Article Text

Abstract
Objective To assess if the risk of first-time salpingectomy was affected by prior hysterectomy with retained fallopian tubes and by prior sterilisation.
Design A historical cohort study.
Setting Denmark.
Participants 170 000 randomly selected women born 1947–1963 (10 000/year) were followed from 1977 until the end of 2010.
Main outcome measures Effect of hysterectomy with retained fallopian tubes or sterilisation on the risk of salpingectomy. Both were modelled in a Cox proportional hazards model as time-dependent covariates, analysing time to first salpingectomy. End of follow-up period was 31 December 2010.
Results Of 9591 hysterectomies, 6456 (67.3%) had both fallopian tubes retained. HRs for salpingectomy after hysterectomy with retained fallopian tubes and sterilisation were 2.13 (95% 1.88 to 2.42) and 2.42 (2.21 to 2.64), as compared with those for non-hysterectomised and non-sterilised women.
Conclusions Women undergoing hysterectomy with retained fallopian tubes or sterilisation have at least a doubled risk of subsequent salpingectomy. Removal of the fallopian tubes at hysterectomy should therefore be recommended.
- Gynaecology
- Chort study
- Hysterectomy
- Salpingectomy
- Sterilisation
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Article summary
Article focus
-
Hysterectomy and sterilisation are common gynaecological surgical procedures.
-
The majority of hysterectomies and sterilisations performed are with retained fallopian tubes.
-
Tubal pathology can occur after both procedures.
Key messages
-
Women undergoing hysterectomy or sterilisation have at least a doubled risk of subsequent salpingectomy, compared with women who have not undergone a hysterectomy or a sterilisation.
-
Our findings suggest that removal of the fallopian tubes at a hysterectomy should be recommended.
-
Salpingectomy as a sterilisation procedure should be discussed thoroughly with the patient before deciding on the approach to be adopted for the individual woman.
Strengths and limitations of this study
-
A large national population-based study.
-
170 000 women were included.
-
Potential missing information on relevant procedures at an age younger than 30 years.
-
No information on emigration.
Introduction
Hysterectomy is the most frequently performed gynaecological surgical intervention among women of reproductive age. In Denmark, there are annually approximately 5000 hysterectomies of benign indication. In 2010, the simultaneous removal of the ovaries and the fallopian tubes was performed in 12% of the hysterectomies.1 After hysterectomy, the blood supply of the ovaries is secured via the infundibulopelvic ligament, and the hormone profile is left unaltered by salpingectomy.2–4 No long-term negative effects of salpingectomy at hysterectomy have been reported. The blind-ended remnants of the fallopian tubes may instead give rise to complications such as hydrosalpinx, infection, benign tumours, tube prolapse/torsion, and perhaps induction of ovarian cancer,4–7 the most frequent being hydrosalpinx (35.5%).8 ,9 Hysterectomised women have a 7.8% lifetime risk of subsequent surgery of adnexae.10
Malignant tumours of the fallopian tube are rare. A reconsideration of the ovarian cancer aetiology is ongoing. One hypothesis suggests that serous epithelial carcinomas originating from the distal end of the fallopian tube may be the origin of some ovarian cancers and/or primary peritoneal cancers.11–17
Hydrosalpinx and other tubal pathology with succeeding salpingectomy can also occur after sterilisation, which is the most frequently applied contraceptive method worldwide. United Nations statistics estimate an annual 200 million sterilised women of reproductive age.18 Surgical techniques of sterilisation vary worldwide.19 However, laparoscopic coagulation of the isthmic portion is generally preferred. In Denmark, ligation with clips is the most frequently used technique20 whereby the fimbriated end of the fallopian tube is left unaffected. This implies a risk of subsequent pathology in the tubes.
Our hypothesis is that there is a potential risk for a second major surgery after both hysterectomy and sterilisation with retained fallopian tubes.
The aim of our study was to assess the effect of hysterectomy with retained fallopian tubes, and sterilisation on the risk of first-time salpingectomy in order to provide an improved empirical basis for deciding whether the fallopian tubes should be removed routinely at a hysterectomy (on benign indication).
Methods
Study population
From the Danish Civil Registration System, we randomly selected 10 000 women born each year from 1947 to 1963 who were alive on January 1 of the year in which they turned 40 years. Thereby, the included women were between 15 and 30 years of age at the start of the observation period (1 January 1977), and had a follow-up to at least the age of 47 years (end of follow-up was 31 December 2010). Occurrences of surgical codes for hysterectomy, salpingectomy, oophorectomy or combinations of these were retrieved from the Danish National Patient Registry (established in 1977)21 for each of these 170 000 women. Procedural codes are given in table 1.
Number of included surgical procedures in the Danish National Patient Registry from 1 January 1977 to 31 December 2010 among the included 170 000 women
Statistical analyses
The cause-specific hazard of time to the first salpingectomy was modelled by a Cox proportional hazards approach, including time-dependent hysterectomy and sterilisation status and birth cohort as categorical covariates (1947–51, 1952–56 and 1957–63).22 HRs were presented with 95% CIs.
The various hysterectomy types and techniques are included in the same model since they all, despite their heterogeneity, contain the possibility of retaining the fallopian tubes, and thereby potentially enhance the risk of tubal pathology.
To illustrate the time aspect of potential salpingectomy after hysterectomy, the cumulative incidence curves for salpingectomy were estimated for the three included birth cohorts.
Results
We identified 9591 hysterectomies during the study period of which 6456 (67.3%) had retained fallopian tubes. Sterilisation was performed in 9829 women, and 7167 had a salpingectomy (table 1).
The cohort-adjusted HRs for salpingectomy after hysterectomy with retained fallopian tubes and after sterilisation were 2.13 (95% CI 1.88 to 2.42) and 2.42 (2.21 to 2.64), as compared with those for non-hysterectomised and non-sterilised women (table 2). Hysterectomy as well as sterilisation thus increased the risk for a subsequent salpingectomy.
Estimated effect (HRs) of hysterectomy with retained fallopian tubes, sterilisation and birth cohorts on the risk of first-time salpingectomy
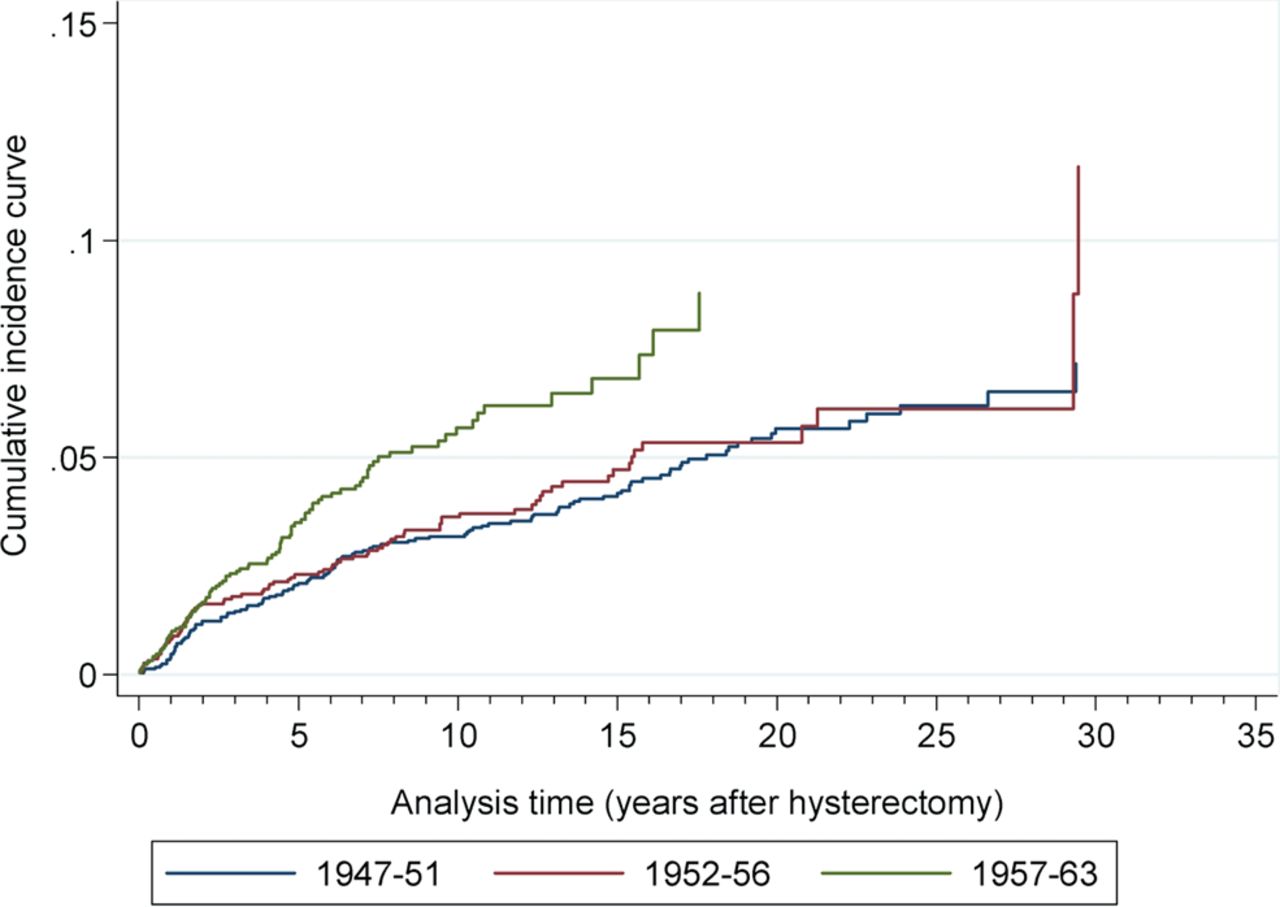
Figure 1 shows the cumulative incidence curve by cohort for salpingectomy after hysterectomy. The cumulative incidence was highest for the youngest cohort.

{kind=link}
Cumulative incidence curves for first-time salpingectomy after hysterectomy by cohort, based on N=6456 hysterectomies.
Five and 10 years after hysterectomy, the numbers of first-time salpingectomy, death or end of follow-up are presented in table 3. There were increasing numbers of salpingectomies after hysterectomy with succeeding birth cohorts, with the youngest women having the highest proportion of salpingectomies after hysterectomy. In absolute terms, after 10 years, 85/2172=3.9% women were salpingectomised. For all three cohorts, about two-thirds of salpingectomies were performed within 5 years after hysterectomy.
Numbers and percentages of first-time salpingectomy, death and end of follow-up, whatever came first after hysterectomy in three consecutive birth cohorts
Discussion
Principal findings
Women undergoing hysterectomy with retained fallopian tubes or sterilisation had at least a doubled risk of succeeding salpingectomy in our study as compared with women without these surgeries.
To the best of our knowledge, no previous study has investigated this on a national level. Small cohort studies (n=38, 82 and 337, respectively) have described that retained fallopian tubes may give rise to tubal pathology.8–10
The cumulative incidence of salpingectomy after hysterectomy with retained fallopian tubes increased in the latest cohort. This can be explained by the development and introduction of ultrasound examinations which increase the chance of detecting pathological tubes. The clinical significance of leaving ‘orphan’ ovaries is unknown. Salpingectomy may cause early cystic degeneration of the remaining ovaries,9 which is of unknown significance. The hormone production is not altered after salpingectomy.2–4 We believe that a salpingectomy, carefully and properly carried out at the same time as a hysterectomy, is not associated with any risk of disturbed ovarian function. To leave the ovaries undisturbed, salpingectomy should be performed with ligation/diathermy of the three major vessels from the ovarian pedicle to the fallopian tube, as far away from the ovary as possible.
Age at menopause could be another issue, but we found no study on the influence of removal of the fallopian tube concomitantly with hysterectomy on age at menopause. The time aspect of an extended operation owing to concomitant salpingectomy is negligible. We could not extract any data indicating disadvantages associated with removal of the fallopian tubes at the same time as a hysterectomy. Salpingectomy as a sterilisation procedure, however, excludes the possibility of later refertilisation by surgical reanastomosis (although the in vitro fertilisation would nowadays be the standard treatment instead of reanastomosis). The decision of conventional sterilisation or salpingectomy should, therefore, be discussed individually with each woman. The information to these women should emphasise the risk of regret, complications to surgery and the potential risk of health hazards with retained fallopian tubes.
The Danish National Patient Registry is a valuable source of data. It records 99.4% of all discharges from hospitals in Denmark, and the surgical procedures for hysterectomy have been validated and show a high quality of the data with positive predictive values of 90–99%.23 ,24
Limitations
For women entering the study at an age close to 30 years, there is potential missing information on relevant procedures at a younger age. The need for hysterectomy before the age of 30 is, however, low. No information on emigration was included in the analysis.
The current study has not been focusing on the development of gynaecological cancer after hysterectomy or sterilisation. The follow-up was to a maximum age of 63, and therefore we had insufficient power for assessing the risk of tubal or ovarian cancer.
Risk-reducing surgical intervention
Prophylactic removal of the fallopian tubes during hysterectomy or even sterilisation would rule out any subsequent tubal pathology and succeeding salpingectomy. This is further tempting with the hypothesis that pelvic or ovarian serous carcinomas may originate from the fallopian tubes.14 Recommendations of prophylactic salpingectomy during hysterectomy or tubal ligation have been published.25–27 These recommendations are in line with our findings.
Other ways of risk-reducing surgical interventions have been discussed in the literature
-
Bilateral salpingectomy with ovarian retention as a potential temporary, short-term intermediate step towards bilateral oophorectomy in younger BRCA1/2 mutation carriers not yet prepared to undergo premature menopause after risk-reducing salpingo-oophorectomy.28
-
Removing the fallopian tubes at the time of a caesarean section in women during their last delivery,29 though these latter risk-reducing surgical interventions lack research data before an evidence-based decision can be made.
Conclusions
We found that women undergoing hysterectomy or sterilisation with retained fallopian tubes had at least a doubled risk of succeeding salpingectomy. Therefore, removal of the fallopian tubes at a hysterectomy should be recommended. Salpingectomy as a sterilisation procedure should be discussed thoroughly with the patient before deciding on the approach to be adopted.
References
Footnotes
-
Contributors RG, SW, CWS, OM and ØL have drafted the article, revised it critically for important intellectual content and approved the final version to be published. All authors are responsible for the study concept and design, and participated in the interpretation of data. SW led the statistical analysis. RG is the guarantor and had full access to all of the data in the study.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests ØL has been an expert witness for the plaintiff in a legal US case in 2011 and 2012 on hormonal contraception and venous thrombosis.
-
Ethics approval The study was approved by the Danish Data Detection Agency (no. 2010–41–4804). According to Danish law, a review by an ethic board or patient consent is not required for purely register-based studies.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement According to the Danish Data Detection Agency, we are not allowed to share our data from the Danish National Patient Registry. This would require special approval from both the Danish Data Detection Agency and the Statens Serum Institut which deliver the data from the Danish National Patient Registry.