Article Text

Abstract
Objectives To explore the relationship between childhood socioeconomic position (SEP) and filling of medicine prescriptions for prevention of cardiovascular diseases (CVDs), with young adult intelligence (IQ) as a potential mediator.
Design Birth cohort study with logistic and Cox-proportional hazard regression analyses of associations between childhood SEP, retrieved from birth certificates, and prevalence, initiation of and refill persistency for CVD preventive medicine.
Setting Denmark.
Participants 8736 Danish men born in 1953, who had no CVD at the start of follow-up in 1995, were followed in the Danish National Prescription Register for initiation of and refill persistency for antihypertensives and statins, until the end of 2007 (age 54 years).
Results Low childhood SEP at age 18 was not associated with prescription fillings of antihypertensives, but was weakly associated with initiation of statins (HR = 1.19 (95% CI 1.00 to1.42)). This estimate was attenuated when IQ was entered into the model (HR=1.10 (95% CI 0.91 to 1.23)). Low childhood SEP was also associated with decreased refill persistency for statins (HR=2.23 (95% CI 1.13 to 4.40)). Thus, the HR for SEP only changed slightly (HR=2.24 (95% CI 1.11 to 4.52)) when IQ was entered into the model, but entering other covariates (education and body mass index in young adulthood and income in midlife) into the model attenuated the HR to 2.04 (95% CI 1.00 to 4.16).
Conclusions Low childhood SEP was related to more frequent initiation of and poorer refill persistency for statins. IQ in young adulthood explained most of the association between childhood SEP and initiation of statins, but had no impact on refill persistency.
- Epidemiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
The study includes all boys born in greater Copenhagen in 1953, and all data on socioeconomic position in childhood, IQ and covariates were collected prospectively from birth to midlife.
-
The register-based information on fillings of prescription medications provides complete coverage of all medicine prescription fillings at Danish pharmacies from 1 January 1995, and the use of register data provides almost complete follow-up on participants and eliminates recall bias.
-
The register data do not contain information on prescribed doses, on actual intake of medicine or on indications for prescription of cardiovascular disease preventive medicine.
-
The study is limited to middle-aged men, and the results may not be transferable to women and older individuals.
Introduction
A number of cohort studies have suggested that socioeconomic disadvantage during childhood contributes to increased morbidity and mortality from various diseases, especially cardiovascular disease (CVD).1 ,2 Low intelligence (IQ) measured early in life has also consistently been associated with lower childhood socioeconomic position (SEP) and mortality from CVD.3–5 Childhood environment may be an important factor leading to social health differences as childhood includes developmentally sensitive periods for the acquisition of cognitive, psychological and social skills which may influence an individual's long-term health. There are several plausible explanations for associations between SEP in childhood, IQ and CVD6; the possible pathways include: the ‘disease prevention hypothesis’, which suggests that high SEP and IQ are associated with favourable lifestyle leading to lower risk of CVD, while the ‘disease management hypothesis’ suggests that high SEP individuals are also more apt at managing existing CVD and associated risk factors such as hypertension and diabetes. Such risk factors are treated with lifestyle changes and medication when needed. Several studies have shown that childhood SEP and IQ levels are associated with the acquisition of lifestyles associated with CVD in later life, such as physical activity, appropriate diet and smoking.7 ,8 However, most studies of lifestyle factors have found that they only explain part of the associations between childhood SEP, IQ and CVD.3 ,4 ,9 ,10 It is also evident that managing treatment is a cognitive task for individuals experiencing illness such as CVD. Individuals with low education, which is correlated with low childhood SEP and IQ, are less likely to understand instructions for medication use or to recognise that their health requires attention.11 Thus, drug prescriptions have been found to be socially patterned12–14 and studies have shown similar social gradients in disease incidence and use of indicated medications, that is, those with higher ‘need’ use more medications.15 ,16 Although fillings of drug prescriptions to a large extent reflect health status, other factors such as access to healthcare and health-seeking behaviour may also influence drug prescription fillings. However, there seems to be no previous studies that have investigated the independent influences of SEP and IQ early in life on fillings of prescription medicine targeting the prevention of CVD in midlife.
The main aim of this study was to explore the relationship between childhood SEP and filling of drug prescriptions for prevention of CVD and to explore the influence of IQ in young adulthood on the expected association between childhood SEP and initiation and refill persistency for antihypertensives and statins in middle age. Furthermore, educational status, body mass index (BMI) in early adulthood and income in midlife were included as potential mediators. IQ has been related to education and BMI, and these factors were included as mediators of any impact of SEP or BMI on prescription fillings. Income was also included since it is considered as a possible mediator (figure 1).

Hypothetical relationship between childhood socioecomic position (SEP), young adulthood intelligence (IQ), educational attainment, body mass index (BMI), income and prescription fillings of medicine for the prevention of cardiovascular disease (CVD). Solid arrows represent the associations from previous studies; broken (dashed) arrows represent the associations of primary interest in this study.
Material and methods
Study population
The study was based on the Metropolit cohort, consisting of 11 532 men who were born in 1953 in the Copenhagen Metropolitan area, and who were living in Denmark in 1968. The cohort is described in detail elsewhere.17 Data from birth certificates, including information on father's occupational status at the time of delivery, were manually collected in 1965 for all members of the cohort. For decades, nearly all Danish men have had to appear before the draft board when they are about 18 years of age. Here they complete an IQ test and undergo a health examination by a medical doctor. In 2004, draft board data were collected from the Danish Military Archives for 11 108 (97%) members of the Metropolit cohort who were alive and living in Denmark in 1971.
The civil registration number of the individual cohort member allowed linkage between historical data and register data. Since 1980, information on selected social and health characteristics has been obtained each year for all cohort members by linkage to the databases of Statistics Denmark and to the Danish National Patient Register. The latter register contains information at individual level on all patients discharged from non-psychiatric hospitals since 1979; the records include admission and discharge date, discharge diagnoses according to the International Classification of Diseases (ICD; 8th revision until 1993 and 10th revision thereafter). The cohort has also been linked to the Danish National Prescription Registry, which contains information on prescription medication purchased by outpatients at Danish pharmacies from 1995 onwards. Each prescription record contains information about the date and anatomical therapeutic classification (ATC) codes.14 ,18
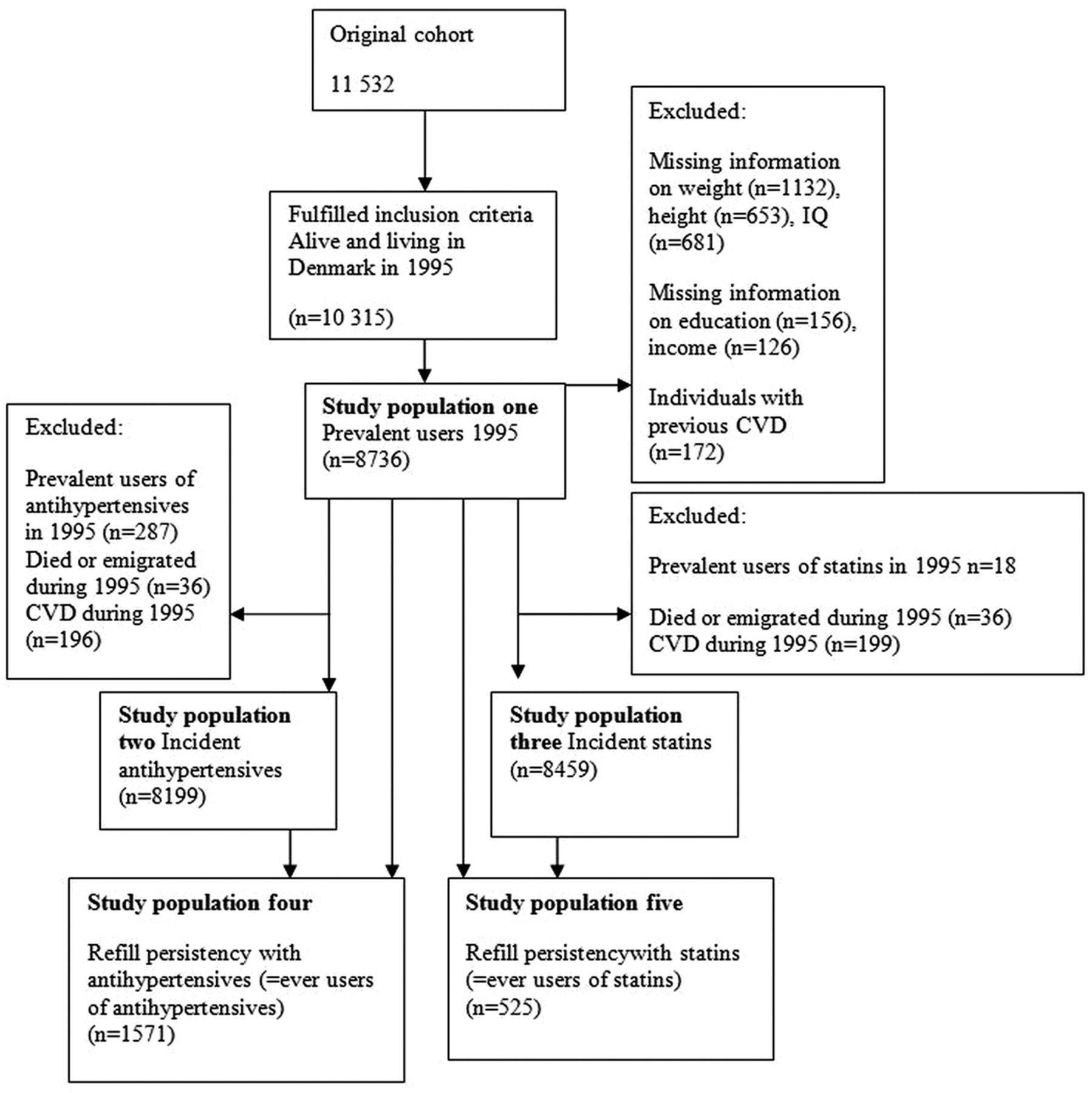
To identify individuals without previous or present CVD, we used historic register data on inpatient diagnoses (defined by ICD8 and ICD10 codes: 390–450 and I00-I52, I60-I99) and in addition dispensed prescribed medication as markers for a range of CVD. These included register-markers for coronary heart disease (CHD) with or without myocardial infarction, stroke, peripheral arterial disease in the lower limbs, along with a range of potential atherosclerotic conditions (eg, arrhythmia and nephropathy) as described in a recent publication with detailed definitions of the applied register-markers.19 By excluding individuals with these conditions, we assume that use of antihypertensive medication is for the treatment of hypertension without existing heart disease or organ damage. Furthermore, the study population was limited to 8736 cohort members with complete information on all covariates (figure 2).
{kind=link}
{kind=link}
Dataflow of eligible participants form a cohort of men born in 1953 (the Danish Metropolit cohort).
To study initiation of and refill persistency for CVD preventive medicine, we defined five subsamples.
Subpopulations and definition of outcomes (CVD preventive medication)
In this study, CVD preventive medicine included antihypertensives (ATC group: C02, C07, C08 and C09) and statins (ATC group: C10AA) dispensed by individuals with no prior CVD.
-
Prevalence of drug prescription fillings in 1995 was defined as the number of cohort members who filled prescription medicine targeting CVD at least once in 1995 (ie, period prevalence). Eligible for this population were individuals alive and living in Denmark on 1 January 1995 without missing data on height, weight or IQ from the draft board record and individuals who had no missing information on education, income or CVD disease before 1 January 1995 (see study population 1 in figure 2).
-
Initiation of antihypertensives in the period 1996–2007 was defined as first filling of antihypertensive medicine during the period 1 January 1996 to 31 December 2007. Eligible for this population were cohort members from study population 1 alive and living in Denmark on 1 January 1996 who did not die, emigrate or had CVD or prescription filling for antihypertensives in 1995 (see study population 2 in figure 2).
-
Initiation of statins in the period 1996–2007 was defined as first filling of statins during the period 1 January 1996 to 31 December 2007. Eligible for study population 3 were cohort members from the study population who were alive and living in Denmark on 1 January 1996 who did not die, emigrate or had CVD or prescription filling for statins during 1995 (see study population 3 in figure 2).
-
Low refill persistency with antihypertensives was those with an interval between two antihypertensive prescription fillings that exceeded 365 days between 1 January 1995 and 31 December 2007. The study population was those ever treated with antihypertensives between 1 January 1995 and 31 December 2007, that is, cohort members from study populations 1 and 2 who had at least one prescription filling of antihypertensive medicine between 1995 and 2007 (see study population 4 in figure 2).
-
Low refill persistency with statins was those with an interval between two statin fillings that exceeded 365 days between 1 January 1995 and 31 December 2007. The study population was those ever treated with statins, that is, cohort members from study populations 1 and 3 who had at least one prescription filling of statins between 1995 and 2007 (see study population 5 in figure 2).
In Denmark, hospitalised individuals are provided with medication from the hospital pharmacy during their hospitalisation, and consequently days spent in hospital were subtracted in the calculation of days between prescriptions. A shift in specific brand or type of medication within the two groups of CVD preventive medicine (ie, within different brands/types of antihypertensive or/and statins) was not considered a discontinuation of medication. Previous studies on persistency with CVD medication showed that longer spells between refills were related to lower probability of later reinitiation of treatment.20
Exposure
Father's occupation at participant's birth in 1953 was recorded in 23 categories and recoded into two occupational social class categories: ‘high’ (self-employed; salaried employed/civil servants) and ‘low’ (skilled workers; unskilled workers and not employed/unknown).
The potential mediator
In this study, IQ was measured by Boerge Prien's Proeve (BPP) which comprises four subtests: letter matrices, verbal analogies, number series and geometric figures.21 The score is the total number of correct answers with a range of 0–78, and the BPP test has been shown to correlate substantially with the Wechsler Adult Intelligence Scale.21 The test is completed at the draft board before which most of the cohort members (90%) appeared in 1972–1973 when they were around 18 years. In this study, the test scores were divided in tertiles.
Covariates
In line with previous studies on SEP and IQ in a life-course perspective, we wanted to study the associations after controlling for available, potentially confounding or mediating factors measured in young adulthood. From the social registers from 1980, we used educational attainment coded into ‘high’ (at least secondary education) and ‘low’ (primary education only). Income details were retrieved from the social registers from 1994 and was categorised into ‘high’ and ‘low’ (above or below the median income in 1994). Height and weight data were retrieved from the draft board registry, and BMI was calculated as weight in kg/height in m2 and categorised as ‘underweight’ (<18.5), ‘normal weight’ (18.5–25) and ‘overweight’ (>25).22
Statistical methods
Medication prevalence, initiation and refill persistency were analysed separately for antihypertensives and statins. Associations between childhood SEP and IQ and prevalence of drug use in 1995 were analysed using logistic regression analyses, where the event was a prescription filling of CVD preventive medicine. Associations of childhood SEP and IQ and initiation of antihypertensive or statin treatment between 1996 and 2007 were analysed using Cox-proportional hazard models, where the event was first prescription filling of CVD preventive medicine after 1 January 1996. Follow-up was from 1 January 1996 to the event or censoring (date of first register marker of CVD, death, emigration or end of follow-up at 31 December 2007 when cohort members were 54 years of age). Discontinuation of treatment was analysed using Cox-proportional hazard models with follow-up starting at the date of first prescription and ending at discontinuation of treatment or censoring (date of first register marker of CVD, death, emigration or end of follow-up (31 December 2007)). The variance inflation test was used to investigate potential problems with multicollinearity in multivariate models.23 In multivariate analyses BMI, educational attainment and income were added stepwise.
Results
The distribution of childhood SEP, IQ and covariates in each of the five study populations are shown in table 1. During 1995, the prevalence of prescription fillings of antihypertensives was 3.3% (n=287), 1284 (15.7%) patients initiated medical treatment with antihypertensives between 1 January 1996 and 31 December 2007 and 275 (17.5%) of the 1571 (ever) treated patients had a break in treatment with antihypertensives. During 1995, 18 (0.2%) men filled a prescription of statins, 507 (6%) patients initiated treatment of statins between 1 January 1996 and 31 December 2007, and 47 (9%) of the 525 men ever treated had a break in treatment with statins. The prevalence of fillings of statins in 1995 was too small to allow further analysis.
The distribution of childhood SEP, IQ, education and BMI in young adulthood and income in relation to prescription fillings with antihypertensive and statins in middle-aged men born in 1953
Table 2 provides the unadjusted OR or HR and 95% CIs for the associations between childhood SEP and prescription fillings of antihypertensives and in the second model the estimates adjusted for IQ and in the third model the estimates adjusted for all covariates. Childhood SEP was not significantly associated with prescription fillings of antihypertensive medication in the unadjusted model. Entering IQ attenuated the OR for low childhood SEP from 24 (95% CI 0.99 to 1.10) to OR=1.12 (95% CI 0.87 to 1.43). Initiation of antihypertensives between 1995 and 2007 and refill persistency of treatment with antihypertensive medications were not related to childhood SEP or IQ.
The unadjusted, IQ and mutually adjusted associations of childhood SEP, IQ, education and BMI in young adulthood and income with prevalence, initiation of and refill persistency with antihypertensives in men born in 1953 (OR and HR and 95% CI)
Table 3 shows HR and 95% CI for the associations between childhood SEP and statin prescription fillings, in an unadjusted model, a model adjusted for IQ and one also adjusted for other covariates. Low childhood SEP was associated with initiation of statins (HR=1.19 (95% CI 1.00 to 1.42)) in the unadjusted model. The HR was attenuated when IQ was entered into the model, and the association with childhood SEP became insignificant (HR=1.10 (95% CI 0.91 to 1.23)). Low childhood SEP was clearly associated with decreased likelihood of persistency of statin treatment (HR 2.23 (95%CI 1.13 to 4.40)). IQ was not associated with refill persistency for statins, and the HR for SEP only changed slightly (2.24 (95% CI 1.11 to 4.52)) when IQ was entered into the model, while entering the other covariates into the model attenuated the HR to 2.04 (95% CI 1.00 to 4.16).
The unadjusted, IQ and mutually adjusted associations of childhood SEP, IQ, education and BMI in young adulthood and income with initiation of and refill persistency with statins in men born in 1953 (HR and 95% CI)
Discussion
This study on the use of CVD preventive medicine in middle-aged Danish men indicated that those with low SEP in childhood tended to have a higher probability of initiation of statins and poorer persistency of treatment with statins. IQ might be a mediating factor between childhood SEP and initiation of statins, while it had no impact on the association of low childhood SEP with low refill persistency for statins. Our study is the first to analyse the association between SEP in childhood and initiation of and persistency of treatment with CVD preventive medicine with IQ measured in young adulthood as a potential mediator. However, a number of studies have investigated the influence of childhood SEP on CVD morbidity and mortality. Most of these studies have found an association between childhood SEP and CVD.1 ,9 ,11 ,24 Furthermore, in a previous study of the Metropolit cohort, men with low childhood SEP had an increased risk of CHD after adjustment for adult SEP.25 This and the other studies point in the direction of a higher ‘need’ of preventive medicine among the socially disadvantaged. In the present study, the associations between childhood SEP and initiation of hypertensives were close to one, which may indicate that the preventive medicine is refilled less than the underlying need would suggest. Previous studies have found that a higher IQ is associated with a lower risk of CHD morbidity and mortality3 ,4 and subclinical atherosclerosis.26 We found that those with higher IQ tended to have a lower initiation of statins. These findings seem to be in line with the smaller ‘need’ found in most other studies, and a priori we had assumed that initiation of CVD preventive medicine would be a proxy for increased risk of development of CVD and thus reflect the ‘need’ of medication. This assumption was partly supported by our findings. The higher initiation of CVD preventive medicine in those with higher BMI also supports that refills of prescriptions for CVD medications reflect the ‘need’ of treatment.
However, other factors than ‘need’ may be involved in the process leading to refill of prescribed medications. It is likely that attitudes towards medications developed in childhood and IQ are related to seeking medical advice, communication with health professionals and the actual purchase of prescribed medication. It has been demonstrated that individuals with low educational attainment, which is strongly correlated with IQ scores, are less likely to understand instructions for medicine use and to know the appropriate actions to take in case of side effects.11
These factors may also be associated with continuing treatment with CVD preventive medicine. Those with higher SEP in childhood and those with higher IQ may have more information and thus be more likely to take medicine as prescribed, which could explain the higher rate of continued treatment in these groups. A few studies have found that IQ in adulthood or old age was associated with non-adherence to medications. However, these studies measured IQ after onset of disease which means that IQ may have declined because of disease.27 ,28 We found that higher IQ was associated with refill persistency for antihypertensive medications but not with persistency with statins. Other studies have linked adherence to CVD preventive medicine to factors such as low income, low education and low health literacy,14 ,29 ,30 all of which have been related to poor SEP in childhood and lower IQ.
We found differences in the patterns of initiation and refill persistency of treatment with antihypertensives and statins. In Denmark, which is known as a country with free access to health services, individuals have to pay for prescribed medicine, and in the late 1990s, statins were rather expensive medication. Lower income is associated with lower refill persistency for statins following a myocardial infarction.14 ,28 It is possible that low adult income also contributes to the higher rate of discontinuation in treatment of statins among those with low childhood SEP. Furthermore, the benefits of statin use have been questioned, and some potential users of statins may have decided not to initiate treatment or to discontinue treatment due to this debate. Moreover, some may prefer to change diet and exercise patterns rather than use CVD preventive medicine, and this strategy may be more common and perhaps also more successful in individuals with more intellectual and financial resources. However, other studies have found that those who were more compliant with statins are also more health conscious,31 which suggests that CVD preventive medicine and life style changes may be used as complementary strategies.
Study strength and limitations
The study includes all boys born in greater Copenhagen in 1953, which corresponds to about one-third of all boys born in Denmark that year. Data on SEP in childhood, IQ and covariates were collected prospectively from birth to midlife. The advantage of register-based information on prescription fillings of medications is the complete coverage of all prescription fillings at Danish pharmacies from 1 January 1995. Information on CHD disease was also retrieved from the Danish National Prescription Register and the Danish National Patient register, which covers all hospital admissions from 1979 and onwards. The use of register data provides almost complete follow-up on participants and eliminates recall bias. However, register data do not contain information on prescribed doses, and an inherent limitation with register data is the lack of information on the actual intake of medicine. The focus of this study was use of antihypertensives as prevention of CVD. Yet, some of these antihypertensives are also prescribed for other indications, for example, β-blocking agents (C07) as migraine preventing medication. This study does not have information on the indication for prescription of CVD preventive medicine or on risk factors such as smoking. BMI was measured at age 18–20 years where few cohort members were overweight. The proportion of overweight and obese individuals was far higher at age 50.32 Nevertheless, BMI measured in early adulthood predicted initiation of preventive medications. This study was limited to middle-aged men, and the results may not be transferable to women and older individuals, who in one study have been found to have better compliance with ACE inhibitors, β-blockers and statins compared with men and younger individuals.20
Conclusion
We found that low childhood SEP predicted more frequent initiation of and poorer refill persistency for statins. IQ in young adulthood explained most of the association between childhood SEP and initiation of statins, but had no impact on refill persistency for statins. Childhood SEP and IQ only had limited impact on fillings of antihypertensive.
Acknowledgments
The authors would like to thank K Svalastoga, E Høgh, P Wolf, T Rishøj, G Strande-Sørensen, E Manniche, B Holten, I AWeibull and A Ortmann who established the data between 1965 and 1983.
References
Footnotes
-
Contributors All authors have contributed to the study. MO formulated the original study idea and provided funding. MK further developed the study idea and design of the study with all coauthors, and carried out data analyses and took responsibility of writing the first draft of the article. All authors participated in interpretation and discussion of the findings.
-
Funding This work was supported by a grant from Center for Healthy Aging sponsored by the Nordea Foundation.
-
Competing interests None.
-
Ethics approval Danish Data Inspection.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.