Article Text

Abstract
Objectives It remains to be determined whether the benefits of botulinum toxin type A (BoNT-A) on cervical dystonia (CD) motor symptoms extend to improvements in patient's quality of life (QoL). This analysis of a large, multicentre study was conducted with the aim of investigating changes in QoL and functioning among de novo patients receiving 500 U BoNT-A (abobotulinumtoxinA; Dysport) for the treatment of the two most frequent forms of CD, predominantly torticollis and laterocollis.
Design A prospective, open-label study of Dysport (500 U; Ipsen Biopharm Ltd) administered according to a defined intramuscular injection algorithm.
Setting German and Austrian outpatient clinics.
Participants 516 male and female patients (aged ≥18 years) with de novo CD. The majority of patients had torticollis (78.1%). 35 patients had concomitant depression (MedDRA-defined).
Main outcome measures Change from baseline to weeks 4 and 12 in Craniocervical Dystonia Questionnaire (CDQ-24) total and subscale scores, patient diary items (‘day-to-day capacities and activities’, ‘pain’ and ‘duration of pain’) and global assessment of pain.
Results Significant improvements were observed in CDQ-24 total and subscale scores at week 4 and were sustained up to week 12 (p<0.001). Changes in CDQ-24 scores did not significantly differ between the torticollis and laterocollis groups or between patients with or without depression. There were also significant reductions in patient diary item scores for activities of daily living, pain and pain duration at weeks 4 and 12 (p<0.001). Pain relief (less or no pain) was reported by 66% and 74.1% of patients at weeks 4 and 12, respectively. Changes in pain parameters demonstrated a positive relationship with change in Tsui score.
Conclusions After standardised open-label treatment with Dysport 500 U, improvements in QoL and pain intensity up to 12 weeks in patients with CD were observed.
- Rehabilitation medicine
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Article summary
Article focus
-
To test the hypothesis whether a modification of clinical symptoms is correlated to quality-of-life (QoL) parameters after treatment with botulinum toxin type A.
-
Investigation of the QoL and pain reduction benefits of Dysport when administered for the de novo management of torticollis and laterocollis in a large cervical dystonia (CD) patient population.
Key messages
-
Dysport 500 U significantly improves QoL, as rated by CDQ-24, in de novo patients with heterogeneous forms of CD.
-
Dysport 500 U treatment results in significant reductions in pain (on several outcome measures) in de novo patients with heterogeneous forms of CD.
Strengths and limitations of this study
-
This is the largest prospective, open-label cohort study of QoL in CD patients to date.
-
This study reflects the short-term effects of Dysport arising from a single 500 U administration; therefore, long-term studies are required to determine whether the observed beneficial effects on symptoms and QoL can be sustained with repeated treatment.
Introduction
Cervical dystonia (CD), the most frequent form of focal dystonia, may present as idiopathic or secondary disease.1 Idiopathic CDs are characterised by abnormal, involuntary muscle contractions, resulting in abnormal head movements and various undesired positions of the head.2 The disorder is commonly classified as a function of the direction of abnormal head position—torticollis (turning of the head), laterocollis (head tilt), retrocollis (neck extension), antecollis (flexion) or, most frequently, a combination of the above.3 Increased involuntary activity in affected muscles frequently leads to hypertrophy, and resulting symptoms include pain in the region of the neck and shoulder, decreased range of motion and impairment of voluntary movement of the head. Reduction of muscle activity with local botulinum toxin type A (BoNT-A) injections is recommended as the first-line treatment option for CD.4 The efficacy and tolerability of abobotulinumtoxinA (Dysport, Ipsen Biopharm Ltd, Wrexham, UK) and other BoNT-A preparations for the treatment of CD have been demonstrated in randomised, placebo-controlled trials and open-label extension studies, with symptom relief being sustained for up to 3 months or four treatment cycles, respectively.4–8
Clinical symptoms of CD (eg, neck pain) cause significant disability that interferes with patients’ daily functioning, such as the ability to remain in employment.9 Moreover, a significant negative impact on quality of life (QoL) is seen with CD and is comparable to that seen with other serious disabling illnesses, such as multiple sclerosis, Parkinson’s disease and stroke.10 In a study of 289 patients with CD from seven European countries, concomitant depression was identified as one of the two strongest predictors of poor QoL (alongside anxiety), in addition to response to botulinum toxin, self-deprecation, stigma and other patient-related factors.11 Successful treatment of motor symptoms by existing treatments does not necessarily entail a positive influence on patient QoL.12 It is, therefore, important to analyse whether clinically effective treatment of the movement disorder also leads to improvements in social and emotional well-being for patients and a positive impact on their daily functions and activities.
A large, prospective, open, multicentre study was conducted to evaluate the effectiveness and safety of a single dose of Dysport (500 U) for the treatment of the two most frequent forms of CD.13 Treatment was given according to a standardised algorithm based on the two most frequent forms of CD, predominantly torticollis and laterocollis. Evaluated over 12 weeks, CD symptom severity was assessed using an established scale (the Tsui scale), with the patient in a standardised seated position.14 Results from the study showed that Dysport was effective and well tolerated for the de novo management of a range of heterogeneous forms of CD, when using a standardised regimen that allows tailored dosing based on individual symptom assessment.13 QoL parameters were assessed as secondary objectives throughout the study using a patient-disease questionnaire (Craniocervical Dystonia Questionnaire; CDQ-24)15 and patient diaries. We present the results of the QoL objectives, which aimed to determine the effects of treatment with Dysport 500 U on patient QoL, and everyday functions and activities. Pain may exert an influence on the patient's rating of the efficacy of BoNT-A therapy, which is not taken into account using the Tsui score. Consequently, pain was additionally evaluated using the aforementioned measures.
Methods
Study design, patients and treatment
This was a non-controlled, prospective, multicentre, open-label study conducted in Germany and Austria to investigate the comparable effectiveness and safety of 500 U Dysport for the treatment of patients (aged ≥18 years) with heterogeneous forms of CD, naïve to BoNT-A. Full details of study design, and inclusion and exclusion criteria, have been published previously by Hefter et al13 and are available through BMJ Open.
All patients received a single intramuscular injection with 500 U Dysport, diluted in 2.5 ml 0.9% NaCl. Complete details of the standardised injection protocol based on the symptoms assessed with the Tsui score have also been published previously.13
Assessments
The severity of CD was assessed by the investigating physicians at visit 1 (week 0; baseline), visit 2 (week 4) and visit 3 (week 12) using the Tsui rating scale total score under standardised conditions, with the patient in a relaxed seated position. The primary efficacy outcome measure was the change from baseline to week 4 in total Tsui score after treatment.13
Craniocervical Dystonia Questionnaire-24
The effects of treatment on QoL, pain and any restrictions of possible everyday functions and activities of the patient were assessed in comparison with baseline values using the validated CDQ-24.15 The CDQ-24 is a disease-specific QoL instrument designed to investigate problems in daily living skills related to CD, and comprises 24 items within five domains related to stigma (questions 7, 8, 9, 10, 18 and 22); emotional well-being (questions 11, 12, 13, 14 and 15); pain (questions 4, 5 and 21); activities of daily living (questions 1, 2, 3, 6, 19 and 20) and social/family life (questions 16, 17, 23 and 24). Scores for each item range from 0 to 4, representing increasing severity of impairment. In order to obtain scores for the individual subscales, the total score of each subscale (sum of the individual item scores) was transformed linearly to a 0–100 scale, where a score of 0 indicates the best and a score of 100 the worst possible QoL (which explains why some subscores, eg, stigma, have higher values than the total score). Assessment of the CDQ-24 was conducted at baseline (visit 1), week 4 (visit 2) and week 12 (visit 3).
Patient diary
Patients were provided with a diary, which was used to self-record weekly ratings (on an 11-point visual analogue scale; VAS) for items related to ‘day-to-day capacities and activities’ (0=not affected, 10=very severely affected), ‘pain’ (0=no pain, 10=strongest imaginable pain) and ‘duration of pain’ (0=never pain, 10=constant pain). Assessment of the patient diary was conducted at baseline (visit 1), week 4 (visit 2) and week 12 (visit 3).
Global assessment of pain
At visits 2 and 3, patients were required to assess change of pain associated with CD according to the following response categories: 1=no pain (any more); 2=less pain; 3=no change; 4=more pain.
Statistical analyses
All efficacy and QoL assessments were conducted in the intent-to-treat (ITT) population (ie, all patients of the safety population with a baseline (visit 1, week 0) and a post-baseline (visit 2, week 4 or visit 3, week 12) assessment of the Tsui rating scale).
Time course was analysed over visits 1, 2 and 3 or weeks 0, 4 and 12, respectively, of CDQ-24 subscale ‘pain’, diary item ‘pain’, global assessment of pain (at visits 2 and 3) and CDQ-24 total score for patients with valid data for all three pain assessments at all visits.
Inferential analyses of CDQ-24 total score and subscale changes from baseline at visits 2 and 3 were conducted for the total population and by main type of CD. Descriptive and inferential analyses of diary item changes from baseline at weeks 4 and 12 were performed for the total population and by main type of CD. Descriptive analyses of standardised pain measures (global assessment of pain by patient at visits 2 and 3; CDQ-24 ‘pain’ change from baseline at visits 2 and 3; diary items ‘pain’ and ‘pain duration’ changes from baseline at weeks 4 and 12) were assessed by main type of CD. All pain statements were documented differently; in order to allow comparisons between the different assessments, all pain measures were converted to a common scale using the following categories for change from baseline: less or no pain; no change or more pain.
Pearson correlation analyses were performed of total Tsui score change from baseline at visit 2 and diary items ‘pain’ and ‘pain duration’ changes from baseline at week 4, and CDQ-24 subscale ‘pain’ change from baseline at week 4. In addition, Pearson correlation analyses were performed between CDQ-24 total score and subscale score changes from baseline and changes from baseline for items of the patient diary.
Additional post hoc analyses were carried out to investigate the impact of concomitant depression on treatment effectiveness and QoL.
Results
Patient disposition and demographics
Baseline demographic, safety and tolerability data for all patients are available in the 2011 BMJ Open article by Hefter et al13 Of the 516 patients enrolled in the study, safety data were available for all but one patient (safety population: n=515). At least one adverse event was experienced by 213 (41.4%) of patients, of which 155 (30.1%) were considered to be related to study medication. Data of the Tsui rating scale at baseline (visit 1) and at least one post-baseline visit (visit 2 or 3) were available for 503 patients (ITT population). Overall, 26 patients discontinued the study prematurely, with the main reasons cited as insufficient compliance and lost to follow-up.
The majority of patients had torticollis (n=402; 78.1%; 112 patients (21.7%) had laterocollis; type of CD was unknown in one patient). Baseline characteristics were generally similar between patients with torticollis and laterocollis, as shown by Hefter et al.13 The proportion of patients with tremor was similar in both torticollis (36.1%) and laterocollis (36.6%) groups. However, approximately half of the laterocollis patients (47.3%) were affected by shoulder elevation compared with only one-third of torticollis patients (31.3%). The majority of patients in the total population (56.5%) were affected by pain (torticollis: 54.5%; laterocollis: 64.3%).
Mean CDQ-24 total score at baseline for the overall patient population was 39.6 (±18.8 (39.8 for ITT population)). Baseline mean CDQ-24 total scores did not differ markedly between the main CD types: torticollis (39.9) and laterocollis (38.8).
After analysis of the study data, 35 patients were identified with depression as concomitant disease, according to the preferred MedDRA term (6.8% of the total population). The Tsui score at baseline was comparable between patients with (n=34) and without (n=469) depression (8.6 and 8.4, respectively), as well as the decrease in Tsui score at week 4 minus baseline (−4.0 and −3.8, respectively).
Treatments and dosing
All treated patients received Dysport 500 U at baseline, with the exception of three patients who received 360, 400 and 460 U. The most frequently reported concomitant medications (>10% of patients) by therapeutic class were β-blocking agents (19%), agents acting on the renin–angiotensin system (14.4%), psychoanaleptics (13.6%), thyroid therapy (13%) and analgesics (10.1%). Use of concomitant medication was similar across CD subtypes.
Craniocervical Dystonia Questionnaire-24
In the total patient population, treatment with Dysport was associated with a statistically significant improvement in the CDQ-24 total score from baseline at week 4 (decrease of 11.1 points (95% CI −12.5 to −9.6); mean score: 28.7), which was maintained up to week 12 (decrease of 11.8 points (95% CI −13.1 to −10.4); mean score: 28.0; figure 1, p<0.001 at weeks 4 and 12 vs baseline).

Change in Craniocervical Dystonia Questionnaire-24 total and subscale scores from baseline to weeks 4 and 12 (ITT: total population). Total score and all subscores differed significantly from baseline to weeks 4 and 12 (p<0.001 at weeks 4 and 12 vs baseline). *Change from baseline score was worse at weeks 12 versus 4. ITT, intent-to-treat.
At weeks 4 and 12, Dysport treatment significantly improved all CDQ-24 subscale scores from baseline (figure 1, p<0.001). Patient-rated QoL at baseline was highest (worst) for subscale ‘stigma’ (mean score: 50.4) and lowest (best) for social/family life (mean score: 21.9). Accordingly, mean changes from baseline (at weeks 4 and 12) were highest for subscale ‘stigma’ (−16.8 (95% CI −19.0 to −14.7) and −16.4 (95% CI −18.4 to −14.3), respectively) and lowest for subscale ‘social/family life’ (−5.6 (95% CI −7.2 to −4.0) and −6.7 (95% CI −8.3 to −5.1), respectively). For all subscales, except ‘stigma’, continued improvement was seen from week 4 through to week 12. The small worsening in ‘stigma’ seems marginal when compared with the improvements seen in other categories, but correlates with an increasing Tsui score between weeks 4 and 12.
There were no statistically significant differences in QoL results between the torticollis and laterocollis groups (for total score and subscores).
Higher CDQ-24 total scores were recorded for the subgroup of patients with depression, with mean scores at visits 1 (baseline), 2 and 3 of 51.8, 41.7 and 38.5, respectively, compared with 38.9, 27.8 and 27.2, respectively, for those without depression. However, the changes in CDQ-24 total score from baseline to weeks 4 and 12 were comparable between patients with and without depression. The difference between patients with and without depression was most apparent for the CDQ-24 subscale ‘emotional wellbeing’ at visits 1, 2 and 3: mean scores of 57.5, 47.4 and 43.8, respectively, for patients with depression, and 38.0, 27.7 and 26.7, respectively, for those without depression. No differences were observed for CDQ-24 total scores between the torticollis and laterocollis groups of patients with depression. However, a noticeably smaller change from baseline to visit 2 was seen in the depressed laterocollis subgroup for ‘emotional wellbeing’ (−4.5) when compared with the depressed torticollis subgroup (−12.5).
Patient diary
Similar to the results for CDQ-24, patients’ diaries reflected positive treatment effects of Dysport on the VAS-assessed activities of daily living, pain and pain duration (mean±SD baseline values 5.3±2.8, 4.1±3.0 and 4.7±3.4 points, respectively). As shown in figure 2, for the total population, ‘pain’, ‘pain duration’ and ‘day-to-day functions and activities’ significantly improved at weeks 4 and 12 vs baseline (p<0.001). For ‘pain’ and ‘pain duration’, there was further mild improvement from weeks 4 to 12.
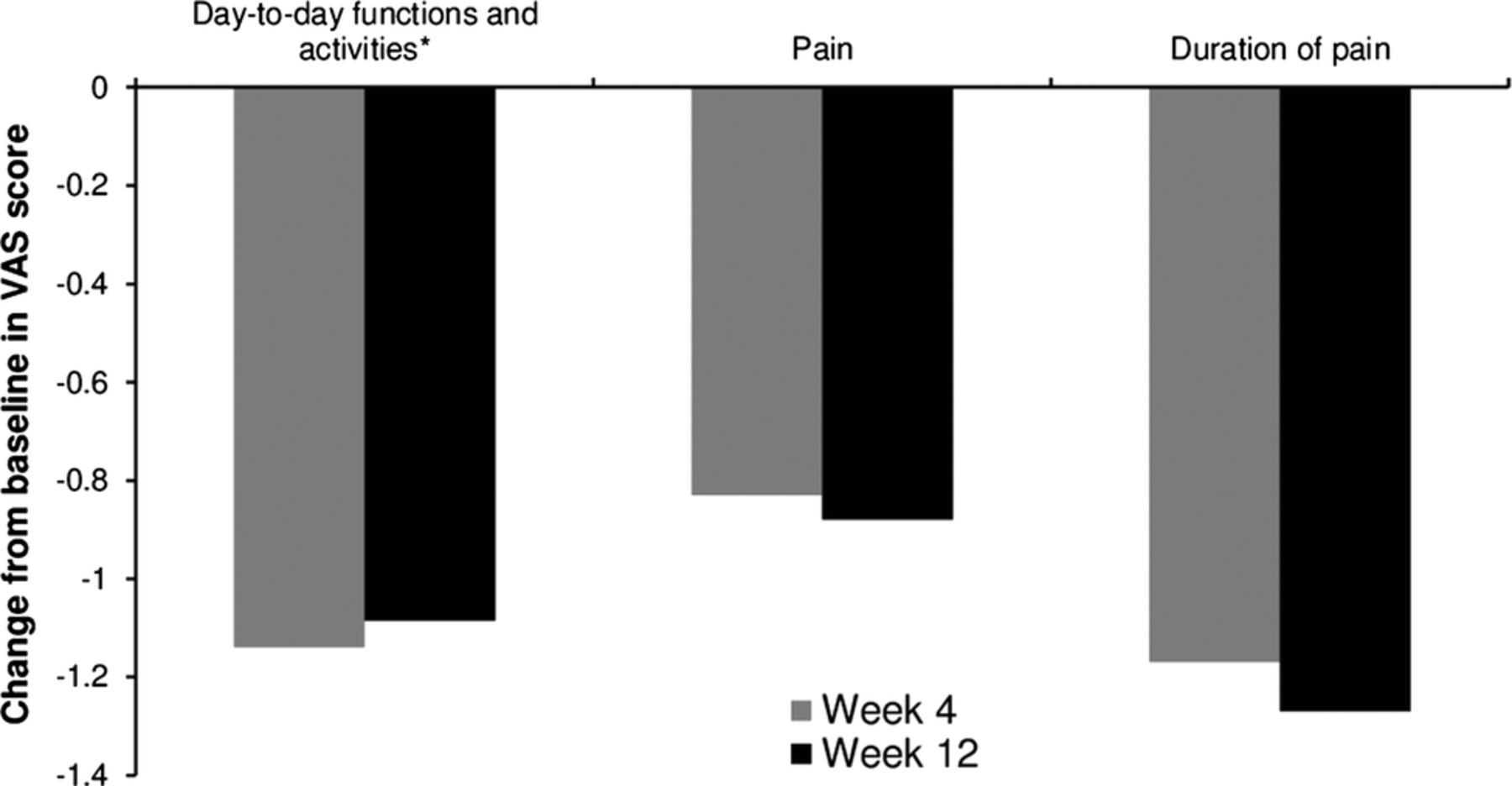
Change in patient diary visual analogue score (VAS) from baseline to weeks 4 and 12 (ITT: total population). t Test analysis: p<0.001 at weeks 4 and 12 versus baseline. *Change from baseline score was worse at weeks 12 versus 4. ITT, intent-to-treat.
Descriptive and t test statistical analyses of diary item changes of the CD subgroups (torticollis and laterocollis) from baseline to weeks 4 and 12 showed that all changes were statistically significant (p<0.05), with the exception of change of ‘day-to-day functions and activities’ of laterocollis patients between baseline and week 12 (p=0.0531). There were no other statistically significant differences in patient diary results in the torticollis and laterocollis subgroups.
Global assessment of pain
Most patients judged pain relief higher at week 12 than at week 4. Pain relief (less or no pain) was perceived by 330 patients (66%) at week 4 and by 363 patients (74.1%) at week 12 (no change: 16.4% at week 4 and 16.9% at week 12; more pain: 17.6% at week 4 and 9% at week 12).
Results of correlation analyses
CDQ-24 and Tsui score
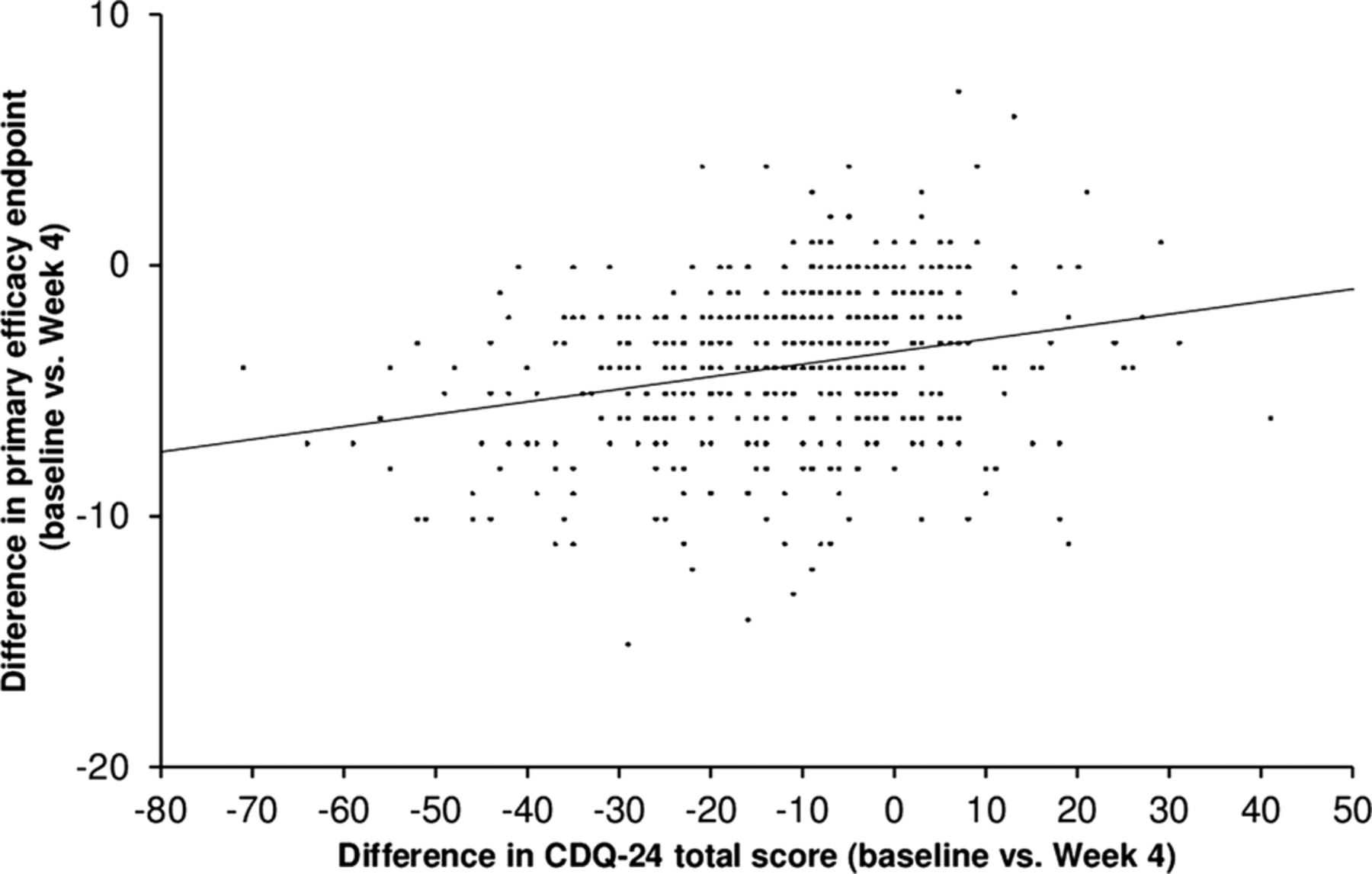
Total CDQ-24 and all CDQ-24 subscores correlated significantly at baseline with Tsui score (p<0.001), with a correlation coefficient (R) varying between 0.17 and 0.27. Comparing the time course of Tsui score and QoL, the positive trend of the CDQ-24 total score at week 4 (24% improvement) continued up to week 12 (27.5% improvement), although the Tsui total score deteriorated between week 4 (44.3% improvement) and week 12 (24.3% improvement) in all patients (figure 3). Nevertheless, statistically significant correlations (p<0.001) were seen between changes from baseline to visits 2 (figure 4) and 3 in total CDQ-24 score and in Tsui total score, but the correlation at week 4 was slightly higher (R=0.26) than at week 12 (R=0.24). Correlations (R<0.3) were also seen between changes from baseline to visits 2 and 3 in individual CDQ-24 subscale scores and in Tsui total score, which were statistically significant (p<0.001) for ‘stigma’, ‘emotional wellbeing’, ‘pain’ and ‘activities of daily living’. For social/family life, the correlation was significant at week 4 (p<0.01) but not at week 12 (p=0.054).

Time course of change in total Tsui score and total Craniocervical Dystonia Questionnaire-24 (CDQ-24) score. Tsui-score: week 4, n=503 patients; week 12, n=490 patients. CDQ-24: week 4, n=483 patients; week 12, n=473 patients.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation between change in Craniocervical Dystonia Questionnaire-24 total score and change in total Tsui score from baseline to week 4. Display of raw data; one dot may represent more than one patient. Correlation coefficient: 0.26, p<0.001, n=484 (week 12: correlation coefficient: 0.24, p<0.001, n=474).
Pain and Tsui score
A correlation was found between the global pain assessment and the Tsui score for the total population: patients with an assessment of ‘less pain’ had a higher decrease in mean Tsui score at week 4 (−4.5) than patients with ‘no change in pain’ (−3.0) and patients with ‘more pain’ (−3.2), respectively. The highest decrease in mean Tsui score (visit 2 vs baseline: −4.9) was achieved by patients in the laterocollis group in which 64.3% of the patients had reported pain at baseline vs 54.5% in the torticollis group.
Global assessment of pain, CDQ-24 subscale pain and patient diary pain
Overall, a significant positive relationship (p<0.001) was seen between all pain parameters (ie, CDQ-24, patient diary and global assessment of pain), with the CDQ subscale pain and the diary item of ‘pain duration’ showing the lowest correlation (R=0.36). The correlation between patient global assessment of pain and the pain intensity in the patient diary resulted in a much higher correlation coefficient (R=0.46).
The percentage of patients reporting a global improvement of pain at week 4 (66%) was higher than the percentage of patients documenting a pain improvement in their diaries (50.2–52.3%). At week 12, the discrepancy was even higher between global improvement of pain (74.1%) and the percentage of patients documenting pain improvement in their diaries at this time point (48.3–55.2%).
CDQ-24 activities of daily living and patient diary daily activities
Comparing all CDQ subscales with the patient diary, the highest correlations in the total population (and for both CD types) were observed between the patient diary item of ‘day-to-day function’ and the CDQ-24 subscale of ‘activities of daily living’ and ‘stigma’, with R=0.48 and 0.37 (for total population), respectively, at week 4, and R=0.43 and 0.38 (for total population), respectively, at week 12 (p<0.001).
Discussion
This study, the largest published, prospective, open-label cohort study of de novo patients with CD to date, demonstrated that a single dose of 500 U Dysport given according to a standardised injection scheme resulted in an improvement in disease-related impairment of QoL, as assessed by CDQ-24. Notably, the CDQ-24 results in week 12 were better than those recorded in week 4, despite an increase (worsening) of Tsui score (figure 3), suggesting that improvements in QoL are maintained for a clinically significant duration. Our findings imply that the positive effects of BoNT-A following treatment are encouraging to patients and help them gain perspective on their condition. Improvement of QoL seems to be better at week 12, just before the second injection, compared with week 4 when the injection has its maximal effect. This aspect and the weak correlation between improvement in CDQ-24 and Tsui underscore the involvement of additional factors beyond abnormal head posture in influencing QoL in CD. We believe that patients appreciate improvements in their condition relative to baseline and that severity of CD can systematically be reduced by repetitive injections every 3 months. This perspective potentially accounts for better scores at week 12 compared with week 4. Additionally, greater improvement at week 12 compared with week 4 may reflect the ability of the CDQ-24 to capture longer term changes in QoL.15
Improvement of QoL items linked to abnormal head posture, such as ‘stigma’, did however follow the temporal course of head position, with worse scores at week 12 than at week 4. This is in contrast to the other subscales of the CDQ-24, which all showed continued improvement. Stigma is associated with the worst baseline CDQ-24 subscale score for all patients. The appearance of patients can be seriously affected by involuntary movements seen in CD and self-perceived stigma can be a major source of disability.11 ,16 Indeed, results from the present study show that stigma is seemingly important for the everyday function of patients, with a positive correlation being observed between the CDQ-24 subscale ‘stigma’ and the diary item of ‘day-to-day functions and activities’.
Pain is another important factor influencing QoL. Interestingly, better improvements in pain were recorded when the clinician was present for the assessment (global assessment of pain) than rated by the patients using their diaries at home. Regardless, systematic improvement of pain, not only of pain intensity but also of pain duration, was reported by all assessments. In general, an improvement of Tsui score correlated positively with an improvement of pain in this study, with patients recording less pain on the global pain assessment achieving the greatest reduction in Tsui total score.
In this study, patients with depression as concomitant disease showed worse QoL scores at baseline. Importantly, following Dysport treatment, patients with depression experienced similar benefits to those without depression, as demonstrated by similar changes from baseline at weeks 4 and 12 for the Tsui score, and for QoL between the depressed and non-depressed subgroups. The ability of BoNT-A treatment to improve QoL in the presence of concomitant depression is particularly pertinent in view of published observations highlighting the role of depression as a key determinant of poor QoL in patients with CD.11
Although laterocollis patients responded well according to Tsui score, pain appeared to be more common in this patient group than in patients with torticollis. The higher proportion of shoulder elevation in laterocollis patients may be one possible explanation for the increased rate of documented pain in these patients. As presented previously,13 improvements in CD symptoms were confirmed by investigator and patient global assessment of symptoms without distinct (significant) group differences, although laterocollis patients experienced more frequent severe muscle weakness as an adverse event than torticollis patients (8.9% laterocollis, n=10 vs 1.7% torticollis, n=7). Investigator and patient ratings of tolerability also varied the most in the laterocollis group at week 4, which could probably be explained by the higher rate of severe muscular weakness reported in these patients.13 Although torticollis and laterocollis patients showed the same clinical response in the Tsui score, there are obviously differences between the two groups in disease perception. More analyses of the available study data including side effects, such as muscular weakness, may help us understand these apparent inconsistencies. Moreover, further studies may clarify if this was a random effect or if these patients would benefit from longer treatment duration with Dysport. Finally, the specific head position, that is, whether the head is tilted or rotated, does not seem to play an essential role in emotional and social well-being; patients with either torticollis or laterocollis demonstrated comparable results in the CDQ-24 subscale ‘emotional wellbeing’ at baseline.
The results from this study support those from a published study by Ben-Shlomo et al11, which demonstrated that, in addition to disease severity, QoL in patients with CD is predominantly determined by factors such as self-esteem, self-deprecation, stigma and depression. Consequently, the care of these patients should not only focus on the reduction of CD symptom severity, but also on the improvement of the patient's psychological well-being. The use of pharmacological treatments with the ability to reduce disease severity has been shown to have a major benefit on both the physical and mental well-being of CD patients.11 Recent controlled studies, for example,17 have shown that short-term treatment with a combination of pharmacological therapy (BoNT-A) and a physical treatment programme (comprising self-control techniques and counselling) may be more effective than a sole pharmacological intervention. Therefore, further studies investigating the long-term effects of pure pharmacological and multidimensional treatment programmes on QoL are warranted.
In conclusion, CD is a disabling and often painful illness that interferes with activities of daily living. As a result, CD has a significant adverse impact on patient's physical and mental well-being and QoL. Results from this large, prospective, open-label study support the ability of Dysport 500 U to provide sustained efficacy in reducing motor symptoms coincident with significant improvements in pain and QoL among patients with CD, and provide the foundation for further investigation in randomised, controlled studies.
Acknowledgments
Data management and statistical analyses were performed by GKM Gesellschaft für Therapieforschung in Munich, Germany. Editorial assistance for the preparation of this manuscript was provided by Ogilvy Healthworld Medical Education; funding for this was provided by Ipsen Pharma. The authors would like to thank Christiane Colling, PhD, Medical Project Manager, Ipsen Pharma, for her assistance in the conduct of the study and for review of the manuscript.
References
Footnotes
-
Contributors All authors were involved in the concept and study design, study conduct, data collection, analysis and interpretation, manuscript writing, review and critique. All authors approved the final manuscript. HH was the coordinating investigator of this study.
-
Funding This study was supported by Ipsen Pharma GmbH, Germany. The contents of this publication, especially the conclusions expressed, are those of the authors of the manuscript only. Funding from Ipsen Pharma made the conduct of the study, the previous publication of primary outcomes and this presentation of secondary outcomes possible. The decision to publish the results was the authors’ only and was made independently from the funders. The study design and concept were developed by the authors in collaboration with Ipsen Pharma; study conduct and data collection were supported by Ipsen Pharma.
-
Competing interests All authors are consultants for Ipsen.
-
Ethics approval Ethikkommission der Landesärztekammer Baden-Württemberg and Ethik-Kommission der Medizinischen Universität Wien und des Allgemeinen Krankenhauses der Stadt Wien.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.