Article Text

Abstract
Objective To explore the views of parents and clinicians regarding the optimal content, format and delivery of safety netting information for acute childhood illness.
Design Qualitative study including semistructured focus groups and interviews.
Setting First contact care settings, community centres, children's centres and nurseries in the Midlands, UK.
Participants 27 parents from a travelling community, Asian British community and white British community. Sixteen clinicians including 10 doctors and 6 nurses from a general practice surgery, an out-of-hours service and two emergency departments (paediatric and combined adult and paediatric).
Results Participants described a need for safety netting to contain information on signs and symptoms of serious and common illnesses, illness management and where and when to seek help. Resources should be basic, simple to use and contain simple symbols. A key criterion was professional endorsement of resources. Internet-based information was desired which is reliable, consistent and up-to-date. Participants described a need for different types of information: that which could be delivered during consultations, as well as more general information for parents to access before consulting a healthcare professional. Face-to-face education, written materials and digital media were suggested delivery mechanisms. Audiovisual material was preferred by families with low literacy. Participants commonly suggested internet-based and phone-based resources, but the travelling community was less comfortable with these approaches.
Conclusions A multifaceted and tailored approach to safety netting is needed so that effective resources are available for parents with varying information needs, literacy levels and ability to use information technology. We have identified key aspects of content, quality criteria, format and delivery mechanisms for safety netting information from the perspectives of clinicians and parents. Resources should be coproduced with parents and clinicians to ensure that they are valued and utilised by both groups.
- primary health care
- safety netting
- qualitative research
- acute disease
- parents
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
Parents and clinicians participated, and the findings could form the basis of truly coproduced resources.
-
We included diverse groups of parents with different information needs and abilities, and clinicians from a range of first contact care settings, to ensure that the views of different groups were included; however, the extent to which the findings are generalisable to other groups or populations is not known.
-
Data were collected and analysed by a team of researchers including clinical and non-clinical, some parents and some not, enabling a deeper understanding.
Introduction
Acute childhood illness is a major contributor to children's presentation to primary care, and to child mortality. Child and young person mortality has fallen in Europe, but child death rates from treatable causes including asthma, pneumonia and meningitis are higher in the UK than elsewhere in Europe, highlighting a need to better manage acutely sick children.1 ,2 The vast majority of children have minor, self-limiting illnesses requiring little or no medical intervention, and it is increasingly difficult for clinicians to identify the very few children with serious illnesses, which often have non-specific presentations and clinical features mimicking those of common, non-serious illness.3 Despite the prevalence of life-threatening acute childhood illness being at an all-time low, there has been an increase in children's emergency hospital admissions, many of which are for minor illnesses which could have been managed in the community.4 ,5 Safety netting information given to parents during consultations advises them about when and where to seek further help.6 As well as aiming to prevent misdiagnoses and avoidable child mortality, there is evidence that safety netting can reduce reattendances in febrile children.7 ,8
Safety netting was first described by Neighbour9 over 20 years ago, who proposed it to be a core component of general practice. More recently, safety netting has been recommended in the management of acutely sick children by the National Institute for Health and Care Excellence (NICE),10 Scottish Intercollegiate Guidelines Network (SIGN),11 other national groups,2 ,12 general practitioners6 ,13 and researchers,14 and has been introduced as a NICE quality standard.15 Despite these recommendations, there are no set guidelines regarding the optimal content, format and delivery of safety netting.
Anxiety and uncertainty surround parents’ decisions about when to consult (and reconsult) healthcare professionals during acute childhood illness at home.16 ,17 Safety netting could potentially help to reduce these, and provide the more explicit and consistent advice that parents seek.7 However, the most effective components and ways of delivering safety netting are yet to be identified,18 ,19 and there is evidence that current safety netting advice may be inadequate. For example, a study of 220 feverish children making 570 contacts with urgent care services found that 19% of parents did not recall being given any safety netting advice, and documentation of safety netting advice regarding what to look for was absent in nearly half (43%) of patients’ records.8
As part of the Acutely Sick Kids—Safety Netting Interventions for Families (ASK SNIFF) project, this study aimed to explore the opinions of parents and first contact clinicians regarding the optimal content, quality criteria, format and delivery of safety netting information. This is vital for the development of effective safety netting materials to increase parental confidence, understanding and satisfaction, decrease uncertainty and anxiety, as well as increase timely and appropriate presentation to primary care. Including and combining the opinions of clinicians and parents mirrors a key principle of the Children and Young People's Health Outcome's Forum, that families must have a voice and be engaged in the development of services.2
Methods
We used a qualitative, exploratory approach due to the lack of prior knowledge on the topic. Maximum variation sampling was used to recruit parents from a wide range of communities, and doctors and nurses working in different first contact care settings in the Midlands, UK. Any parents with at least one child under the age of 5 years and any clinicians treating children under 5 years of age at first contact, who were able to speak English, were eligible to participate. We conducted focus groups and/or interviews in each parent community and at each first contact care workplace.
Recruitment was coordinated by email or in person using the local Primary Care Research Network, the Comprehensive Local Research Network for clinicians, community facilitators, health ambassadors and day nursery/children's centre managers for parents. All participants gave written informed consent. The study was approved by the East Midlands—Nottingham 2 NHS Research Ethics Committee (REC reference 12/EM/0076) —and the appropriate research and development offices of each local Trust. Two experienced female researchers (SN, a children's nurse lecturer and HS, a social scientist) facilitated focus groups and interviews between May and December 2012, which were semistructured and lasted around an hour. Participants were asked a number of questions about provision of safety netting information (see box 1), and the facilitators used prompts to elicit further details. One facilitator took notes and gave a verbal summary at the end, asking the participants to correct misinterpretations and give further comments. Focus groups and interviews were audio recorded, transcribed verbatim and anonymised.
Box 1 Topic guide for focus groups and interviews
Parents
What information do you want/need to find when your child becomes sick?
Where would you like to find/be given this information?
In what ways, if any, would you like to see access to information improved?
In what ways, if any, do you think the information provided needs to be improved?
Clinicians
What safety netting information do you think parents of sick young children should be given?
How do you think they should be given this information?
In what ways, if any, do you feel the safety netting information available needs to be improved?
In what ways, if any, would you like to see access to information improved?
Data were analysed using the grounded theory method of constant comparison. Three main themes were predetermined by the research question and topic guide (content, quality criteria and format/delivery of safety netting). Codes and subthemes within each of these themes were developed according to the content of focus groups/interviews. Separate coding schemes were devised for parent and clinician data, with many of the same codes occurring in the parent and clinician coding schemes. Throughout the process of data collection and analysis, codes were edited, combined and new ones added, and codes were grouped together as subthemes were developed within each theme. The coding schemes were developed together by CJ (a non-clinical researcher) and SN (a children's nurse lecturer), who allocated text to codes accordingly. CJ coded the clinician data and SN coded the parent data, and both researchers cross-checked the codings. Both researchers were familiar with the content of all focus groups/interviews and both coding schemes. Emerging subthemes and comparisons between parent and clinician data were discussed and developed among the wider research team. The constant comparative method enabled us to identify similarities and differences within the data coded to the same and different subthemes from parents and clinicians.
Results
Participants
Participants included 27 parents and 16 clinicians. Parents were from a travelling community (recruited via a community facilitator), Asian British community (recruited at a local community centre and a children's centre) and white British community (recruited from a children's centre and a private nursery; see table 1). Clinicians were included from a general practice surgery, a District General Hospital (DGH) emergency department (ED) (treating adults and children), a paediatric ED and an out-of-hours service (OOHS; see table 2).
Characteristics of participating parents
Characteristics of participating clinicians
Below we present the three main themes—content, quality criteria and format/delivery of safety netting—and the subthemes within them. Tables 3⇓–5 display each theme, respectively, and the subthemes within them, with quotes to illustrate aspects of our interpretation of the data within each of the subthemes.
Subthemes and illustrative quotes within the Safety Netting Content theme
Subthemes and illustrative quotes within the Safety Netting Quality Criteria theme
Subthemes and illustrative quotes within the Format and Delivery of Safety Netting theme
Safety netting content
There was consensus among the clinicians working in the different settings that paediatric illness is broad, and safety netting advice should focus on signs and symptoms of the most serious and most common childhood illnesses: “It's the nasty ones that you want to catch and the very common things that people will have never seen before but are OK” (DGH ED doctor). Some clinicians thought that in addition to specific advice given during consultations, there is a need for generic advice or education: “perhaps there could be… more kind of generic advice about unwell children” (OOHS GP); “instant access [to information] doesn't really help because you need to build up your knowledge long before the child becomes ill” (DGH ED doctor). This emphasises the potential need for two different resources: a diagnosis or illness-related safety netting resource for use during/postconsultation, and a more general educational resource for use preconsultation.
Clinicians described the importance of signposting parents to different services according to illness severity and providing information on illness management. Primary care staff focused on the need to educate parents about when to care for their child at home or visit the pharmacy, whereas ED staff focused more on the need to communicate what signs and symptoms indicate that parents should attend an ED immediately.
Parents’ need for information matched that of clinicians, namely what symptoms are associated with the most common and most serious illnesses (particularly meningitis), and when/where to access help. After receiving a diagnosis, information is wanted on illness causation, management and trajectory: “Where I ask every question under the sun. What is it, why did they get that, how many times will they get it again?” (travelling community mother).
Safety netting quality criteria
Clinicians and parents similarly stated that safety netting resources should be basic, simple to use, with simple messages. Simple symbols and colour indicators were suggested for presenting safety netting information visually, which would be particularly useful for people who are unable to easily understand written information. Suggestions included ticks and crosses, sad and happy faces, traffic lights, red and green: “a picture with a green smiley face, a meningococcal septicaemia rash with a big upset blue light on top of it type face or something like that” (DGH ED doctor). The parents and clinicians felt that information should be provided in simple language, as well as multiple languages; and that it should be symptoms-based because parents would not always know their child's diagnosis when searching for information.
Importantly, it was commented that written information, including internet-based resources, should be easy and quick to access. However, one clinician raised a caveat: “you've got to be very careful with the information that you are putting out there, because you don't want to drive the paranoia more that there is” (paediatric ED doctor).
A key quality criterion identified by parents and clinicians was professional endorsement: “I think if it was NHS backed you'd kind of have a bit more trust” (white British mother). Publicity was also highlighted: “it needs to be publicised that patients know to access that site, whereas what's happening now is that they're accessing Google and getting a whole lot of symptoms which, y'know, lots of them are not necessarily useful and, erm, heightens the anxiety” (GP surgery doctor). These criteria were described particularly in relation to internet-based safety netting resources: currently, searching the internet generates an ‘overload’ of information, some of which are not useful, which creates uncertainty and anxiety among parents. Access to reliable, consistent, up-to-date internet-based information was commonly requested: “the problem is I think the information's there, it's not all in one place, it's all over different websites and if the Department of Health was able to somehow streamline the advice nationally and set up a process of okaying national advice for parents… I think that would be the way to do it” (paediatric ED doctor).
It was suggested that parents need resources which are portable, particularly when caring for a distressed child. Different methods were suggested for achieving this, including providing portable hard copy: “You've got them clung to you cause they're unwell, you're not going to sit at a computer” (GP surgery nurse); “I think they sort of produce sort of credit card sized things they can give out… so perhaps more of those sorts of resources” (OOHS GP). Alternatively, phone-based internet access could provide a quick and easy access to information: “I would do it on my phone, oh yeah, yeah, yeah, very much so. And that I actually find easier than picking up the phone because if you've got a crying child, trying to pick up the phone and talk to somebody is actually a lot more difficult than having a quick look on the internet to see…” (white British mother).
Format and delivery of safety netting
As described above, the participants described a need for different types of safety netting resources including those delivered during consultations and those accessed prior to consultation. They also acknowledged that information should be provided in multiple formats: “It can be on different forms of media, Internet. Obviously, Internet may not be accessible to many people and if it is accessible, they may not be able to go to the right information, right section so having it in different formats will be quite helpful” (Asian British father).
Consultation-based safety netting
Clinicians described how verbal and written safety netting information could be delivered during consultations, and suggested demonstration of physical signs including tracheal tug, intercostal recession and slow capillary refill time. Provision of written materials during consultations could be useful for parents: “Well half the time when you're taking your child to the doctors they're not very well, are they, so they're clingy, you've had to probably strip them off… so they're crying and they're trying to tell you all this information and getting them back dressed again really quickly… There is pressure to get out quickly, I think, so I think you do forget what the doctor has said.” (white British mother).
Another type of safety netting was referring children to other services such as community children's nurses. Some clinicians thought that written safety netting materials should be tailored to the local area accordingly: “a bit more specific to the area as well, that would be good so it was, you know it takes into account sort of local pathways, what's available locally including things like the community children's nurses” (OOHS GP). Conversely, one parent highlighted the need for standardised advice: “It should be across nationally and so on, so that everyone is getting the same message” (Asian British mother).
Preconsultation education
Safety netting resources for use prior to consultation included general preparatory educational information to be accessed prior to illness occurring and more specific information for parents to access during acute childhood illness, before they consult a healthcare professional.
Educational methods suggested by the clinicians included education by health visitors, and peer education so that parents can learn from the experiences of others—a caveat being that the information is correct: “actually learning by somebody else's experience what happened and what were you told and it's getting that because peer education, if it's correct, ‘cause that's another reason why we get to see people, ‘cause another relative has sent them in and said you must be seen, because advice has changed…” (GP surgery nurse). Other suggestions were delivery by school/nursery teachers and social workers. Parents had similar suggestions to clinicians, namely education on childhood illnesses by health visitors and schools/nurseries as well as novel suggestions including libraries, community centres and GP surgeries (in waiting rooms as well as during consultations). They also suggested community-based delivery systems including community champions, community educational programmes (such as short courses in community centres) and community snowballing (whereby healthcare professionals provide initial educational sessions, then peers provide these sessions afterwards).
Written materials were suggested for educating parents prior to their child becoming ill. The parents and clinicians mentioned posters, and suggested the information pack for new parents as a way to deliver written information (although parents did comment that they did not use the information provided in this pack beyond the neonatal period). Other parental suggestions for written materials included booklets, leaflets, flash cards and small quizzes. The parents and GPs had a limited knowledge of the information on childhood illness currently contained in the personal child health record (‘red book’), and felt that it was not well used by parents or GPs. Building on the information contained in books, or introducing new books, may not be an effective mechanism to educate parents about childhood illness: “I think I possibly looked at it when I was a new mum with you know, so much enthusiasm, and then about a week in I was like… I'm far too tired to do this, there's no way I'm reading through that book” (white British mother).
Parents suggested a wide range of digital media which could be used to deliver information, including internet, phone-based media, DVD, television programmes and rolling displays on waiting room screens. Many parents recalled media campaigns for stroke, and the glass test for non-blanching rash in meningitis. These campaigns appear to have reached all of the social groups in the sample. Parents felt that media campaigns could be successful for acute childhood illness. The GP surgery focus group acknowledged the success of media campaigns and suggested this could work for educating parents on child illness, although it was acknowledged that media campaigns could create anxiety.
Internet-based resources
Internet-based resources such as a centralised website were commonly mentioned by parents and clinicians alike. One thing parents would like is a well-signposted website with NHS endorsement, which is easy to search and appropriate for mobile phones. Parents were in favour of doctors giving out information about a reliable site at the end of consultations. Clinicians indicated that they were happy to perform this; but it would need to be simple to use: “you wouldn't want to, yeah, be getting into huge conversations about how you do it… how you access it, so yeah, it would need to be sufficiently simple and accessible” (OOHS GP).
Similarly to parents, clinicians in all settings suggested that a phone-based application could be successful in helping parents of sick children assess whether/where to seek help: “World and times are changing, everything is about internet, everything is about apps and I think if you've got something well written and accessible, on the internet with maybe an iPhone app, an android app, that people can download y'know, some sick kids guide or something like that with a bit of a symptom checker and robust, this is what paediatricians, this is what GPs, this is what emergency physicians would advise you to do, then I think people will take that seriously and I suspect it would cut down the attendance rate at all different places plus make people a lot more happy” (DGH ED doctor). However, the travelling community highlighted that the current generation of parents are often unfamiliar with information technology: “But the new generation when they get a bit older, in a couple of years from now, cause all the children now they're all permanently at school that would help them but not for all us, not for this generation” (travelling community mother).
Audiovisual material
A benefit of internet-based resources, highlighted by parents and clinicians, is that they could include short video clips showing signs and symptoms, presenting information that is difficult to explain verbally or in diagrams. Parents suggested clips of sounds of specific coughs (croup, whooping cough), respiratory movements (recession) or the appearance of different rashes (chickenpox, meningitis). Conditions that were suggested for video format by clinicians, some of which matched those suggested by parents, were croup, wheeze, increased work of breathing, recession, bronchiolitis, dehydrated child, floppy child, seizures and fainting, tracheal tug, capillary refill time and rashes. Parents highlighted that these could be viewed, for example, on a mobile phone while holding a baby. Audiovisual material was the preferred option for families with low literacy: the Asian British and travelling communities highlighted that some families would not be able to read written language. Limitations of audiovisual material were however recognised: “[Doctor 1] Photos are very difficult because even if you look at the different atlases we have for dermatology… [Doctor 2] and each book looks slightly different [Doctor 3] And it can be falsely reassuring can't it. ‘Cause you have meningococcal disease, you can have a blanching rash” (paediatric ED doctors).
It is important to note that in addition to discussing information resources, parents and clinicians alike highlighted that for worried parents, nothing will replace face-to-face reassurance from a healthcare professional: “only physical contact with somebody who you trust and feel can answer your question will ever give you the reassurance with regards to a child that you're looking for… ultimately you really just want to speak to someone and show them your child, you want to speak to someone who you feel is experienced and knowledgeable about what you are talking about and can help you with your child” (white British mother); “verbal advice can reassure you, I don't think any website or any information can reassure you” (DGH ED doctor). This message came across particularly strongly from the Asian British community.
Discussion
Principle findings and implications
Coproduction
Parents and clinicians described a diverse range of desirable attributes for safety netting advice, as well as techniques for its delivery. This highlights the need for true coproduction of safety netting resources by parents and clinicians, throughout every stage of design and development of resources, to ensure that they meet the range of criteria identified as important by both groups. This mirrors the key principle of the Children and Young People's Health Outcome's Forum regarding family involvement in the development of services.2 Safety netting is a perfect example of where true coproduction by clinicians and parents could result in the development of effective resources which will be utilised and valued by both groups.
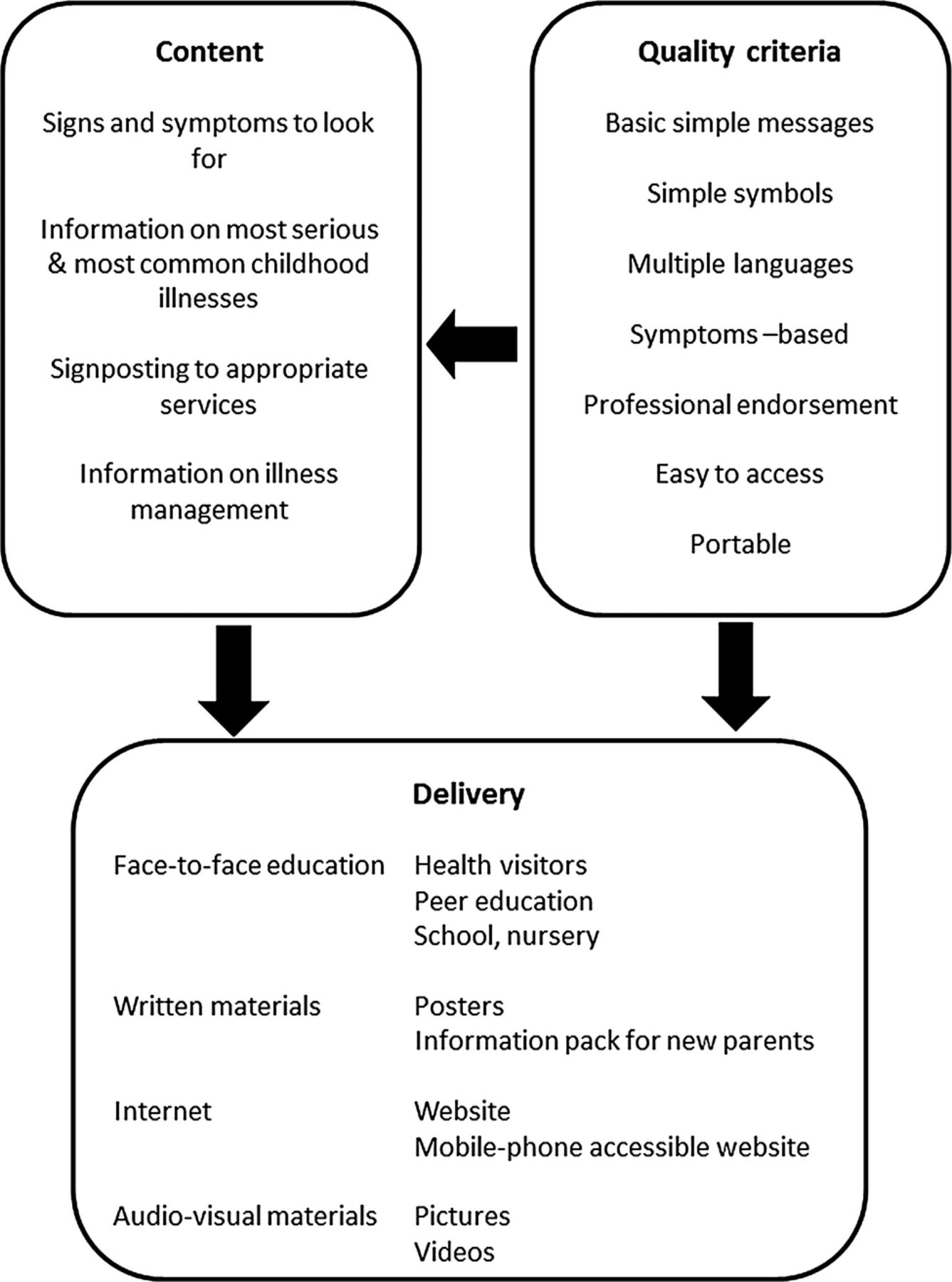
There were some important differences between groups, for example, while clinicians in all settings, and many parents, favoured the idea of internet-based and phone-based resources, the travelling community highlighted that this would not be appropriate for the current generation of parents; and the Asian British and travelling communities highlighted that some families would not be able to read written English, thus particularly preferring audiovisual materials. However, generally parents and clinicians from different communities/settings suggested a very similar range of content, quality criteria, format and delivery methods for safety netting advice, while acknowledging that multiple techniques and resources are needed. (Note, however, that the number of participants from each community/setting was small which limited our ability to draw comparisons.) Previous research in the UK has also found commonality of parental information needs across different socioeconomic groups regarding childhood illness.20 The good degree of agreement between the subthemes emerging from the two groups highlights the potential for the development of safety netting techniques which are indeed endorsed by parents and clinicians. Figure 1 shows desirable safety netting attributes that were proposed by both parents and clinicians: resources should be developed that meet these criteria.

{kind=link}
Content, quality criteria and delivery mechanisms for safety netting information, suggested by the parents and clinicians.
Multifaceted approach
Participants recognised that one approach will not be appropriate for all parents, and that a variety of techniques and resources are needed. For example, written materials are not suitable for those with low literacy; and websites are not suitable for those who lack confidence in, or access to, the internet and smart phones. There may be a need for a tailored approach to meet individual needs.
An information leaflet for parents on feverish illness has already been developed by the NICE21; yet the information is not multifaceted or tailored for different groups, and none of the clinicians reported using the leaflet for safety netting. Providing more multifaceted, tailored information coproduced with parents may better meet the requests of parents and clinicians. Furthermore, the information leaflet meets some of the key criteria presented in figure 1 (including signs and symptoms to look for, information on illness management, professional endorsement), but it could perhaps be improved by including other key criteria including simple symbols, pictures and videos.
Delivery
Participants were imaginative in their consideration of how safety netting advice could be delivered; ideas included DVDs, television programmes, rolling displays in waiting rooms, posters, booklets, leaflets, flashcards and even quizzes. Media campaigns were thought to have been successful at improving knowledge in other areas of health, and could be applied to childhood illness; however, clinicians warned against creating anxiety. Furthermore, it would be difficult to design and deliver a successful media campaign for such a broad topic as acute childhood illness. Clinicians also warned against falsely reassuring parents; for example, emphasising a non-blanching rash in pictures may prevent children with meningococcal disease being presented before the appearance of this symptom. There is a balance to be met between creating false reassurance and over-anxiety.3
Types of information
It was commonly suggested by the parents and clinicians that there is a need for different types of information to be delivered at different times:
-
Specific information: provided when children are sick (usually during a consultation), specific to the particular illness the child is experiencing.
-
Symptom-related information: accessible by parents preconsultation when their children are sick and could also be provided during a consultation.
-
General information: education for parents on childhood illness in general.
Regarding specific illness-related or symptom-related information, a common proposal was for a well-signposted website on childhood illness, with professional endorsement, that is easy for parents to search and provides the information they need when their child is sick. Previous research has similarly revealed parental need for consistent advice from a trusted source, and a preference for NHS-branded websites compared with other internet resources.20 Our participants also frequently suggested that this should be compatible for use on mobile phones so that parents can access it easily while caring for their child. The inclusion of pictures and videos would increase the accessibility. A variety of symbols were suggested which could be used in such resources including sad and happy faces and different coloured symbols.
Parental need for high-quality internet-based resources is not surprising given the evidence that parents are increasingly using the internet to access health information. In two independent surveys, 52% of parents had sought health information for their children on the internet22 ,23; however, the quality and accuracy of internet advice are variable.24
Regarding general information, both groups suggested that education could be delivered by health visitors or by peers in the community, with the important caveat of ensuring that the information delivered is correct. We have recently completed a systematic review of the effectiveness of interventions providing information on when to seek medical help for parents of acutely sick children (Neill et al, personal communication). Characteristics of interventions likely to be more effective included comprehensive information, information on how to assess the severity of their child's illness as well as home management advice and reinforcement from healthcare professionals. These match some key criteria summarised in figure 1. Interventions which were codesigned with parents were also more effective, again reinforcing the importance of this approach.
Strengths and limitations
This study has taken a first step at identifying the optimal content, format and delivery of information resources for parents of acutely sick young children, from the perspectives of parents and clinicians. Including parents and clinicians strengthened our study because in order to be effective, resources must be endorsed and valued by both groups. Indeed, we identified similar needs from both groups, indicating the possibility of developing resources which are coproduced. Furthermore, we included diverse groups of parents with different literacy levels, information needs and ability to use information technology, ensuring that the views of different groups with diverse needs are understood. A range of doctors and nurses from different settings were also included, allowing us to include the perspectives of the broad group of clinicians who provide safety netting advice in different settings. However, while the maximum variation sampling provided us with participants with a diverse range of characteristics, the qualitative approach means that the extent to which the findings are generalisable to others in the same or different groups and geographical locations is not known. Data were collected and analysed by a team of researchers with different backgrounds, so their range of perspectives helped to reduce bias and facilitated a deeper understanding.
Conclusion
A multifaceted and tailored approach to safety netting is needed, in which information is delivered in multiple ways and is accessible to different groups of parents with varying needs, resources and abilities. It is important that resources are coproduced with parents and clinicians so that they are accessible to and understood by parents, as well as endorsed by clinicians. This study has shown that it is possible to identify common priorities among both groups regarding resource development.
Research is needed to determine the effectiveness of different components of safety netting resources and the impact on parent knowledge, understanding, satisfaction, anxiety and reconsultation rates, among other outcomes. There is also a need for the development of safety netting quality standards to ensure that all clinicians provide parents with appropriate advice, and so that all parents receive the correct information in an efficient way. This study is a first step towards developing testable safety netting interventions and developing an evidence base around safety netting on which to base quality standards.
Acknowledgments
The authors would like to thank the participants for taking part, and all those who coordinated the recruitment.
References
Footnotes
-
Contributors SN, ML, DR and MT conceptualised and designed the study. SN and HSM collected the data. CHDJ and SN analysed the data. CHDJ drafted the manuscript. All the authors read and approved the final version.
-
Funding This publication presents independent research funded by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research funding scheme (RP-PG-0407-10347) and arising from a Career Development Fellowship supported by the NIHR (MT). The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
-
Competing interests ML was the clinical director leading development for the NICE feverish illness guidelines, was a NICE fellow from 2010 to 2013 and is on the NHS evidence advisory board.
-
Ethics approval East Midlands—Nottingham 2 NHS Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.