Article Text

Abstract
Objective Comparison of recent national survey data on prevalence, awareness, treatment and control of hypertension in England, the USA and Canada, and correlation of these parameters with each country stroke and ischaemic heart disease (IHD) mortality.
Design Non-institutionalised population surveys.
Setting and participants England (2006 n=6873), the USA (2007–2010 n=10 003) and Canada (2007–2009 n=3485) aged 20–79 years.
Outcomes Stroke and IHD mortality rates were plotted against countries’ specific prevalence data.
Results Mean systolic blood pressure (SBP) was higher in England than in the USA and Canada in all age–gender groups. Mean diastolic blood pressure (DBP) was similar in the three countries before age 50 and then fell more rapidly in the USA, being the lowest in the USA. Only 34% had a BP under 140/90 mm Hg in England, compared with 50% in the USA and 66% in Canada. Prehypertension and stages 1 and 2 hypertension prevalence figures were the highest in England. Hypertension prevalence (≥140 mm Hg SBP and/or ≥90 mm Hg DBP) was lower in Canada (19·5%) than in the USA (29%) and England (30%). Hypertension awareness was higher in the USA (81%) and Canada (83%) than in England (65%). England also had lower levels of hypertension treatment (51%; USA 74%; Canada 80%) and control (<140/90 mm Hg; 27%; the USA 53%; Canada 66%). Canada had the lowest stroke and IHD mortality rates, England the highest and the rates were inversely related to the mean SBP in each country and strongly related to the blood pressure indicators, the strongest relationship being between low hypertension awareness and stroke mortality.
Conclusions While the current prevention efforts in England should result in future-improved figures, especially at younger ages, these data still show important gaps in the management of hypertension in these countries, with consequences on stroke and IHD mortality.
- Epidemiology
- Public Health
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Article summary
Article focus
-
Comparison of hypertension prevalence, awareness, treatment and control in three National studies in England, the USA and Canada.
-
Correlation with stroke and ischaemic heart disease mortality.
Key messages
-
Important variation by country.
-
Strong relationship between hypertension indicators and stroke mortality.
-
Gaps in the management of hypertension.
Strengths and limitations of this study
-
National population data.
-
Detailed data on hypertension characteristics.
-
Strong correlation with meaningful outcome, mortality.
-
Data from England from 2006, but they provide an important basis for measuring progress (current data not yet available).
-
Limited to three countries.
-
Ecological correlation with mortality that excludes looking at confounders.
Introduction
Increased blood pressure is the leading risk factor for premature death, stroke and heart disease worldwide.1 In the year 2000, the world was estimated to have close to 1 billion people with hypertension and predicted an increase to 1.56 billion by 2025.2 The global economic burden of increased blood pressure was estimated to consume US$370 billion worldwide and 10% of healthcare expenditures.3 Usual blood pressure is strongly and directly related to vascular and overall mortality without evidence of a threshold down to at least 115/75 mm Hg,4 with small changes in blood pressure resulting in substantial changes in vascular disease.5
On the basis of clinical and population research, increased blood pressure, hypertension and hypertension-related complications are largely preventable. Lifestyle changes can lower blood pressure and prevent hypertension while antihypertensive drug therapy can effectively reduce the cardiovascular events attributed to hypertension.1–6 Nevertheless, most people with hypertension worldwide are not effectively treated and controlled to the recommended blood pressure targets.7 There are few national programmes to serve as models for prevention and control of hypertension and few countries have embarked on national hypertension prevention and control programmes. The USA blood pressure education programme was established in 19728 while Canada (2000) and England (2004) have recent initiatives.9 ,10 This manuscript compares recent data on the prevalence, awareness, treatment and control of hypertension in England, the USA and Canada and correlates these hypertension-related parameters in the three countries with mortality from stroke and ischaemic heart disease (IHD).
Methods
Survey methods used in England, the USA and Canada are summarised in table 1. Detailed methodology for each survey is available elsewhere.11–13 Briefly, each survey is a representative sample of each country's non-institutionalised population and uses standardised protocols and devices. While the England (2006) and Canada (2007–2009) surveys used automatic oscillometric devices, the USA (2007–2010) survey used mercury wall sphygmomanometer models. The number of blood pressure measurements available for analysis varied by count of blood pressure measures and survey protocols (table 1).
Survey methods, by country
In these analyses, hypertension was defined as a mean systolic blood pressure (SBP) ≥ 140 mm Hg or a mean diastolic blood pressure (DBP) ≥90 mm Hg or a respondent self-report of medication to lower blood pressure. Prehypertension (SBP 120–139 or DBP 80–89 mm Hg), stage 1 (SBP 140–159 mm Hg or DBP 90–99 mm Hg) and stage 2 (SBP ≥160 mm Hg or DBP ≥100 mm Hg) hypertension were defined according to the Seventh Report of the Joint National Committee on the Prevention, Detection, Evaluation and Treatment of High Blood Pressure (JNC 7) definitions.6
Prevalence, awareness, treatment, control and awareness of hypertension were defined using commonly recognised standards. Prevalence was defined as SBP ≥140 or DBP ≥90 or currently taking medication to lower their blood pressure. Awareness was defined by self-report and included, having been diagnosed as hypertensive by a doctor or nurse, excluding women diagnosed during pregnancy (England), medication to lower blood pressure in the past month or reported high blood pressure (Canada) or having been diagnosed as hypertensive by a doctor or nurse, excluding women diagnosed during pregnancy (USA). Treatment was defined as taking medication to lower blood pressure, as recorded by the nurse (England), or a self-report of taking medication to lower blood pressure (Canada and the USA). Treated and controlled was defined as taking medication to lower blood pressure and SBP<140 and DBP <90 mm Hg; treated and uncontrolled a SBP ≥140 or DBP ≥90 mm Hg while on medication to lower blood pressure. Aware, yet not treated, was defined by self-report and included having been diagnosed as hypertensive by a doctor or nurse (England)/healthcare provider (Canada and the USA) and not taking medication to lower blood pressure.
Survey data were not age and sex standardised. They represent the current country-specific figures and therefore correspond more precisely to each country's crude mortality rates for stroke and IHD. All prevalence figures are weighted using survey weights to represent each country's population. SEs were computed taking into account each country's sampling methodology.11–13 To be comparable across the three surveys, the analysis was restricted to individuals aged 20–79 years and excluded pregnant women. The Canadian Health Measures Survey (CHMS) data analysis was performed using the SAS Enterprise Guide (V.4.1, SAS Institute Inc, Cary, North Carolina, USA, 2006). The Health Survey for England (HSE) data analysis was performed using SPSS V.19. The National Health and Nutrition Examination Survey (NHANES) data analysis was performed using SAS V.9.2 and SAS-Callable SUDAAN V.10 (RTI International)), to account for the complex sampling design.
The latest WHO country-specific mortality data available were from 2008 for Canada and the USA,14 and we used the 2006 data for England.15 Crude mortality rates per 100 000 were obtained for men and women for stroke and ischaemic heart disease (IHD) and plotted against country-specific prevalence data for hypertension awareness, treatment and control.
Results
The distribution of SBP and DBP by sex, age and country shows an increase in SBP with age and an increase, plateau and decrease in DBP with ageing (figure 1; see online supplementary appendix 1 table). SBP is higher in men than women in the younger age groups and becomes higher in women than men after age 60 years in Canada and age 70 years in England and the USA. The mean SBP is overall higher in England than in the USA and Canada in all age-gender groups. DBP is similar in the three countries before age 50 and then falls more rapidly in the USA while being lower overall in men and women from the USA.

Distribution of systolic and diastolic blood pressure by country, age and sex.
The distribution of measured blood pressure (including treated individuals), by level, in table 2 reflects the findings in figure 1. Only 34% of adults aged 20–79 years would be classified as having a normal blood pressure (<120/80 mm Hg) in England, compared with 50% in the USA and 66% in Canada. Prehypertension and stages 1 and 2 hypertension prevalence figures are also much higher in England than in the USA and Canada.
Distribution of measured blood pressure by level, sex, age and country
The prevalence of hypertension, and awareness, treatment and control levels among those with hypertension are shown in table 3. The prevalence of hypertension is lowest in Canada (19·5%) and higher in the USA (29%) and England (30%). Hypertension awareness is close to 80% in the USA (81%) and Canada (83%) and lower in England (65%). England also has lower levels of hypertension treatment (England 51%; the USA 74%; Canada 80%) and control (England 27%; the USA 53%; Canada 66%). These patterns are similar in the different age and sex subgroups (table 3). Among individuals treated for hypertension (ie, taking medication to lower blood pressure), the proportion being controlled is lowest in England (53%), compared with 71% in the USA and 82% in Canada.
Hypertension prevalence and percentage with hypertension, aware, treated, controlled, by sex, age group and country
The mean SBP and DBP are provided in online supplementary appendix 2 by the different prevalence categories of table 3. The data are consistent with those in the previous tables showing the highest SBP mean in England in all categories. For DBP also, England has higher means than the USA and Canada among all hypertensives and the aware and treated categories.
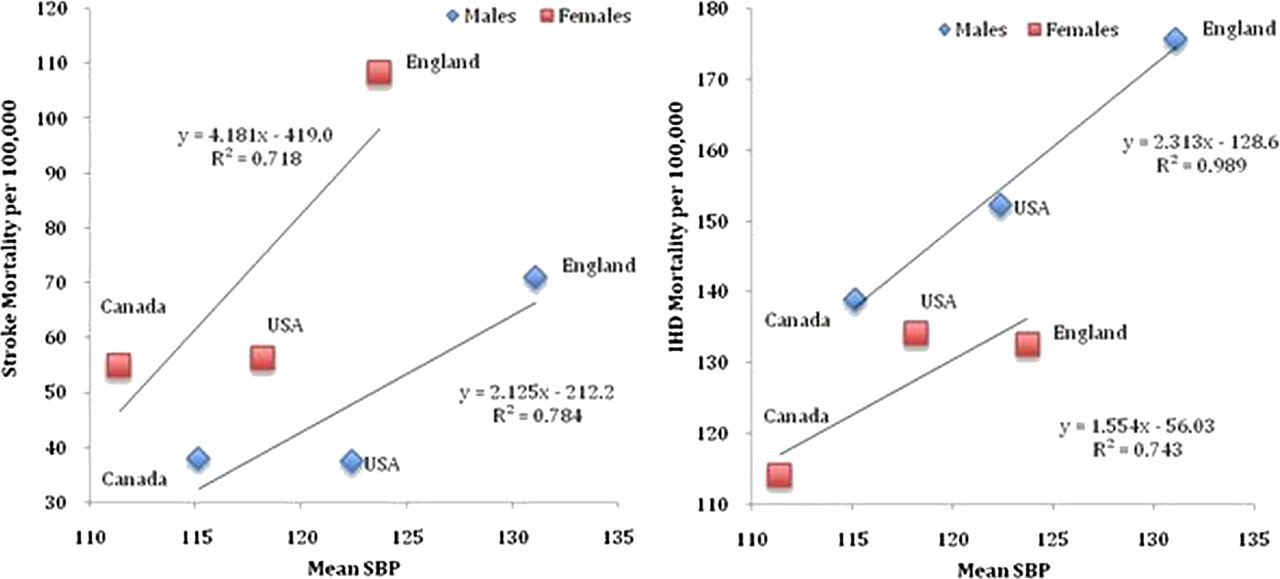
At the time when these surveys were being conducted, Canada had the lowest stroke and IHD mortality rates while England had the highest. The rates of both outcomes were inversely related to the mean SBP in each country (figure 2). We found a strong relationship between the selected blood pressure indicators and stroke and IHD mortality, the strongest relationship being between hypertension awareness and stroke mortality, especially in women (figure 3). Stroke rates were higher in women than men for any level of each of the BP indicators, and the opposite was true for IHD (figures 2 and 3).

Stroke and ischaemic heart disease (IHD) mortality* by country mean SBP.

{kind=link}
{kind=link}
{kind=link}
Stroke and IHD mortality by country prevalence of hypertension awareness, treatment and control.
Discussion
Although all the three countries evaluated have had substantive improvement in most hypertension treatment indicators over the past two decades,16–20 this study found marked differences in hypertension prevalence, awareness, treatment and control rates in England, the USA and Canada. Canada has the lowest prevalence of hypertension at 19% followed by England and the USA at about 30% each. A previous study based on earlier cycles of these surveys also found little difference in the prevalence of hypertension between England and the USA.21 The main determinants of hypertension are known. These include poor dietary habits, excess sodium intake, physical inactivity, obesity, excess alcohol consumption, as well as age, gender, race and sociodemographic factors. The national differences in prevalence are most likely related to differences in the interaction between these determinants as well as differences in the clinical systems, community programmes and environmental and policy supports for hypertension prevention and management. Compared to the USA, Canada has a lower rate of obesity, but to our knowledge there has never been a comprehensive comparison of the determinants of blood pressure using appropriately adjusted data in these countries. A comprehensive comparison of the determinants of hypertension and the policies that fail to address adverse differences in the modifiable determinants would be an important next step. This is also important since these data show an important difference in the younger age groups between England, Canada and the USA. Since blood pressure tracks with age,22 efforts to influence the determinants of hypertension are essential to reduce hypertension prevalence in the older age groups. The recent decrease in childhood obesity in England23 should be followed by a reduction in blood pressure in the future surveys.
Our study has also found important differences in the awareness, treatment and control of hypertension in the three countries. England, the USA and Canada all have developed differing approaches to improve hypertension treatment and control. In the USA, several diverse approaches have been taken.6 ,8 ,24 Historically, the USA has had one of the world's highest rates of hypertension awareness, treatment and control and has also seen improvements in these indicators with intensified efforts18; however, despite broad clinical and community efforts, over half of the adults with hypertension are uncontrolled based on the current guidelines.19 Recent national activities and recommendations are staged to positively impact hypertension estimates.25–29
Importantly, we also found national-level differences in mortality rates from stroke and IHD, which paralleled the differences in hypertension awareness, treatment and control between these three countries. Stroke and IHD mortality were strongly inversely correlated with mean SBP in each country.
Efforts in England have included episodic national hypertension recommendations developed by the British Hypertension Society (BHS—a non-governmental organisation of specialists and researchers) with the recommendations recently being developed by a governmental organisation in collaboration with the BHS.30 Implementation programmes have included an extensive public programme to educate people on the risks of salt for hypertension31 and also an extensive government programme to make bonus payments to general practitioners for achieving benchmarks for hypertension care32—although the efficacy of payment for performance for improving hypertension control has been questioned.33
In 2000, Canada launched an annually updated hypertension recommendations programme (Canadian Hypertension Education Programme (CHEP)).9 In 2006, the programme was assisted by an extensive initiative to inform the public about hypertension and the health risks and opportunities to reduce dietary salt.34 The introduction of CHEP in Canada is temporally related to improvements in management patterns and has also been temporally associated with reduced cardiovascular disease in Canada.35
It is difficult to assess how much the different national approaches to hypertension detection and management impact on the differences observed in our study. British Guidelines in place in 200610 ,36 and since30 do not recommend the routine use of antihypertensive treatment for those with a SBP >140 and/or DBP >90 mm Hg; rather, they do so only if such people have an estimated 10 year CV risk of >20%. Consequently, treatment rates and control rates might be expected to be lower in England than in the USA and Canada. Furthermore, in England, the National Institute for Health and Clinical Excellence's Quality and Outcomes Framework, which includes measures used in the calculation of provider reimbursement, included a higher blood pressure target (<150/90) during the period of data used for these analyses. This will be lowered (to <140/90) in 2013/2014 to align with the national guidelines. In addition to the new National Institute for Health and Clinical Excellence guidelines,30 the national salt reduction programme in England would be expected to result in further reductions in the prevalence of hypertension and improvement in hypertension treatment indicators in recent and future years as Canadian and Finnish data suggest.37 ,38
There are several potential limitations to our current analyses. In addition to the low response rates and hence small numbers in some strata, each country uses different methodology to assess blood pressure and relatively small differences in blood pressure can impact the hypertension indicators. In particular, Canada has adopted the use of a fully automated blood pressure device that operates in the absence of an observer and averages the last five of six blood pressure readings. The Canadian method reduces the influence of the observer (white coat effect) on blood pressure and results in a slightly lower average blood pressure than a single auscultatory blood pressure reading. Nevertheless, using an algorithm to adjust the data in the Canadian survey39 to represent a single manual reading results in little change in the major hypertension indicators as the difference in methods at the therapeutic cut point of 140/90 mm Hg is relatively small but might reduce the differences between the USA and Canada. The close relationship between stroke mortality and hypertension prevalence and hypertension indicators suggests that the blood pressure and hypertension differences seen in this study are real and biologically important. We acknowledge the limitation of using three points for our mortality graphs, which require a high level of correlation to be statistically significant.
We did not use age-adjusted or gender-adjusted data from the different countries. The lack of adjustment was intended so that the hypertension risk factors could be directly compared to stroke mortality for each country. In addition, in a separate analysis, comparison of age-adjusted data to a common standard population showed very little difference with the current figures. We were not able to obtain more recent common mortality data than 2008 for all countries. There is some overlap between the timing of the US and Canadian surveys, but the English survey was conducted more than 1 year earlier. Management of hypertension in England is quite likely to have improved since 2006. Increased blood pressure and hypertension represent major global threats to population health, with stroke and IHD being the most closely related adverse outcomes.4 Interventions to lower the average population blood pressure and interventions to identify and control blood pressure in those with hypertension are critical to prevent blood pressure-related complications.2–6 Nevertheless, the hypertension control rates are low even in developed countries and most countries do not have formal programmes to control hypertension.40 Further, population surveys indicate that approximately 29% of men and 25% of women have uncontrolled hypertension with increasing numbers of hypertension cases globally due to population growth and ageing.41 Hence, countries worldwide should consider introducing and evaluating coordinated programmes to improve the prevention, detection, awareness, treatment and control of hypertension, and our data suggest that the more assertive approach apparent in North America is associated with large benefits in terms of reduced cardiovascular mortality. A greater focus on prevention of high blood pressure in the younger age groups is also necessary.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
- Data supplement 2 - Online tables
Footnotes
-
Contributors MJ, EF, CG and CR contributed to the data analysis, interpretation and writing. FL, NP, FAM, HJ, OB and NC contributed to the data interpretation and writing.
-
Funding Funding for NHANES comes from two primary sources: direct funding through the NCHS base budget and reimbursable funding from collaborating agencies; The Health Survey for England was funded by the National Health Centre; Health Canada and the Public Health Agency of Canada supported Statistics Canada in obtaining federal funding for the Canadian Health Measures Survey. Other sources of support: FAM is supported by an Alberta Innovates Health Solutions Senior Health Scholar Award and the University of Alberta/Capital Health Chair in Cardiovascular Outcomes Research. NC holds the Heart and Stroke Foundation of Canada CIHR Chair in Hypertension Prevention and Control. NP is grateful for support from the NIHR Biomedical Research funding scheme and the NIHR Senior Investigator Award. Funding of the original surveys.
-
Statement of independence of researchers from funders The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention, the Public Health Agency of Canada or the UK Department of Health.
-
Competing interests NP reports grants from Pfizer and from Hypertension Trust and personal fees from various Pharma companies, as well as from Servier, outside the submitted work. NC receives salary support for an HSFC CIHR Chair in Hypertension Prevention and Control.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement All the authors had access to the original tables from the different studies, So no additional data are available.