Article Text

Abstract
Objective Low socioeconomic position is a known health risk. Our study aims to evaluate the association between socioeconomic position (SEP) and lower limb amputations among persons with diabetes mellitus.
Design Population-based register study.
Setting Finland, nationwide individual-level data.
Participants All persons in Finland with any record of diabetes in the national health and population registers from 1991 to 2007 (FinDM II database).
Methods Three outcome indicators were measured: the incidence of first major amputation, the ratio of first minor/major amputations and the 2-year survival with preserved leg after the first minor amputation. SEP was measured using income fifths. The data were analysed using Poisson and Cox regression as well as age-standardised ratios.
Results The risk ratio of the first major amputation in the lowest SEP group was 2.16 (95% CI 1.95 to 2.38) times higher than the risk in the highest SEP group (p<0.001). The incidence of first major amputation decreased by more than 50% in all SEP groups from 1993 to 2007, but there was a stronger relative decrease in the highest compared with the lowest SEP group (p=0.0053). Likewise, a clear gradient was detected in the ratio of first minor/major amputations: the higher the SEP group, the higher the ratio. After the first minor amputation, the 2-year and 10-year amputation-free survival rates were 55.8% and 9.3% in the lowest and 78.9% and 32.3% in the highest SEP group, respectively.
Conclusions According to all indicators used, lower SEP was associated with worse outcomes in the population with diabetes. Greater attention should be paid to prevention of diabetes complications, adherence to treatment guidelines and access to the established pathways for early expert assessment when diabetic complications arise, with a special attention to patients from lower SEP groups.
- Preventive Medicine
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Article summary
Article focus
-
Previous studies have shown a low-socioeconomic position (SEP) to be associated with increased health risks. In recent years, declining amputation incidences among diabetic persons have been reported, but there is still a wide difference in amputation rates between countries and populations. Studies on the relationship of an individual’s SEP and amputation risk among patients with diabetes are relatively scarce. Our study aims to evaluate the association between (SEP) and lower limb amputations among persons with diabetes mellitus.
Key messages
-
Our results indicate that low SEP is associated with an increased risk of the first major amputation among persons with diabetes in Finland. The incidence of first major amputation decreased significantly by increasing income. Furthermore, the 2-year amputation-free survival rate after the first minor amputation was significantly higher in the highest SEP group when compared with the lower SEP groups. A similar association was also seen between income and the ratio of first minor/major amputations.
Strengths and limitations of this study
-
We were able to use nationwide data collected from comprehensive administrative registers and link registers using identity codes. The data allowed us to examine the total population of Finnish residents treated for diabetes. We were also able to use individual register data on the SEP. On the downside, the national registries do not contain information on life style or health-related risk factors and some persons with diet-controlled diabetes who do not use any hypoglycaemic medication or have no hospital visits with diabetes diagnosis are missing from the data.
Introduction
Poverty, poor education, low-occupational status as well as a poor-labour market situation have repeatedly been shown to constitute health risks.1 Several studies have shown a low-socioeconomic position (SEP) to be associated with an increased risk of stroke at a younger age,2 ,3 high mortality due to coronary heart disease4 and high case-death after the first cardiac event.5
A major amputation is a devastating complication of diabetes mellitus. In recent years, declining amputation incidences among diabetic persons have been reported,6 ,7 but there is still a wide difference in amputation rates between countries and populations.8–11 Studies on the relationship of an individual’s SEP and amputation risk are scarce, especially among diabetic patients. In Australia, Bergen et al12 have reported differences among persons with diabetes from deprived and non-deprived areas in diabetic ulcers, but not in amputation rates. In three other studies, the association between low SEP and high-amputation rate was reported in patients with critical limb ischaemia.13–15
The aim of the current study was to evaluate the relationship of lower limb amputation and SEP among diabetic individuals in Finland using three outcome indicators: the incidence of first major amputation, the ratio of first minor/major amputation and the 2-year survival rate with preserved leg after the first minor amputation.
Material and methods
Our study utilised the FinDM II database,16 which comprises data on all diabetic individuals in Finland with any record of diabetes in the national healthcare and insurance registers for 1991–2007. The database was used to identify diabetic individuals and to follow-up on their amputations and deaths. Sociodemographic data were obtained from the longitudinal employment statistics database of Statistics Finland. The record linkages between and within the registers were carried out using the individual personal identity codes applied in all administrative registers in Finland.
Two criteria were applied to identify patients with a diabetes mellitus diagnosis: a person was on hypoglycaemic medication according to the national health insurance files or he/she had been hospitalised for diabetes according to the National Hospital Discharge Register. The use of hypoglycaemic medication is recorded in two National Health Insurance registers maintained by the Social Insurance Institution—the register on entitlements for special (elevated) health insurance reimbursement for hypoglycaemic medication (data from 1964 to 2007) and the register on reimbursed medication purchases (data 1994–2007) coded with the Anatomic Therapeutic Chemical classification system code A10. Hospital admissions in Finland are recorded in the National Hospital Discharge Register (data for 1969–2007) using the International Classification of Diseases (ICD) codes (www.who.int/classifications/icd/en). Diabetes is registered with the ICD-8–9 code 250 and ICD-10 codes E10–14. The high health insurance reimbursement level for hypoglycaemic medication has resulted in a comprehensive coverage of individuals with diabetes in the medication registers. The Hospital Discharge Register is also comprehensive and covers both public and private hospitals. All hospitals in Finland have a legal obligation to report all hospital discharges. Up until 2008, mortality among individuals with diabetes was monitored in the Causes of Death Register of Statistics Finland.
In the present study, those who were not permanent residents of Finland or had gestational diabetes only were excluded from the analyses. A comparison against a local diabetes register of the Helsinki metropolitan area has demonstrated good coverage of diabetic patients in the nationwide register.17 A more comprehensive description of the study population is available elsewhere.16
In 1993, the number of persons with diabetes was 130 244 (26 049/SEP group), and it increased to 274 388 (54 878/SEP group) by 2007.
Amputations
After identifying all persons treated for diabetes in the country, the data were cross-linked with the National Hospital Discharge Register using the personal identity codes to identify which patients had sustained a lower extremity amputation (LEA) (NOMESCO procedure codes NFQ20, NGQ10, NGQ20, NHQ10, NHQ20, NHQ30 and NHQ40 or Finnish Hospital League procedure codes 9571, 9572, 9573, 9574 and 9575) from 1987 to 2007. All amputations above the ankle were considered major and those below the ankle minor (codes NHQ20, NHQ30, NHQ40, 9571 and 9572). We excluded amputations due to neoplasm or trauma (with the exception of those with the ICD-10 codes S90–91, T80–81 and T87.3–T87.6).
Socioeconomic position
We used income as an indicator of SEP. The net household income was obtained from tax records included in the annual employment statistics databases compiled from several administrative registers by Statistics Finland. The annual incomes of persons with diabetes were classified into quintiles adjusted for family size using the OECD equivalence scale.18 The analyses were also performed using register data concerning educational attainment, that is, basic (up to 9 years), intermediate (10–12 years) and higher (13 or more years) education as an indicator of SEP.
Statistical methods
The first major amputations (preceding a 10-year amputation-free period) among persons with diabetes were identified and stratified according to age group, sex, type of diabetes, duration of diabetes and year of amputation. The adjusted impact of these variables on the incidence of first major amputation was analysed using the Poisson regression model.
The minor/major amputation ratios were calculated by dividing the number of all first amputations classified as minor by those classified as major. Ratios were calculated for each SEP group using a 3-year time window (moving) over the follow-up period.
Survival analyses were used to study the time elapsed from the first minor amputation to death or major amputation. Unadjusted survival with preserved leg was studied using the Kaplan-Meier product-limit estimator, and the adjusted effect of SEP was analysed using the Cox proportional hazards model. The result was considered censored at the final day of 2008 if no event of interest had occurred before that.
All statistical analyses were performed using the R software package with the library Muste (www.survo.fi/muste).
The study protocol was approved by the Institutional Ethics Committee of National Institute for Health and Welfare (§367/2011), and the permissions to use register data were applied from the National Institute for Health and Welfare, Statistics Finland and Social Insurance Institution. Informed consents were not required since the data were anonymous register data and the people were not contacted.
Results
First major amputation
In 1993, the crude incidence of first major amputations per 100 000 person-years among persons with diabetes (pyrs) was 420 (95% CI 386 to 456). The incidence decreased steadily during the study period, being 154 (95% CI 139 to 169) in 2007. In 1993, the crude incidence was roughly 600 in the lowest SEP group and 200 in the highest. The incidence decreased significantly in all SEP groups during the study period, being 260 in the lowest and 60 in the highest SEP group in 2007 (figure 1). In the Poisson regression model adjusted for age, sex, type of diabetes, year and diabetes duration, higher income was associated with a decreased risk of first major amputation (p<0.001; table 1). In the highest income group, the relative risk was 0.46 in comparison to the lowest income group. In the highest educational group, the relative risk was 0.54 (95% CI 0.49 to 0.60, p<0.001) compared with the group with basic education only.
Risk factors for first major amputation* among persons with diabetes in Finland in 1991–2007 (Poisson regression model)

The crude incidence of the first major amputation among diabetic persons by income quintile in Finland from 1993 to 2007.
Ratio of first minor/major amputations
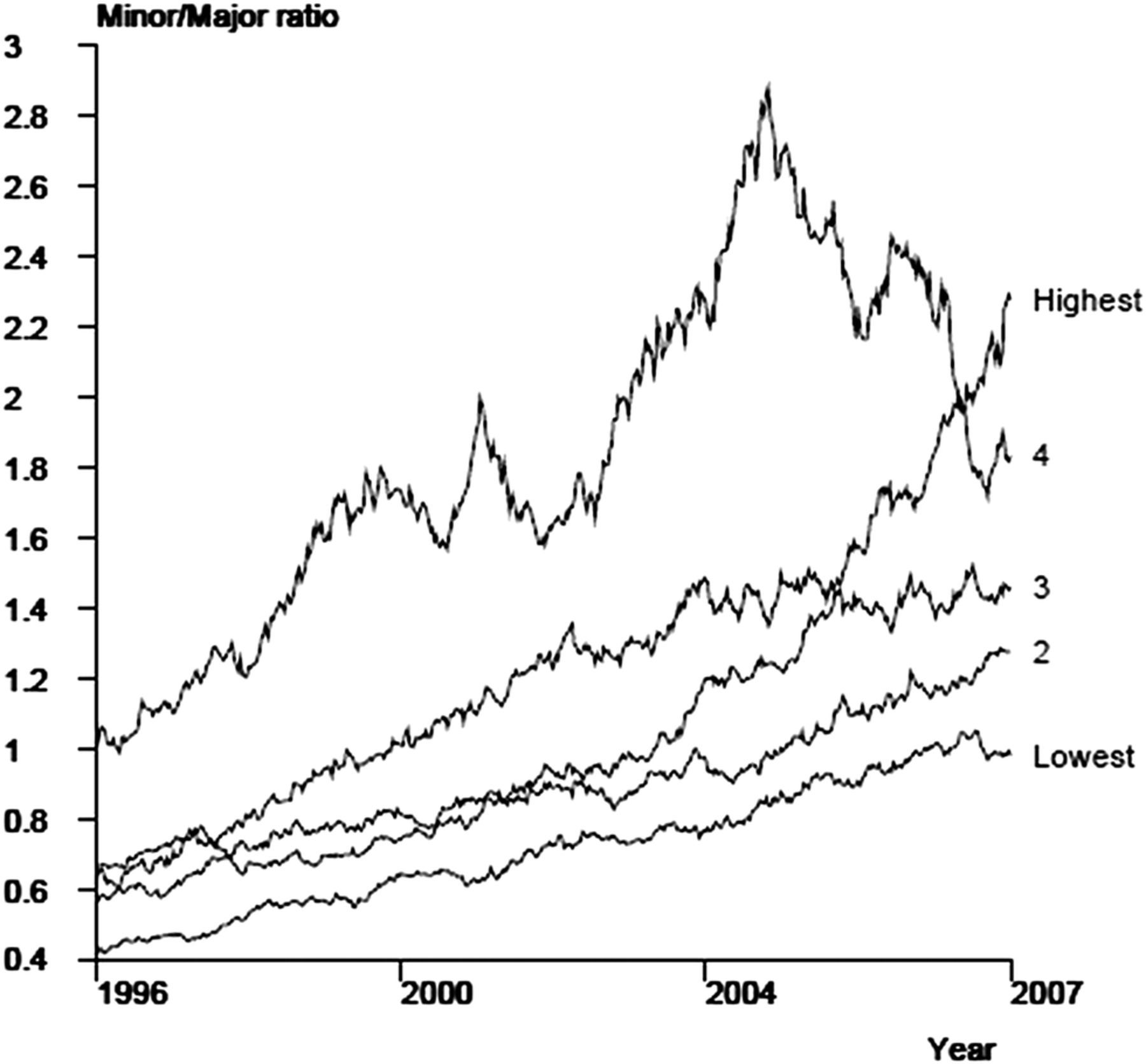
During the study period, the ratio of first minor/major amputations increased steadily. A gradient was detected by income: the higher the income group, the higher the ratio. This gradient persisted throughout the study period. Furthermore, the differences were remarkably large between the highest income group and other groups (figure 2). A similar pattern was detected for education: the group with basic education only was clearly different from the groups with intermediate and highest (data not shown).

The ratio of minor and major amputations among diabetic persons by income group in Finland in 1993–2007 (calculated by sliding a 3-year-wide observation window over the follow-up period).
Two-year survival with preserved leg after the first minor amputation
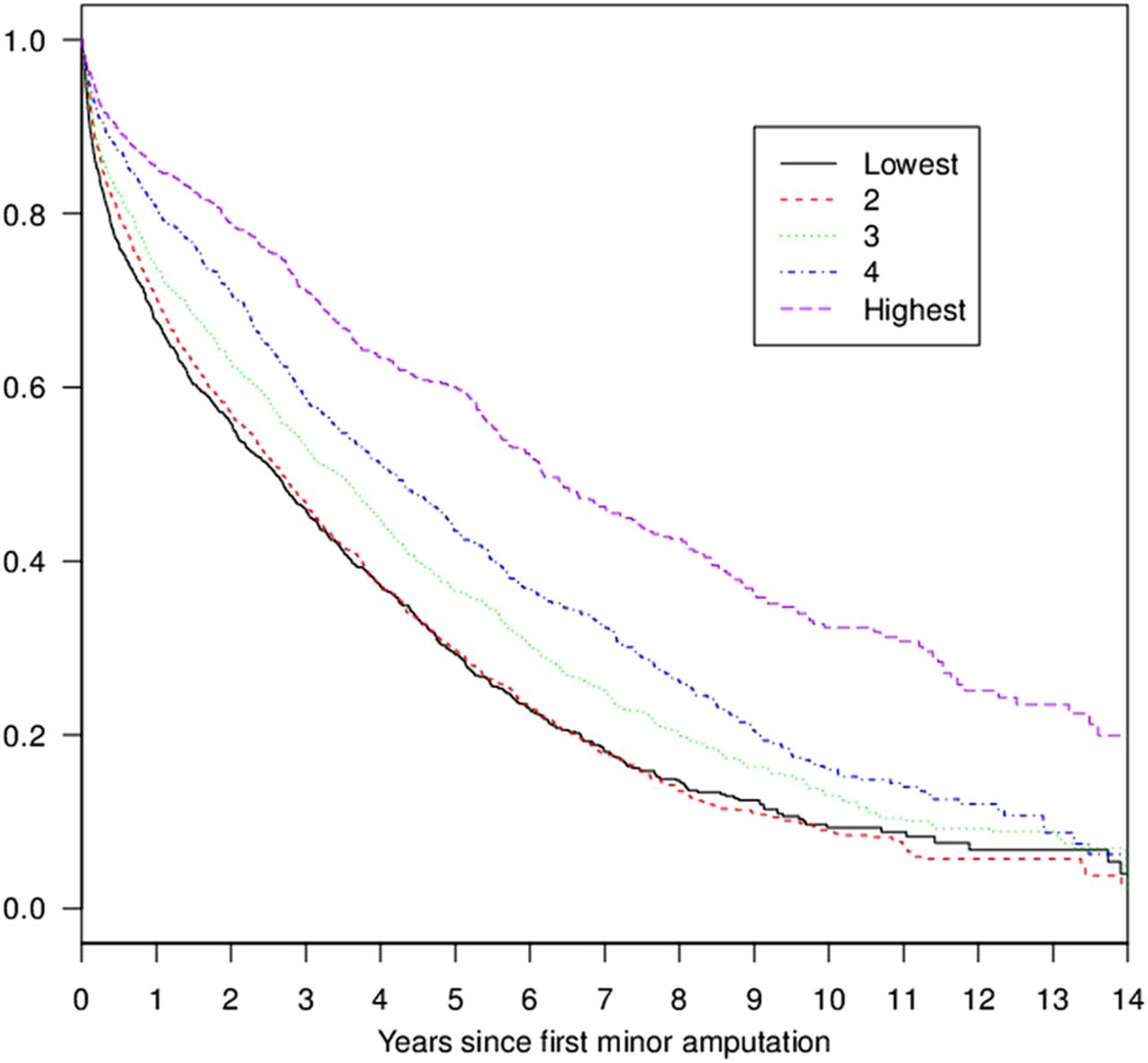
The 2-year amputation-free survival after the first minor amputation was 55.8% in the lowest SEP group and 78.9% in the highest SEP group. The 10-year amputation-free survival percentages were 9.3 and 32.3, respectively (figure 3). In the Cox regression model with 2-year follow-up adjusted for age, sex, diabetes duration, year and diabetes type, higher income was associated with lower risk of death and/or major amputation after the first minor amputation. While the differences between the three lowest income groups were not statistically significant, the amputation-free survival was significantly higher in the two highest income groups when compared with the lowest income group (table 2). For education, the differences were statistically significant: in the group with the highest education, the relative risk was 0.71 (95% CI 0.62 to 0.80, p<0.001) compared with the group with only basic education.
Risk factors for major amputation and/or death during 2 years after first minor amputation among persons with diabetes in Finland in 1991–2007 (Cox regression model)
{kind=link}
{kind=link}
{kind=link}
Unadjusted amputation-free survival with the leg intact/preserved after first minor amputation among diabetic persons by income group in Finland from 1993 to 2007 (Kaplan-Meier product-limit estimator).
Discussion
Principal findings
Our results indicate that low SEP is associated with an increased risk of the first major amputation among persons with diabetes in Finland. The incidence of first major amputation decreased significantly by increasing income. Furthermore, the 2-year amputation-free survival rate after the first minor amputation was significantly higher in the highest SEP group when compared with the lower SEP groups. A similar association was also seen between income and the ratio of first minor/major amputations. Thus, our results are in line with other studies suggesting an increased amputation risk in patients with critical limb ischaemia in the low-SEP population.12–15
Strengths and weaknesses of the study
The main weakness of our study is that with our register-based data, we were not able to control for some important clinical or life-style or health-related factors, such as body mass index or smoking, that are likely to affect the outcome. However, the major strength is that we were able to use nationwide data collected from comprehensive administrative registers. It is known, for instance, that the validity of the Finnish Hospital Discharge Register is high and that the Finnish Causes of Death statistics are valid and reliable by international standards.19 ,20 The data allowed us to examine the total population of Finnish residents treated for diabetes although our data are likely to miss some persons with diet-controlled diabetes mellitus who are not using any hypoglycaemic medication or do not have any hospital visits with diabetes diagnosis. We were also able to use individual register data on the SEP. The socioeconomic data used in the study were based on longitudinal data files containing information from tax registers and from several registers maintained by Statistics Finland. Data on the vascular surgical procedures on the lower extremity did not include all the endovascular procedures in the used registers, which made it impossible to examine how much of the differences in outcomes could have been explained by limited access to vascular surgery in the lower SEP groups.
Strengths and weaknesses in relation to other studies, discussing particularly any differences in results
The crude incidence of the first major lower limb amputations in Finland seems to be somewhat higher than in some other countries.7 ,10 For example, the crude incidences were 1.54 (per 1000 of diabetes population) and 7.98 (per 100 000 of general population) in Finland in 2007, while the corresponding incidences were reported to be 1.26 and 4.43 in Scotland.7 Such comparisons of crude incidences are not without problems. Population structures may be different, and the use of denominator including all age groups may be misleading as most amputations are performed for older persons. Furthermore, calculation of crude incidences and standardised incidences as reported in our earlier study6 provides different figures from the same data. Therefore, when incidence figures are concerned, the rates are comparable only within one study, while the relative comparisons are much more suitable for benchmarking purposes. Differences in incidences between populations could be related to prevention measures, access to care, treatment decisions and options available for reconstructive vascular surgery. This interpretation is supported by the reported regional differences of amputation rates observed in some countries.10 ,11
In the USA, several studies have shown that African-American patients undergo a major lower extremity amputation two to three times more frequently than Caucasian patients.21 ,22 An explanation suggested by Feinglass et al22 is SEP differences between ethnic groups. A cross-sectional study including 20% of all non-federal hospital discharges in the USA13 found that a primary amputation was performed with a higher frequency on patients with lower extremity ischaemia who were non-white, had a low income and were not covered by private insurance. A delayed diagnosis of peripheral arterial disease (PAD), a lack of access to adequate primary care or vascular surgery, or both, as well as cultural distrust may explain these findings.13 Some studies from the USA have also found large regional differences in LEAs among Medicare recipients with and without diabetes11 ,23 even after controlling for patient characteristics including sex, age and ethnic background. The authors suggest that these variations could be related to treatment practices, access to and use of preventive care among patients, and health-based education of the patients and their treatment preferences.
Meaning of the study: possible mechanisms and implications for clinicians or policymakers
A major amputation is an end stage of a progressive disease, while almost all patients with diabetes who undergo an amputation have developed neuropathy and PAD, and many of them also suffer from infections and renal insufficiency.24 Comprehensive diabetes care, however, probably slows down the progress of the disease and reduces the risk of major amputations. Our results suggest that the long-term treatment of diabetes may have been less successful among lower SEP groups over the years. Low SEP has been reported to be a risk factor for poor glycaemic control in young persons with type 1 diabetes.25 ,26 The prevalence of risk factors can differ between different socioeconomic groups. In Finland, for example, smoking is more common among lower SEP groups.27 ,28 Smoking is a very strong risk factor of PAD.29 During the period 2000–2004, about 38% of adult Finnish men with lowest education were smokers compared with 17% with the highest education smoked in Finland.28 The corresponding figures for women were 28% and 13%. Smoking persons with diabetes have more proximal amputations.30 Part of the explanation to differences in outcomes is likely to be worse hyperglycaemia and higher prevalence of smoking in the lower SEP groups.
In Finland, like in many industrialised countries, equal access to healthcare according to need has been an important goal for health policy for decades. All residents in Finland have access to primary and secondary healthcare, independent of their SEP, when attention to a health problem is needed.31 The municipalities have the main responsibility of provision of healthcare for the residents. Ambulatory and hospital services are primarily provided by the public sector and are mainly financed through taxation and user fees are low, but there have been problems in long waiting times. For employees, occupational healthcare provides easy and free of charge access to ambulatory care. In urban areas, private ambulatory services are available, but for patients deductibles are high (over 60% on average). However, care for patients with diabetic complications, as well as peripheral vascular surgery and limb amputations, is almost exclusively provided by the public healthcare system. In addition to sluggish access to public ambulatory services, the Finnish healthcare system has been slow to adopt active methods of improving treatment for patients with chronic conditions.32 Disease registers, call–recall systems and outreach services, which are uncommon in Finland, could help to improve continuity of personal care among disadvantaged patients with complicated diabetes. Timely and adequate healthcare could ameliorate the potential long-term adverse consequences of SEP differences, as a recent study in Finland suggested while showing that SEP is not associated with the effectiveness of lifestyle interventions in persons with a high risk for diabetes.33
The association between SEP and the ratio of first minor/major amputations was clear in our study. This indicates that major amputations are performed more often as the first amputation in lower SEP groups, whereas the number of minor amputations is relatively higher in higher SEP groups. The factors that influence the level of amputation are the size and location of the lesion in the foot, the patient's ambulatory status and the blood supply to the foot.34 The goal of vascular surgery is to avoid major amputations and to improve circulation to enable wound healing. Indeed, an inverse correlation between the rate of distal bypass operations and amputation incidence has been established.35 ,36 However, if the tissue lesion in a foot is extremely large or there is a widespread infection, major amputation may be the first choice. The results by Henry et al14 suggest an inverse association between SEP and lower extremity revascularisation rates in patients with critical limb ischaemia. Unfortunately, our register did not include revascularisation data.
The 2-year amputation-free survival rate after the first minor amputation was significantly lower in the lower SEP groups as compared with the higher SEP groups. This result seems to suggest inequities in the care of these patients even after their limb-threatening situation has been identified by healthcare professionals. Since all of these patients have undergone their first minor amputation, their treatment schema should have been similar after the beginning of the follow-up. All of these patients have been in contact with healthcare due to the amputation and should have undergone an assessment of blood supply to the foot. Furthermore, they should all have had equal follow-up after the minor amputation. Yet, patients with low income are more likely to die or undergo a subsequent major amputation.
In the current study, the classification of SEP was based on family income. We also carried out our analyses using education as an indicator of SEP, and the main results remained the same. Persons with a higher education had a significantly lower incidence of first major amputations, a higher minor/major amputation ratio and a better 2-year amputation-free survival rate than those with basic education only.
Conclusion
Our results suggest that SEP is associated with a risk of amputation in patients with diabetes. Those in a lower SEP are more likely to sustain amputations, and their amputations are more likely to be major amputations, leading to more severe disability. Low SEP also increases the risk of death and/or major amputation after the first minor amputation. More attention needs to be paid to addressing the risk factors for diabetic complications and life style, especially among patients from lower socioeconomic groups, during all contacts with healthcare from the early stages of diabetes to vascular treatment and rehabilitation.
References
Footnotes
-
Contributors MV, KM, IK, KW, TI and RS conceived the idea of the study. RS and IK were responsible for the design of the study. RS, KM and MV were responsible for undertaking the data analysis and produced the tables and graphs. IK and KW provided input into the data analysis. The initial draft of the manuscript was prepared by MV and KM and then circulated repeatedly among all authors for critical revision. TI made the major revisions. RS was responsible for the acquisition of the data and MV, KM, IK, TI and KW contributed to the interpretation of the results. All authors read and approved the final manuscript.
-
Funding The study was financially supported by the Social Insurance Institution, but the SII had no involvement in its design, data collection, findings or decision to publish.
-
Competing interests All authors included on the paper fulfil the criteria or authorship. An authorship statement form is attached to the submission.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.