Article Text

Abstract
Objective To assess factors related to use and non-use of a sophisticated interactive preventive health record (IPHR) designed to promote uptake of 18 recommended clinical preventive services; little is known about how patients want to use or be engaged by such advanced information tools.
Design Descriptive and interpretive qualitative analysis of transcripts and field notes from focus groups of the IPHR users and of patients who were invited but did not use the IPHR (non-users). Grounded theory techniques were then applied via an editing approach for key emergent themes.
Setting Primary care patients in eight practices of the Virginia Ambulatory Care Outcomes Research Network (ACORN).
Participants Three focus groups involved a total of 14 IPHR users and two groups of non-users totalled 14 participants.
Outcomes/results For themes identified (relevance, trust and functionality) participants indicated that endorsement and use of the IPHR by their personal clinician was vital. In particular, participants’ comments linked the IPHR use to: (1) integrating the IPHR into current care, (2) promoting effective patient–clinician encounters and communication and (3) their confidence in the accuracy, security and privacy of the information.
Conclusions In addition to patients’ stated desires for advanced functionality and information accuracy and privacy, successful adoption of the IPHRs by primary care patients depends on such technology's relevance, and on its promotion via integration with primary care practices’ processes and the patient–clinician relationship. Accordingly, models of technological success and adoption, when applied to primary care, may need to include the patient–clinician relationship and practice workflow. These findings are important for healthcare providers, the information technology industry and policymakers who share an interest in encouraging patients to use personal health records.
Trial Registration Clinicaltrials.gov identifier: NCT00589173
- Primary Care
- Preventive Medicine
- Qualitative Research
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Article summary
Article focus
-
What are necessary elements for patient engagement in advanced interactive personal health records?
Key messages
-
Engagement in an interactive prevention health record (IPHR) is related to integration into current care and the patient–clinician relationship.
-
Models of technology success and acceptance may warrant modification when applied to primary care use of the IPHRs.
Strengths and limitations of this study
-
An advanced IPHR shown to increase use of preventive services was employed for the study.
-
The sample was drawn from northern Virginia, USA. Other locales may have different the IPHR needs and require different strategies to engage patients in the IPHR use.
-
Most participants had ongoing established relationships with their clinician.
Background
The concept of patient-centred care is not new to medicine.1 ,2 Decades ago, research demonstrated that engaging patients in their care improves patient satisfaction, quality of care and clinical outcomes.3 ,4 Recently, national movements aimed at transforming healthcare have formally defined, incentivised and institutionalised patient-centred care. The goals of the Patient-Centered Medical Home espouse these principles.5 ,6 State and national legislation combined with payer initiatives now encourage and support practices to provide patient-centred care.7 ,8 The national Meaningful Use Roadmap defines patient and family engagement from a patient perspective as ‘actions we must take over time to obtain the greatest benefit from the healthcare services available to us’, further stating that engagement is desirable and necessary for health information systems.5 ,9 ,10
Personal health records (PHRs) are an important resource to help practices provide patient-centred care. Currently, the most common functions performed by PHRs include record keeping, secure messaging, appointment scheduling and bill payment.11 Yet, other PHR features could help facilitate patient engagement in their medical care, including use of plain English depictions of clinical data, motivational messages to seek needed care, educational resources, decision aids and resources and tools to support and guide care.12 ,13
While electronic PHRs have been available for more than a decade and have wide adoption in some large healthcare organisations,14 ,15 they are used by only a fraction of Americans, and practices struggle to promote patient adoption.11–23 One possible reason for poor PHR uptake is that many systems lack integration into the care delivery system, including clinicians’ EMRs.13 ,17 ,21 Tang and Lee suggest that integrated PHRs could provide patients better access to laboratory and other data, as well as communication with their cliniciani. This, they posit, will facilitate ‘the type of physician–patient relationship that will improve health.’19
To date PHR adoption has typically been approached from clinician23 ,24 or technology-driven24 ,25 perspectives, operating under the assumption that increasing the number of clinicians using an EMR will increase the number of patients who use a PHR.23 National survey data suggest and others have advocated that patient PHR adoption would better increased by designing and promoting more patient-centred PHRs that consider patients’ individual and cultural issues as well as promote the patient–clinician relationship.12 ,22 Similarly, even widely cited models of technology promotion, such as the Model of Information Systems Success (MISS)26 and the Technology Acceptance Model,27 have often been applied to healthcare with little patient or clinician perspective28 ,29 or by purposively eschewing ‘person-to-person trust’ in evaluating such models.25 To our knowledge, no one has evaluated these models in a patient-centred PHR shown to improve patient outcomes.
In 2007, we created an IPHR that was designed with greater functionality to engage and activate patients in their preventive care. Details about the design of the IPHR,30 findings from a randomised controlled trial demonstrating that the IPHR significantly improved preventive care31 and a how-to-guide showing practices how they can use their PHRs to better promote preventive care, have been previously published.32 The IPHR was not meant to be a complete PHR or to replace commercial systems. It did not contain common administrative functions, such as secure messaging, appointment scheduling or bill paying. Rather, the IPHR was meant to be patient-centred, action-oriented, prevention-focused application that functioned within existing PHRs. Briefly, the IPHR combined a patient's clinical information from his/her clinician's EMR (eg, history, dates and results) with patient-reported information (eg, family history and health behaviours). The IPHR robustly applied this information to national guidelines from the US Preventive Services Task Force and six other guidelines to provide a very personalised overview of recommended preventive services.33–40 All recommendations include personalised explanations of the information in plain language, tailored motivational messages, links to additional educational resources and decision aids, tools to promote action and periodic reminders. The information is shared with both the patient through the IPHR portal and their clinician via their EHR.
While multiple studies have evaluated why patients use PHRs with more basic functionality,10 ,16 less is known about their interests in and engagement with PHRs with more advanced patient-centred functionality as provided by the IPHR. As part of our ongoing trials, we used qualitative methods to capture perspectives from both ‘users’ and patients who were invited to use the IPHR but did not use the system (‘non-users’), with a lens towards informing the knowledge gaps and varying viewpoints about PHR adoption noted above. As framed by Kuzel,41, this inquiry was “driven not by a need to generalise or predict, but rather by a need to create and test… interpretations.”
Methods
Design
We employed descriptive and interpretive analysis of focus group transcripts and field notes, with data reduction via coding and editing for development of major themes and subthemes. We then used a combination of grounded theory and editing analysis42 with initial codes derived from key emergent themes from our interpretive analysis. A trained moderator led the focus groups, using broad-based questions to explore patients’ perspectives about the IPHR and PHRs in general. A focus group guide was used to ensure consistency of procedures, questions and discussion topics. The guide, developed from ‘discussions with experts familiar with the topic’,42 and focus group process were based on the methods described by Crabtree and Miller42 and by McNamara.43 At the beginning of each patient focus group, participants completed a brief printed questionnaire eliciting demographic characteristics and information about interactions with their clinician. The study was approved by the Virginia Commonwealth University Institutional Review Board.
Sample
All participants were patients from one of eight family medicine practices that were located in northern Virginia and participated in the Virginia Ambulatory Care Outcomes Research Network (ACORN). In order to address sampling adequacy, a minimum total of 12 participants in both user and non-user groups was targeted.44 During the first 4 months the IPHR was available to the practices, 229 of the 2250 patients randomly selected and mailed an invitation used the tool (completed registration and entered data on the website). All of these patients were invited through email to participate in focus groups. Of the 44 who expressed interest, 30 selected to provide a range of ages, genders and practice locations were asked to participate in three user focus groups. (The first user group was rescheduled due to inclement weather and 3 of 10 participants ultimately attended. The next two groups had 5 and 6 of 10 invited participants attend, respectively.) Of the 2021 non-users, a random sample of 150 patients, stratified by age, gender and practice location, were mailed focus group invitations. From the 32 patients who responded to the letter, 20 selected to provide a range of ages, genders and practice locations were asked to participate in two non-user focus groups; 14 attended. Each participant received a $50 gift card incentive.
Procedures
Focus groups, each approximately 1.5–2 h in duration, were held at a location near the participating practices. Group discussion was guided by semistructured questions with probes and prompts to provide follow-up lines of inquiry, clarify topics and stimulate further discussion. The user and the non-user groups were shown screen-shots demonstrating how the IPHR worked at appropriate times during the groups so all participants could comment on the IPHR attributes and uses. Sessions were audio-recorded, and the transcriptions of the recordings were then corrected as necessary through comparison with the original recordings. Field notes were also taken to capture aspects of the group interaction that would not be identified on recordings. This included such observations as participant body language and tone, as well as researcher thoughts and reactions.
Transcripts and field notes underwent descriptive analysis with a provisional categorical structure based on focus group question guides. Data were combined with field notes to explore descriptive similarities and differences within and between the groups. Coding and editing of transcripts and field notes were used to derive higher level themes and explanations, and tentative explanations of findings were based on both our data and relevant literature. A four-member team (JWK, AHK, DRL and AJK) performed each step of the analysis independently. Differences in coding, development of themes and derivation of tentative explanations were discussed by the team until consensus was reached. Model development ensued (AHK and JWK), building on key emergent themes from the interpretive analysis. Initially concentrated on contextual thematic interrelationships (eg, linked Venn diagrams), resultant thematic modifications resulted in iterations of models which were ‘based on both process and causal considerations’.26
Results
Study population
The patients who used the IPHR during the study period were primarily men (56%), white (85%) and more than 50 years old (68%). Of the 50 patients who agreed to participate in focus groups (30 users and 20 non-users), 28 patients attended the sessions, including 14 PHR users and 14 non-users (table 1). Focus group participants were predominantly women (64%), white (93%), over 50 years old (86%) and all reported having attended at least some college. Nearly allii participants rated their health as good to excellent, stated they had been with their clinician at least 3 years, and rated their clinician highly.
Focus group participants
All but one focus group participant acknowledged using the internet daily, and some described ‘constant’ internet use for job and personal purposes. Although nearly all stated that they did not use the internet as often for health-related matters as for other needs, they did report using the internet to garner health information, primarily for themselves and their family.
Themes
Across all five focus groups,iii three major themes emerged about how participants wanted to be engaged by PHRs: they wanted (1) novel content that was relevant to their immediate and ongoing care, (2) a PHR they could trust for accuracy, security and privacy and (3) a highly functional PHR, facilitating care and communication with their clinician, and providing access to comprehensive personalised information shared with the clinician. Although practical usefulness was said to be essential, a major reason why participants said they trusted, used and sought relevance in the IPHR was that it was offered to them by their personal clinician.
Relevance
A few participants noted that upcoming appointments with their clinician made the IPHR use more compelling, contributed to their registering, and led them to notice the content pertinent to that visit. Most, however, reported that the invitation for the IPHR was received at a time unassociated with an office visit or any specific healthcare needs. Indeed many participants reported that as a result they did not feel a pressing need to immediately register for and use the IPHR (table 2). A few non-users declared that they just had not gotten around to registering. Many participants in the non-user and the user groups voiced the opinion that they could access similar information on the internet, and that they did not recognise that the IPHR content was personalised to their needs. Some users commented that they had already fully addressed their preventive healthcare needs with their clinician.
Representative participant comments on relevance of the interactive prevention health record (IPHR) (Why they didn't feel a need to register)
Trust
Nearly all participants vigorously discussed three components of trust necessary for them to use a PHR: security (protecting their health information), privacy (not sharing their health information with others) and accuracy (ensuring that the clinical content and health recommendations proffered by the system were correct and appropriate for them; table 3). Most participants reported trusting the IPHR because it was recommended and used by their clinician's practice. A few participants in the non-user groups indicated discomfort with having any of their personal health information on the internet. However, most participants in all groups expressed the view that clinician endorsement of the IPHR was an indication that their personal health data were secure. Most participants also expressed strong opposition to PHRs developed by commercial entities and to sharing their health information with their insurance company due to the risk of future denial of coverage.
Representative participant comments on trust of an interactive prevention health record (IPHR)
Nearly all participants reported having had difficulties distinguishing between accurate and inaccurate health information on the internet (table 3). A few participants gave examples of erroneous health information that caused anxiety or led to poor personal health choices. Most participants stated that they asked their clinician to verify information they found on the web. Nearly all participants reported that they would trust the accuracy of the content and recommendations made by the IPHR because it was endorsed and used by their clinician, and identified their clinician as their primary authority on the accuracy and application of healthcare information.
Functionality
Functions that the participants identified as important involved two subthemes: enhanced patient–clinician communication and patient-centred utility (table 4).
Representative participant comments on functionality enhanced patient–clinician communication from using an interactive prevention health record (IPHR)
Many participants stated that they wanted PHRs to enhance communication with their clinician both electronically and in person. Several liked being contacted about preventive care after they used the IPHR. Participants described how the IPHR could focus discussions during office visits, making their visits more productive. Conversely, several also mentioned that the IPHR could appropriately broaden discussions for some topics, such as identifying preventive screening choices that they or their clinician viewed as warranting dialogue, or starting conversations about lifestyle changes. However, some participants expressed concern that more time would be required for busy clinicians and patients to use the IPHR or similar tools. Participants worried about increased fees for either patients or practices to use similar PHRs in the future.
Many participants said that a critically important feature of the IPHR was the ability for patients to access their personal health information. They explained that this access was important so that they could be ‘on the same page’ as their clinician. They also commented that shared access to information would contribute to improved accuracy of records and more productive interactions.
Many participants identified the personalised advice offered by the IPHR, its prompts to discuss its recommendations with the clinician (eg, whether to take aspirin), and its ability to prioritise recommendations and thereby highlight critical or information to act on, as very important. Also of interest to many (but not available in this IPHR) were adding features for comprehensive medication reconciliation, in-depth information for the whole family for prevention as well as for specific diseases, and links to local resources that provide support and information for lifestyle changes, preventive care needs and chronic diseases. Moreover, several participants stated that PHRs, such as the IPHR, should be shared seamlessly across all healthcare providers and settings.
Discussion
Given the national investment of $27 billion to promote the adoption, implementation and meaningful use of health information technology,9 ,45 ,46 it is essential to understand how to better engage patients in using technology if it is to achieve its full potential. Many Americans have not embraced the use of PHRs,47 but our findings underscore the general interest of patients in using such tools if certain attributes are offered.
When PHR use is integrated into care so that it improves the efficiency and quality of patients’ care (eg, timely use related to clinician visits), its relevance becomes more transparent. The PHR becomes a welcome extension of interactions with the clinician and the related healthcare team.
National surveys have clearly documented a level of public concern about personal health information existing on the web and about employers, insurers or even commercial entities being able to access or misuse such information.47 Although one could argue that such fears may ease over time as more private information migrates into the cyber-environment, this reticence may have already contributed to the failure of some commercial PHRs to gain wide acceptance by the general public.48
The addition of certain PHR features that seem popular with patients, such as displaying test results or supporting asynchronous communication via secure messaging, has generated only modest increases in actual PHR utilisation.17 ,21 One explanation is that patients who are accustomed to more powerful information tools in other aspects of life may expect greater functionality than merely seeing their information.49 ,50 Indeed, participants in this study wanted much more—including links to personalised recommendations, and resources and tools to help make information actionable to improve health, as provided by this IPHR.
Across the users and the non-users, nearly all participants reported being more likely to perceive a PHR as relevant, trustworthy and functional if it was offered to them by their personal clinician. We conclude that a key element of engaging patients to use a PHR extends beyond the tool's design and includes how it is presented to patients and integrated into their care experience (figure 1).
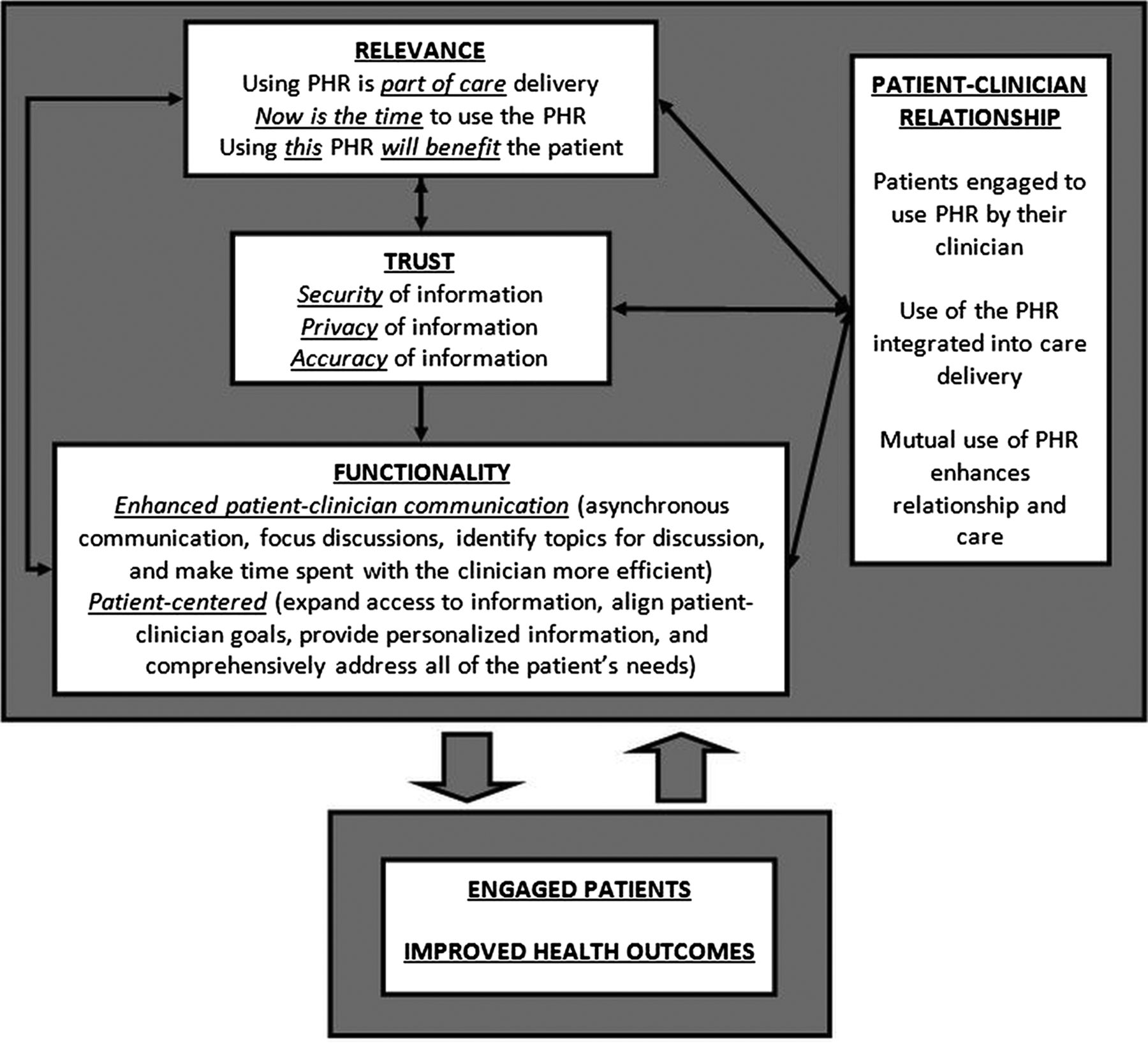
Personal health record features needed to engage patients.
Although some PHR evaluations seem to show enhanced patient uptake when patients had a lack of trust in their clinician,51 ,52 other information seems to indicate that encouragement of PHR uptake by a patient's clinician has a positive influence on patient use and that patient and clinician PHR use enhances their relationship.53 Our findings support Nazi's findings53 and extend them to show, as in figure 1, that the patient–clinician relationship explicitly supports all critical components of patient engagement in the IPHRs.
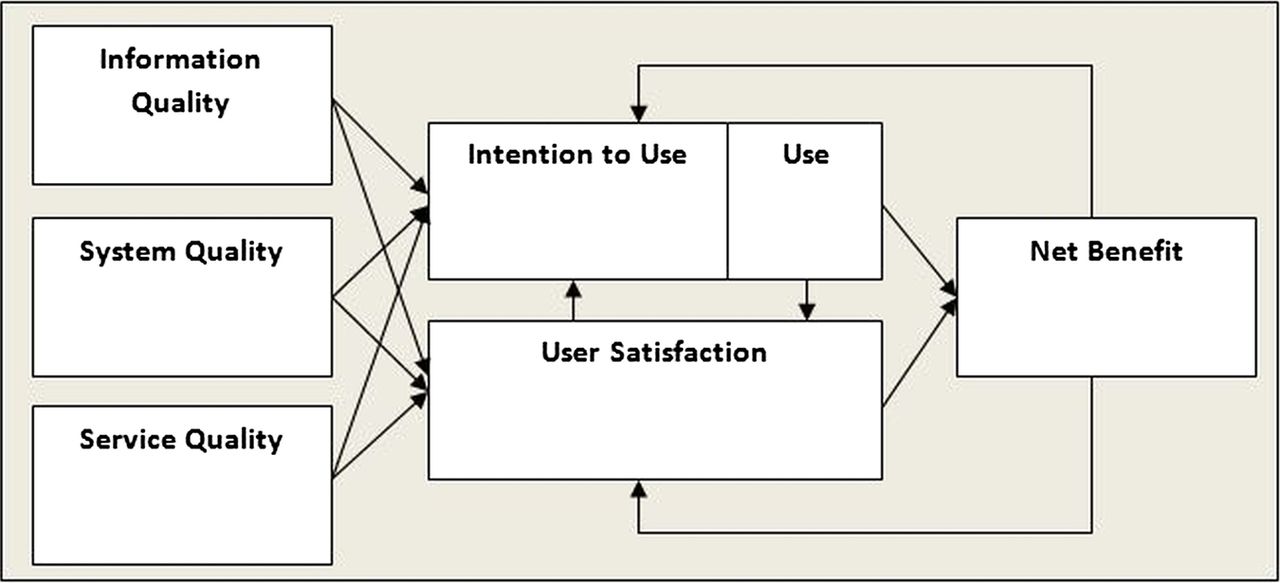
Other models, among them DeLone and McLean's26 MISS (figure 2), have been applied to clinical information systems, including PHRs. Booth states that MISS lacks sensitivities to medical and relationship-laden milieus of technology (previously described by Sandelowski),29 ,54 whereas figure 1 and our results demonstrate clinical as well as personal contexts for patients and clinicians. Further, although Archer et al23 used MISS to categorise aspects of their scoping review of PHRs, they only examined selected parts of the model.

{kind=link}
{kind=link}
Delone and Mclean's model of information system success.26 From William H. Delone and Ephraim R. McLean, “The DeLone and McLean Model of Information Systems Success: A Ten-Year Update,” Journal of Management Information Systems 19(4) (Spring 2003), 24. Copyright © 2003 by M.E. Sharpe, Inc. Reprinted with permission. All Rights Reserved. Not for Reproduction.
Differences between figure 1 and MISS aside, we wish to point out several similarities as well, including the previously mentioned use of causal and process elements, and the feedback loop from ‘Net Benefits’ to ‘Use’ and ‘User Satisfaction’.
Our study has several important limitations. First, while we attempted to assemble focus groups with a representative range of ages and genders, we may have introduced a selection bias in our sample. Participants were older, more likely to be female, mostly white, and more educated than the overall user and non-user populations.55 ,56 However, women are more likely than men to use PHRs57 and to make healthcare decisions for families.57–59 Other studies indicate that members of different socioeconomic and racial-ethnic groups may have different PHR preferences (eg, a PHR not based on the internet) and may require assistance in using a PHR.60–62 Second, the sample was drawn entirely from eight practices in northern Virginia. Other locales may have different PHR needs requiring different strategies to engage patients in PHR use. Third, all participants were recruited from family medicine offices that already offered PHR to patients, and most participants had established relationships with their clinician. Accordingly, participants may have emphasised the value of the patient–clinician relationship in PHR use more than populations from other settings. Finally, whereas the number of participants (28) will not quantitatively generalise to all IPHR users, the nature of qualitative research is often that of looking at specific cases, many times in order to inform the gaps generated by other data, rather than to compete with or duplicate that information.42
Conclusion
To engage primary care patients with an IPHR, this study identifies the importance of relevance, trust and functionality, all integrated with office processes and the patient–clinician relationship. In addition to suggesting possible modifications to established models of technological acceptance, these findings have relevance for healthcare providers, the information technology industry and policymakers who share an interest in encouraging patients to use PHRs or other information tools. Studies like ours should be expanded and replicated in other settings to more fully understand how to make such technology more useful to patients.
Acknowledgments
The authors thank the participating study practices: Fairfax Family Practice, Gainesville Family Medicine, Herndon Family Medicine, Lorton Station Family Medicine, Prince William Family Medicine, South Riding Family Medicine, Town Center Family Medicine, and Vienna Family Medicine. We received invaluable advice and assistance with the focus groups from Christine C Kerns, RN, and in designing the project from Stephen F Rothemich MD, MS as well as Kristin Schmidt in project assistance.
References
Footnotes
-
↵i (Herein ‘clinician’ means physician, nurse practitioner or physician assistant.)
-
↵ii The following is used for the verbal annotation of participant percentages: All=100%, nearly all=80–99%, most=60–80%, many=40–60%, a majority= >50%, some=25–40%, few=<25%.
-
↵iii Unless otherwise indicated, findings described herein are from both the user and the non-user groups.
-
Contributors JWK was involved in design, data acquisition, data analysis/interpretation, drafting/critical revision and final approval. AHK was involved in conceptualisation, design, data analysis/interpretation, critical revision and final approval. DRL was involved in design, data analysis, critical revision and final approval. AJK design, data acquisition, data analysis/interpretation, critical revision and final approval. SHW was involved in conceptualisation, data analysis/interpretation, critical revision and final approval.
-
Funding Agency for Healthcare Research and Quality (R18 HS17046-01).
-
Competing interests Virginia Commonwealth University holds the intellectual property rights to the interactive preventive care record evaluated in this study. Although the university and developers are entitled to the system's revenue, MyPreventiveCare is a non-commercial product, and no revenues have been generated other than grant funding.
-
Ethics approval Institutional Review Board of Virginia Commonwealth University.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Transcripts for the focus groups in this study are not able to be shared due to requirements of our Institutional Review Board.