more specific to family interventions, such as the danger of increasing burden related to caregiving, role strain, lack of experience and/or interest52 and the complexities of navigating confidentiality.53 Such discussions are largely speculative and reviews of evidence tend to focus on the provision of specific interventions, such as family psychoeducation29 or FI.54 This systematic review aims to assess how the involvement of families is implemented in the treatment of patients with psychosis, taking a broad view of involvement as described above in order to capture the barriers, problems and facilitating factors that operate in practice. In doing so, this may help to better define and implement families’ involvement in psychiatric treatment in the future.
Methods
The full protocol for this systematic review is reported in the online supplementary file 1.
Identifying relevant studies
Computerised databases were searched for eligible studies: MEDLINE, EMBASE, PsycINFO, AMED (via Ovid), BNI and CINAHL (via HILO), Social Sciences Citations Index (via Web of Knowledge) and CDSR, DARE and CENTRAL (via the Cochrane Library). Word groups representing patient diagnosis, intervention and involvement terms and outcome descriptors were combined in several ways. Strategies were adapted for each database, using controlled vocabulary (MeSH, Emtree, Thesaurus of Psychological Index Terms) and free text (see online supplementary file 2). The search was last repeated on 1 June 2014.
Publication bias was minimised by including conference papers and book chapters, searching grey literature for dissertations and reports (ETHOS, SIGL) and corresponding with authors to identify further works. Both backward snowballing (from the reference lists of included studies and identified reviews) and forward snowballing (finding citations to the papers) was conducted.
Inclusion procedure
A study was eligible for inclusion if: (1) it was an original collection of data; (2) situated in primary or secondary mental health services; (3) the patient population included people being treated for psychotic disordersi; (4) the intervention involved tripartite communication between health professionals (any), families (unpaid carers) and adult patients, excluding those focused exclusively on professional–family communication, family–family communication or multiple-family groups; and (5) results described barriers, problems and/or facilitating factors in involving families in treatment. No study type was excluded, however only Latin-script languages were able to be translated.
‘Barriers’ were defined as factors that prevented an approach from taking place or limited the scope of it, ‘problems’ referred to issues that emerged when delivering an approach and ‘facilitating factors’ were considered to be any factors that aided implementation or delivery. ‘Family involvement’ was defined inclusively as any process allowing health professionals, families and patients to actively collaborate in treatment, such as in making joint treatment decisions. Studies not reporting clear information on how families were involved in treatment were excluded. Studies into general experiences, opinions, satisfaction or needs were also excluded, unless they related to a clearly described specific involvement in treatment.
Two reviewers (EE and DG) screened all of the titles and collected relevant abstracts. These were screened and then excluded if they did not fit the selection criteria. Studies that seemed to include relevant data or information were retrieved and their full text versions analysed and examined for study eligibility. All final full text choices were confirmed and agreed by both reviewers.
Method of analysis
Data extraction and synthesis was guided by the Economic and Social Research Council (ESRC)'s Guidance on the Conduct of Narrative Synthesis in Systematic Reviews.55
The included studies used both qualitative and quantitative methods, yet clearly had conceptual overlaps despite reporting results in different formats. Any available quantitative data were usually descriptive, reported in addition to qualitative findings and were largely used to explore existing themes or concepts. It was therefore considered appropriate to transform quantitative findings into qualitative form to systematically identify the main concepts across the studies using thematic analysis.55 ,56 The use of this method is increasingly being advocated with studies involving data that are quantitative or from mixed methods56–58 to address questions relating to intervention need, appropriateness and acceptability in systematic reviews.59
Data extraction and synthesis
Theoretical Thematic Analysis60 using inductive themes to identify the barriers, problems and facilitating factors of family involvement was used as a framework to explore further themes.
Two non-clinician researchers (EE and AD) independently extracted author interpretations and participant data from the included studies using a piloted data extraction sheet. They then separately allocated the findings to relevant sections of the framework (eg, ‘Barriers according to staff perspectives’) and coded the data within each section. Identified categories (eg, ‘Unsupportive attitudes of managers’) were aggregated into subthemes (eg, ‘Attitudes towards family work’) and finally became grouped under overarching themes (eg, ‘Context: addressing the organisational culture’). These emerging themes were discussed throughout analysis along with a clinician-researcher (DG), and discrepancies were resolved through iterative discussions. Robustness of the synthesis was investigated and themes were checked for completeness. Two clinician-researchers (DG and SP) acted as third party assessors of the final data synthesis.
Results
Included studies
Database searching produced 15 615 titles to screen. After removing duplicates and irrelevant papers, a full text assessment of 119 documents was conducted. Twenty eight publications met our inclusion criteria and second stage searching including grey literature searching, personal correspondence and snowballing techniques led to the further identification and inclusion of 15 articles. This brought the final number of studies to 43. The PRISMA flow chart in figure 1 depicts the identification and exclusion of articles.

PRISMA flow diagram for paper selection.
Overview of papers
Forty-two papers were published between 1991 and 2013 and one in 1978. Just over half of the studies were based on UK findings, with the rest from Finland, the USA, Italy, Australia, Canada, Germany, India, Ireland, New Zealand, Spain, Greece and Portugal. Mainly, papers reported on experiences of implementing FI approaches (n=33). Typically these followed a similar structure and were broadly modelled on the Behavioural Family Therapy approach61 (see online supplementary file 3 for full study characteristics). This included variations such as ‘Psychosocial Intervention’ and ‘Family Psychoeducation’ that fit the model of an FI. The remainder explored Open Dialogue approaches (n=6), Systemic Psychotherapy (n=3) and one purely Behavioural Therapy programme. The vast majority were cross-sectional studies and 13 were naturalistic evaluations, descriptions or case studies of a service. In all, 37 papers explored staff perspectives, eight papers featured patient perspectives and six featured ‘family’ perspectives. In total, the review included data of 588 professionals, 321 patients and 276 ‘family members’ or ‘families’.
In depth review: synthesis across studies
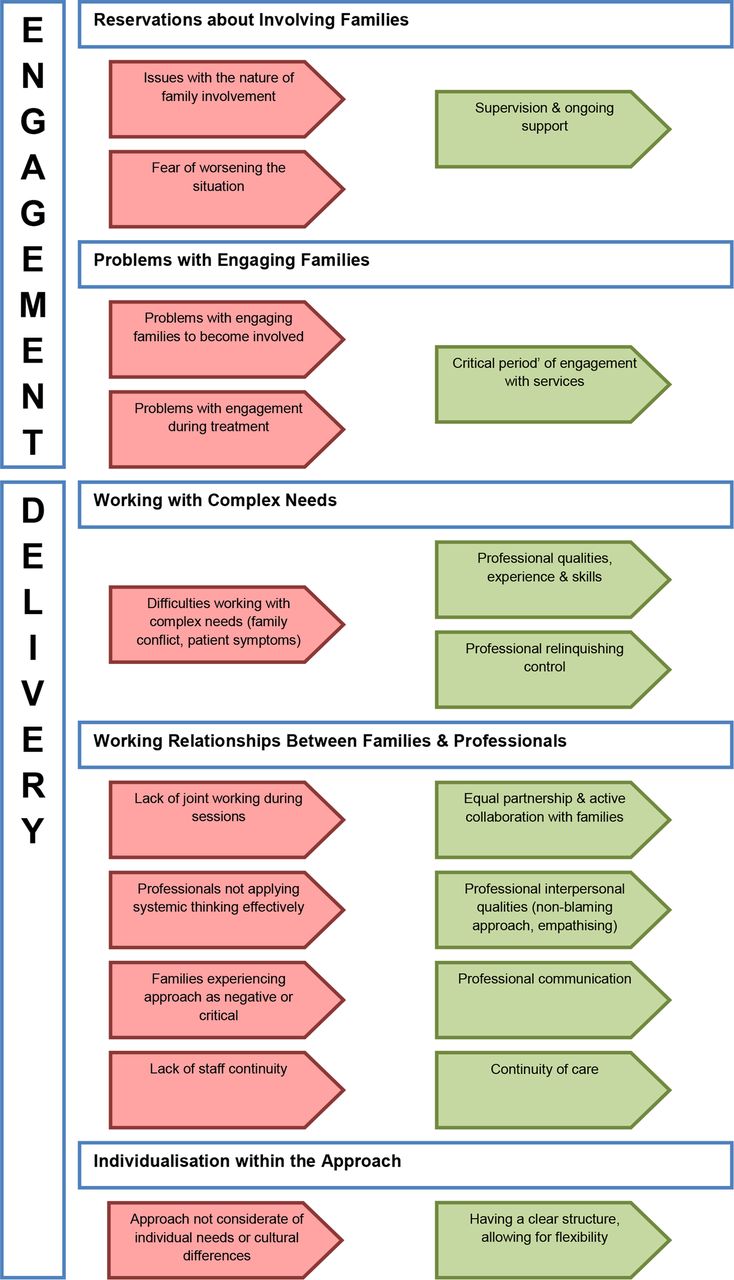
Figure 2 summarises the final cross-study synthesis: the identified barriers/problems (in red) and facilitating factors (in green) and the themes in which they seemed to be operating. The themes closely relate to temporal sequencing in the process of delivering an intervention: the context, engagement and then delivery. The figure provides a visual representation of the matches and gaps between barriers and facilitating factors related to involving families. This is for the most part conceptual, as barriers and their direct facilitating factors may not have been discussed in the same study. The themes and subthemes are explored in greater detail in the synthesis below, which includes details of problems associated with delivering approaches that involve families as well as barriers and facilitating factors of this work.

Barriers, problems and facilitating factors related to family work. Summary of themes.

{kind=link}
{kind=link}
{kind=link}
Continued
Context: addressing the organisational culture
This theme reflects the majority of the findings, mostly from staff perspectives. Their experience of implementing family work could be characterised as working in relative isolation in a system where colleagues and managers did not value and prioritise family involvement or were openly hostile to it. With multidisciplinary cooperation and working systems not in place, practical burdens associated with family work were sometimes insurmountable. Mirroring this, factors that enabled family involvement to take place were related to top-down management support, prioritisation and changing the culture of family work.
Organisational attitudes and paradigms
This subtheme covered general attitudes, such as family involvement not being valued at organisational and team level but also highlighted possible entrenched reasons for this. For example, individualistic, biological paradigms made family work seem secondary or optional62–64 and staff found it difficult to adopt a collaborative stance, relinquishing the role of didactic problem solver.63 In some cases, it appeared that historical negative attitudes towards families had not shifted.62 ,64 Attitudes against family work described among colleagues ranged from resistance towards the approaches63 ,65–68 to well-intentioned but complicating beliefs regarding clinicians’ duty towards the patient.64 ,69 ,70 Facilitating factors related not only to specific strategies but to an overall shared culture and prioritisation of family work,64 ,71 ,72 shifting attitudes towards viewing the family as equal partners71 ,73 and thinking more systemically about problems.71 ,74
Practical needs associated with family work
Overwhelmingly, staff reported on the practical burdens of family work: that it requires time, resources and funding and is difficult to integrate with other clinical casework,62 ,64–70 ,73 ,75–87 particularly in areas with high demands and clinical crises.73 ,82 ,83 Specific needs reported for family work included flexible hours64 ,65 ,67 ,70 ,80 ,82–84 87–90 and the accommodation of family requirements such as childcare facilities80 or home visits.82 ,89 ,91 A lack of systems and structure for carrying out and recording family work was also reported as a barrier to implementation and problem during delivery.63 ,87 ,92 This included a lack of coordination between inpatient and outpatient care.62 These issues were compounded by reports of services and managers not making time allowances for family work, for example, not providing time in lieu for out of hours work,64 ,65 ,77 ,83 ,84 or obstructing time use, for example, by refusing the release of staff for training.63
Management culture
Commonly, staff reported on the unsupportive attitudes of managers and colleagues as limiting the implementation of family involvement.63 ,64 ,66 ,77–79 ,87 ,92 ,93 This ranged from a ‘management culture of benign neglect rather than of active opposition’93 to overt challenges such as not respecting ring-fenced time for family work.87 The strongest facilitator seemed to be that of strong leadership through senior management support and developing strategic solutions. This ‘sanctioned’ family work, giving it core priority status within the service,64 and could facilitate specific powerful initiatives such as writing family work into business plans, policies and job descriptions of all staff.63 ,79 Further endorsement came from providing flexible hours, creating new staff roles and financial provision.63 ,73 ,79 ,94 The value emerged of having regular multidisciplinary meetings to address team-specific needs72 ,78 ,79 ,88 and developing strategies that prioritised family work and made it a part of regular clinical practice.63 ,72 ,73 ,79 ,88 ,94 This included having routine assessment of all families, asking clinicians about families when reviewing caseloads and providing regular feedback of family data to teams and managers.63 ,94
Training needs
Staff also reported on lacking access to adequate supervision and training62 ,63 ,65 ,66 ,83 ,86 ,87 ,92 as barriers to implementation. This may link with reports of staff lacking skills or confidence to do the work.62 ,64 ,85 ,86 ,92 Some problems during delivery (such as managing family dynamics64 ,65 ,70 ,74 ,78 ,88 ,95) could also be related to staff skills and experience.71 ,78 ,81 As expected, having a structured regime of supervision, encouraging attendance and ongoing support was described as helping staff to deliver work with families.63 ,72 ,78 ,79 ,88 Staff also reported on the value of belief in the approach and having an identity in their role.71 ,72 ,79 ,81 ,86
Team attitudes, commitment and multidisciplinary cooperation
Difficulties arose when only a minority of team members had been trained in an intervention.82 Staff reported that collaboration was often lacking63 ,65 ,69 ,73 ,77 ,80 and that involving families requires whole team commitment.76 ,82 ‘Ownership’ was sometimes an issue, with various staff groups perceiving family work as within the domain of other roles, not theirs.69 ,80 Role and team-specific issues also emerged, such as psychiatrists, inpatient staff and home treatment teams being less involved.63 ,66 ,73 ,81 Collaboration in the form of multidisciplinary coworking, peer-supervision and whole team approaches were all reported as aids to implementing family work.63 ,66 ,71–74 ,78 ,79 ,82 ,88
Problems with finding ‘appropriate’ referrals were reported widely.65 ,67 ,68 ,77 ,78 ,80 ,82 ,83 ,93 While some patients do not have families, the pervasiveness of this response also called into question staff members’ pre-existing ideas about what constitutes an ‘appropriate’ family for intervention. Staff reported the resistance of other professionals to make referrals,67 ,88 family work services being ‘forgotten’ and referrals being made as a ‘last resort’, by which time the families themselves may have grown resistant.93 Acting as a facilitator was the promotion of family work, both as a cascading effect through colleagues and across services.64 ,79 ,87
Engagement: addressing concerns through openness, encouragement and building alliances
The next theme related to the process of engagement, informed more broadly by both staff and family responses. A picture emerged of families sometimes being reluctant to engage, and of valid concerns. Yet the successful establishment of trusting relationships indicates these concerns may be surmountable in many cases.
Reservations about involving families
Similar issues around the nature of involving families emerged as a barrier to families becoming involved and as problems during treatment. Some concerns seemed linked to fears around power and control: bi-directional privacy concerns (keeping the extent of the illness from the family and keeping family issues from services)70 and patients’ fears of placing relatives in a position of power70 ,95 or of exposing their vulnerability.75 Responses in all three participant groups addressed the need for an exclusive patient–professional relationship.69 ,70 ,76 ,95 Existing individual and family problems (such as patients’ symptoms being directed at family members62) also precluded family involvement. Both families and staff expressed fears of making the current situation worse, such as by burdening the family and worsening the patient's symptoms.70 ,80 ,84 ,86 ,91 Professionals described building trust and rapport, through open discussions with the family, acknowledging concerns and providing reassurance.71 ,74 ,88 ,91
Problems engaging families
These were often unspecified as scepticism, lack of motivation or refusal from the families, occurring prior to engagement or during treatment.65 ,76 ,78 ,83 ,84 ,88 ,93 ,96 As professional responses, these may reflect their attitudes towards families as unmotivated, but could also describe the failure of the team to mobilise the family in favour of treatment.96 A factor described as a facilitator was having a critical period of engagement: intensive efforts at contact and involvement early on after contact with services93 ,96–99 and presenting the approach enthusiastically71 ,89 functioned to establish collaborative relationships between families and professionals as the modus operandi.
Delivery: active collaboration, professional skills and respect for families as individuals
The final theme related to factors that affected how staff members delivered FIs and how families experienced them. As a whole, both family and staff responses highlight the importance of respectful, equal partnership, enhanced by professional skills and experience.
Working relationships between families and professionals
Collaboration between families and professionals on an equal footing appeared valued by both families and professionals. Lack of collaboration was cited as a problem during delivery, resulting in families feeling patronised or not understood.76 Open Dialogue papers particularly emphasised the lack of success when actions were unilaterally decided, rather than emerging from a joint process.74 ,99 Factors helping to overcome this included being able to relinquish control, that is, tolerate uncertainty in order to allow a joint solution to emerge,78 ,96 ,98–100 approaching the family on an equal basis71 and actively collaborating with families during meetings.66 ,71 ,89 ,92 ,96
How families experienced an approach closely linked with their experience of the professional. Some families reported experiencing an approach as negative or critical, both through the model itself for example, its characterisation of illness,101 or experiences of the professional, perhaps as criticising parenting.101 ,102 Yet, the interpersonal qualities of the professional and the establishment of a therapeutic alliance strongly emerged as facilitating factors: professionals being informed, genuine, warm, non-blaming71 ,89 ,101 and demonstrating an awareness and understanding of the problems of the whole family.71 ,79 ,89 ,90 ,99
A lack of continuity was cited as a problem,99 while a facilitator was having the same team involved from the beginning and staying with the family throughout the treatment process.96 ,98 ,99
Individualisation within the approach
Approaches were sometimes described as culturally insensitive:76 ,88 rigid, manualised approaches did not meet the general needs of particular groups while individual needs, such as illiteracy, were sometimes not catered to.64 ,76 ,97 ,103 Professionals and families valued having a clear structure while allowing for flexibility.71 ,76 ,88 ,99 Professionals’ skills were also important, by way of communicating information in an easy-to-understand format, avoiding jargon71 ,88 ,89 ,99 and developing an individualised and contextualised approach.71 ,76 ,88 ,93 ,99
Working with complex needs
Professionals highlighted the complexities of working both with families and with patients with psychosis. The difficulties of managing patient symptoms and working in a meaningful way with their beliefs73 ,104 may be compounded by family dynamics64 ,65 ,70 ,74 ,78 ,88 ,95 ,104 and potentially relatives’ own emotional and affective problems.104 Staff members’ qualities, skills and experience in the area were naturally described as facilitating factors.71 ,76 ,78 ,79 ,81 ,83 ,89 ,90 ,100 Perhaps unsurprisingly, useful skills were described as working creatively to overcome barriers, hypothesising, reflecting and persevering.71 ,79 ,100
Discussion
Main findings
Our results suggest that having ‘top-down’ support and training some staff members to carry out family work is necessary but not sufficient. In order to effectively implement family involvement in care, all members of a clinical team should be trained and regularly supervised and a ‘whole team approach’ should be used. Developing a clear structure for the intervention may be beneficial for the delivery of family involvement, provided that flexibility to accommodate individual needs is ensured. Concerns emerged regarding privacy, power relations, fear of negative outcomes and the need for an exclusive patient–professional relationship. Exploring and acknowledging such concerns through open, yet non-judgemental communication could facilitate the establishment of a therapeutic alliance between staff, families and patients.
These findings may help to explain why family interventions—despite their overwhelming evidence base and their inclusion in practically all policies and guidelines—are so poorly implemented in routine practice. The requirements identified may be challenging given that family-oriented practice may need to be embraced by a whole organisation and included in work routines in order to be implemented.
Strengths and limitations
To our knowledge, this is the first systematic review that specifically focused on barriers, problems and facilitating factors for the implementation of family involvement in the treatment of patients with psychosis. This is of high importance given the current climate of government policies and psychiatric guidelines stipulating that families should be supported and actively involved in psychiatric treatment,6–11 and the disappointments in achieving this in practice so far. The search strategy allowed for the capture of a large number of studies, different researchers independently extracted and reviewed the data and when necessary authors were contacted to clarify ambiguous information. The use of thematic analysis, described as having the ‘most potential for hypothesis generation’,108 allowed for understanding the larger picture, which is more than the sum of its findings. While interpretative, this process has been carried out in accordance with RATS guidelines61 and presented transparently. Though some themes were not highly recurrent—for example, criticisms of manualisation emerged only in structured approaches such as Behavioural Family Therapy—in all, findings were complimentary, not contradictory. The fact that common themes emerged in spite of variations in approach, across 16 countries, speaks for the robustness of the findings as representing shared issues with family involvement.
However, a number of limitations must be considered when interpreting the results of this study. Methodologically, conducting subgroup analysis, that is, for different intervention models, was not considered viable due to the strong association between type of approach and methodology used for example, Open Dialogue with case studies and Behavioural Family Therapy with the Family Intervention Schedule (FIS) questionnaire. Carrying out a subgroup analysis may have therefore had the risk of mischaracterising certain approaches due to variation in the richness of data. While there are well-established methods for assessing the quality of intervention studies, this is not the case for studies of implementation processes, qualitative or mixed methods research56 and the use of appraisal tools in qualitative research remains contentious.109 ,110 The decision not to use quality-based analysis was therefore also based on recognition of the important contribution and explanatory value that descriptive accounts offer. Despite efforts to find grey literature, the search strategy may still have been limited in its bias towards published research, yet the nature of this review topic means that service level audits and evaluations are likely to be of relevance. Conceptually, the dominance of staff and academic perspectives may have led to barriers within the organisation being explored most thoroughly, however does not lead to the conclusion that there are no inherent problems with involving families in clinical settings.
Comparison with available literature and implications for practice
Our findings reflect important key features for implementation of evidence-based practices, already identified in previous research in implementation science, such as top-down input and leadership and the need for continuing consultation and training.105 The presence of management and leadership decisions and strategies operating as barriers and facilitating factors throughout the organisational context—both directly and indirectly—aligns with findings that leadership at all levels (eg, executive director, middle manager, clinical supervisor) is associated with innovation,106 implementation of evidence-based practice (EBP),107 and with improving the organisational context for EBP implementation.108 The need for support from senior managers (and commissioners) and for a whole team approach is also reflected in the suggestions on how to implement family work in mental health services provided by professionals and carers with experience of participating in a Family Behavioural Therapy Programme.109
The fundamental role of the organisational context is emphasised in the literature with both culture (the normative beliefs and shared expectations of the organisation) and organisational climate (the psychological impact of the work environment on the professional) strongly moderating the uptake of EBP.110 The practice to be implemented must match the mission, values, tasks and duties of the organisation and individuals within that organisation.111 The absence of a strong organisational culture favouring family work may be influenced by traditional paradigms based on the predominance of biological models of mental illness, which tend to minimise the focus on the individual's social context.50 Also, the characterisations of families as dysfunctional and sometimes even as ‘the cause of psychiatric illness,’ despite being widely rejected,112 may have contributed to a loss of trust in services and strained relationships between professionals and families.113 This may explain the importance and the effort required in building alliances, which emerged in our findings. Clinicians may uphold the patient–professional alliance by addressing concerns regarding privacy and by being mindful that patients do not perceive a loss of power due to having family involvement in their care.
Future directions for research
So far the findings largely reflect what can go wrong rather than provide evidence of successful implementation. For example, sustainability has not been addressed in the review as this stage has hardly been reached. More research will be needed to see which organisational steps can actually change the culture in a service so that family involvement happens, not only in a research study or with particular patients, but with all families, every day and over longer periods of time.
Future studies should attempt to better capture wider views, particularly in-depth understanding of patients’ and families’ views. This may also enable insight into the potentially varied experiences of minority groups. These views may be best obtained outside of group interviews, in which a power imbalance may be present. There would also be value in exploring the views of professionals who have not already demonstrated commitment to family work.
Despite a ‘whole team approach’ seeming to be the way forward for a widespread implementation of family work, there is a need to obtain insight into the organisational challenges that may be related to this and to develop clear practical guidelines for the reorganisation of clinical teams.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online supplement
- Data supplement 3 - Online supplement
Footnotes
-
Contributors DG, EE and SP contributed to the conception and design of the study. EE designed and conducted the search, DG and EE selected the studies. AD and EE extracted data and carried out the thematic synthesis. EE wrote the manuscript, AD and DG reviewed and edited the manuscript and SP provided critical review of the manuscript. All authors contributed to and approved the final submitted version.
-
Funding This paper presents independent research and was partially funded by the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care (NIHR CLAHRC) North Thames at Bart's Health NHS Trust.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.
-
↵i Attempts were made where possible to focus on patients with psychosis, however many studies used opportunity sampling of mixed ‘severe mental illness’ groups, which were included in order to be as inclusive as possible.