Article Text

Abstract
Objectives Tumour recurrence of glioblastoma multiforme (GBM) after initial treatment with surgical resection, radiotherapy and chemotherapy is an inevitable phenomenon. This retrospective cohort study compared the efficacy of interstitial high dose rate brachytherapy (HDR-BRT), re-resection and sole dose dense temozolomide chemotherapy (ddTMZ) in the treatment of recurrent glioblastoma after initial surgery and radiochemotherapy.
Design Retropective cohort study.
Setting Primary level of care with two participating centres. The geographical location was central Germany.
Participants From January 2005 to December 2010, a total of 111 patients developed recurrent GBM after initial surgery and radiotherapy with concomitant temozolomide. The inclusion criteria were as follows: (1) histology-proven diagnosis of primary GBM (WHO grade 4), (2) primary treatment with resection and radiochemotherapy, and (3) tumour recurrence/progression.
Interventions This study compared retrospectively the efficacy of interstitial HDR-BRT, re-resection and ddTMZ alone in the treatment of recurrent glioblastoma.
Primary and secondary outcome measures Median survival, progression free survival and complication rate.
Results Median survival after salvage therapy of the recurrence was 37, 30 and 26 weeks, respectively. The HDR-BRT group did significantly better than both the reoperation (p<0.05) and the ddTMZ groups (p<0.05). Moderate to severe complications in the HDR-BRT, reoperation and sole chemotherapy groups occurred in 5/50 (10%), 4/36 (11%) and 9/25 (36%) cases, respectively.
Conclusions CT-guided interstitial HDR-BRT attained higher survival benefits in the management of recurrent glioblastoma after initial surgery and radiotherapy with concurrent temozolomide in comparison with the other treatment modalities. The low risk of complications of the HDR-BRT and the fact that it can be delivered percutaneously in local anaesthesia render it a promissing treatment option for selected patients which should be further evaluated.
- Neurooncology
- Radiotherapy
this is an open-access article distributed under the terms of the creative commons attribution non-commercial license, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. see: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
Analyse survival rates after salvage treatment of recurrent glioblastoma.
-
Compare the efficacy of interstitial high dose rate brachytherapy (HDR-BRT), re-resection and dose dense temozolomide chemotherapy (ddTMZ) alone in the treatment of recurrent glioblastoma.
-
To report mature results of long-term follow-up, outcomes and toxicity.
Key messages
-
HDR-BRT is a safe alternative for salvage treatment of recurrent glioblastoma.
-
The HDR-BRT group did significantly better than both the reoperation and the ddTMZ groups.
Strengths and limitations of this study
-
Non-randomisation regarding choices of treatment and selection bias.
Inroduction
Glioblastoma multiforme (GBM) is the most common of all gliomas and the most malignant primary brain tumour. Despite multimodality initial treatment with gross total removal, radiotherapy and chemotherapy, the prognosis of GBM remains poor1 and the reported median survival is about 14–18 months.2 Tumour recurrence is observed in almost all patients. The treatment algorithm for recurrent glioblastoma varies from centre to centre, and there is not yet a consensus on the most appropriate treatment for this devastating disease. Non-surgical treatment such as intensive temozolomide chemotherapy is, at best, a treatment option after which long-term survival is seldom observed.3 ,4 Dose dense temozolomide treatment (ddTMZ), as 1 week on/1 week off regimen, did not show superior efficacy as compared with the standard day every 4 weeks schedule.5 New agents such as bevacizumab are being tested as single agent chemotherapy or in combination with other drugs.6 Resurgery is sometimes recommended and probably produces the better survival results but also carries associated risks.7 Studies have shown that the extent or completeness of resection have been correlated with survival.8 ,9 Previous studies have retrospectively assessed outcomes of patients after recurrent glioblastoma tumour resection,10–13 and tried to develop prognostic scoring systems to predict survival after surgery.7 However, surgical resection is not a good option in many patients in the recurrent setting, given the extent of the recurrent tumour and the proximity to eloquent neurological structures. Another feasible treatment option that can play an important role in providing palliation is the interstitial high dose rate brachytherapy (HDR-BRT) consisting of an afterloading 192Ir implant, which is applicable even to patients with extended recurrent tumours and can be delivered via the percutaneous approach with CT guidance.14 ,15
The aim of this retrospective study was to describe the survival rates and 3-month radiographic response to treatment for recurrence of glioblastoma, with either HDR-BRT, resurgery or intensive temozolomide chemotherapy, acknowledging selection bias over which one of the three salvage therapies was chosen. Despite its methodological and conseptual limitations due to its retrospective nature, this report gives a full account of consecutive patients with recurrent glioblastoma treated in our departments with HDR-BRT or resurgery or sole ddTMZ and provides survival rates, as well as compares and contrasts the outcomes and complication rates between the three different groups of salvage treatment.
Patients and methods
We conducted a retrospective analysis from consecutive patients with recurrent glioblastoma after initial surgery and radiotherapy with concomitant temozolomide who were admitted in our hospital between January 2005 and December 2010. This study was approved by the institutional research ethics board. Among the 115 patients with glioblastoma recurrence, 111 patients underwent either HDR-BRT, re-resection or ddTMZ as a salvage treatment, and they formed the focus of interest in this study. Prospectively collected data on patient characteristics, clinicopathological features and survival outcomes were reviewed. The primary endpoint of the study was disease-specific survival. Secondary endpoints were complication rates, adverse events and radiographic response to salvage therapy. All the patients had received previous surgery as primary treatment for initial histology-proven glioblastoma (WHO grade 4), and gross total resection was performed in 81/111 (73%) and subtotal resection in 30/111 patients (27%). All the patients were given postoperative partial-brain irradiation with a focal dose of up to 60 Gy, and the median interval from the date of surgery until the start of radiotherapy was 24 days (6–58 days). All the patients received temozolomide chemotherapy as part of their initial treatment.
The inclusion criteria were as follows: (1) histology-proven diagnosis of glioblastoma (WHO grade 4), (2) primary treatment with resection and radiochemotherapy, and (3) tumour recurrence/progression. The exclusion criteria for this study formed simultaneously the contraindications for further treatment: (1) patients with poor neurological function Karnofsky performance score (KPS) <70 and (2) patients with consciousness impairment were considered ineligible. No case of secondary GBM was included.
The median recurrent tumour volume in all groups was 46 cm³ (3–207 cm³). The HDR-BRT consisted of an afterloading 192Ir implant which delivered a median dose of 40 Gy (30–50) at twice-daily fractions of 5.0 Gy to a CT-MRI fusion-defined planing treatment volume. Catheter implantation was implemented using interactive CT guidance under local anaesthesia and sedoanalgesia and the median catheter number was 7 (1–21). A detailed description of the implantation technique and brachytherapy planning can be found in our previous reports in the literature.14 ,15
Patients in the surgical arm underwent a maximal safe surgical resection of their recurrent tumours. Resurgery and HDR-BRT were followed by TMZ chemotherapy as an adjunctive treatment with a dose of 100 mg/m2 for 5 days in a 28-day cycle. Of course, the rechallenge of these patient groups with TMZ confounds interpretation of the results but we considered not to withhold such a therapy from a patient population with this devastating disease.
In patients treated with sole chemotherapy, we used the 1 week on/1 week off temozolomide with a daily dose of 150 mg/m², until documented disease progression or unacceptable toxicity. We chose this more rigorous dose regimen of TMZ according to the publications of Wick et al16 who reported a progression-free survival (PFS) as high as 48% with an overall survival for 12 months of 81% Toxicity was evaluated according to the Common Terminology Criteria for Adverse Events (CTCAE; V.3.0). In case of haematological toxicity grade 4 or non-haematological toxicity grade 3, the dosage TMZ of the next cycle was reduced by 25 mg/m²/day. In case of CTCAE grade 4 non-haematological toxicity, the patient stopped treatment. In case of a grade 4 haematological toxicity or a grade 3 non-haematological toxicity at dose level of 75 mg/m²/day, the patient went off treatment. In case of dose reductions, dose re-escalation was not allowed. Blood examinations were done on day 15 and day 29 and when platelets were above 100×109/l and neutrophils counts above 1.5×109/l, the following 7 days TMZ was administered. Otherwise treatment was postponed until recovery to CTCAE grade 1 and/or platelets were above 100×109/l. The treatment was stopped if it had to be postponed for more than 4 weeks.
Diagnostic criteria for recurrent glioblastoma
The follow-up protocol for patients with glioblastoma in our centre consisted of MRI of the brain not later than 48 h after tumour resection. Surveillance for tumour recurrence was conducted using MRI scans 8 weeks after radiochemotherapy and thereafter, every 3 months. Glioblastoma recurrence is defined as the appearance or enlargement since prior imaging, of a contrast-enhancing mass on T1-weightedMRI. Differentiating tumour recurrence from radiation necrosis can be difficult, for this task we used effectively in some cases positron emission tomography, MR spectroscopy and MR perfusion. In cases where these data were not useful, we obtained a stereotactic biopsy.
Radiographic response to therapy was evaluated at 3 months after starting the salvage treatment using the Macdonald criteria.17 These criteria use the largest cross-sectional area of the postcontrast images, neurological status and corticosteroid dose. Complete response (CR) was defined as complete disappearance of measurable disease by MRI, partial response (PR) as 50% decrease in the area of enhancement and progressive disease (PD) as >25% increase in the area of enhancement, appearance of a new lesion or deterioration in clinical status, probably secondary to tumour progression. Patients with CR or PR had to be on the same or decreased steroid dose and have stable or improved neurological findings. Stable disease (SD) is defined for patients not fulfilling CR, PR or PD criteria.
Selection criteria for HDR-BRT, re-resection or ddTMZ as a salvage treatment
Only patients with recurrent tumours in areas not traditionally considered eloquent brain regions were included for re-resection. It was generally avoided in the presence of (1) affected basal ganglia, and/or (2) an involvement of eloquent/critical brain areas: the presumed motor area, the presumed speech area, (3) a platelet count <100×109/l and/or leuopaenia <4/nl, signifying myelosuppression after chemotherapy.
Extension of tumour recurrence in more than two lobes, multilocality of recurrence and affection of both hemispheres would discourage neurosurgeons to treat with resurgery. HDR brachytherapy and ddTMZ were selected for recurrent tumour independently from tumour location or extent. All patients were considered in our oncological conference, after careful analysis of the radiological studies and clinical factors, the multidisciplinary team of neurosurgeons, radiotherapists and neuroradiologists developed the treatment plan. The study was based on different policies of treatment. Allocation to HDR-BRT, re-resection or ddTMZ was not randomised. The best approach involved collaborative interactions and decisions made by the team. If controversy existed, and provided that the above selection criteria are fullfilled, resurgery was considered as the first treatment choice. Patients were generally not considered for treatment unless their KPS was ≥70.
Stereotactic biopsy for histological confirmation was performed in all patients included in this study. All the patients were informed about the pros and cons of salvage therapy modalities. Many patients refused further treatment options and among alternatives of supportive care, intensive temozolomide chemotherapy was offered as salvage treatment (n=23).
Treatment planning in HDR-BRT was devised to deliver 60 Gy to the edge of a volume that extends 1 cm beyond the contrast-enhancing tumour, with variations included to spare radiosensitive structures (eg, optic chiasm).
Statistical analysis
Continuous variables were expressed in medians (IQR) and compared using the Mann-Whitney U test. Categorical variables were compared with the χ2 test or Fisher's exact test when appropriate. Overall survival and median PFS of the three study groups were estimated by the Kaplan-Meier method. Comparison of survival between groups was performed with the log-rank test. Median PFS after treatment of glioblastoma recurrence was defined as the period from the date of treatment of recurrent glioblastoma to the date of the second tumour recurrence, progression or death. Overall survival was defined as the period from the date of first surgery for glioblastoma to the date of death related to any cause. A p value ≤0.05 was considered to be significant. Statistical analysis was performed using the BiAS computer software program.
Results
The median follow-up duration was 49 months (11–61 months). Table 1 shows the patients’ characteristics and KPS profiles at the time of glioblastoma recurrence. The three groups had similar KPS rates and a similar incidence of comorbid illness. Patients in the HDR-BRT group were older than those in the re-resection and chemotherapy groups but this difference was not statistically significant.
Demographic, clinical and radiographic characteristics of patients with recurrent glioblastoma*
All patients in the re-resection group had recurrent tumours not invading the eloquent regions, whereas 74% of patients in the brachytherapy group had some kind of affection of the presumed motor area, the presumed speech area and basal ganglia. Pretreatment laboratory investigations at the time of recurrence were comparable for the three groups except that 10% patients in the HDR-BRT group had a lower white blood cell count level. With regard to the extent of resection of the primary pathology (gross total vs subtotal) and tumour volume of the primary group the three groups shared similar features. The HDR-BRT group, however, had a larger recurrent tumour size than the re-resection and ddTMZ groups (51 vs 43 vs 45 cm³), suggesting that the size of tumour recurrence played an important role in aggressiveness of treatment. Time to develop first recurrence was similar in all groups (12.2 vs 8.7 vs 9.1 months). O-6-methylguanine-DNA methyltransferase (MGMT) methylation was studied in 30% of the cases (33/111 patients) and was similar in the three groups.
OTable 2 showed the complication rates of patients undergoing HDR-BRT, re-resection and ddTMZ alone as salvage treatment. Six patients developed procedure-related morbidities in the HDR-BRT group. Among those, two developed intracerebral bleeding after catheter implantation and one of them died due to massive haemorrhage. One patient developed bacterial meningitis postexplantation, and was treated successfully with antibiotics. Symptomatic radiation necrosis occurred in two cases and manifested several months after brachytherapy. They were managed conservatively, either by corticosteroid or by intravenous mannitol.
Complication rates
Four patients in the resurgery group developed procedure-related morbidities and two patients succumbed during the same hospital admission. Nine patients in the ddTMZ group developed procedure-related morbidities. One patient developed pneumocystis carinii pneumonia and died. Eight patients discontinued TMZ because of toxicity: grade 4 thrombocytopaenia (4), persistent grade 4 leucopaenia (3) and grade 4 elevated transaminases (1). The incidences of procedure-related morbidity and hospital mortality between HDR-BRT and reoperation groups were not statistically different for the three groups. The higher complication rate in the ddTMZ group was due to increased toxicity. Adverse events of all treatment groups due to toxicity are summarised in table 3.
Adverse events due to toxicity in different treatment groups
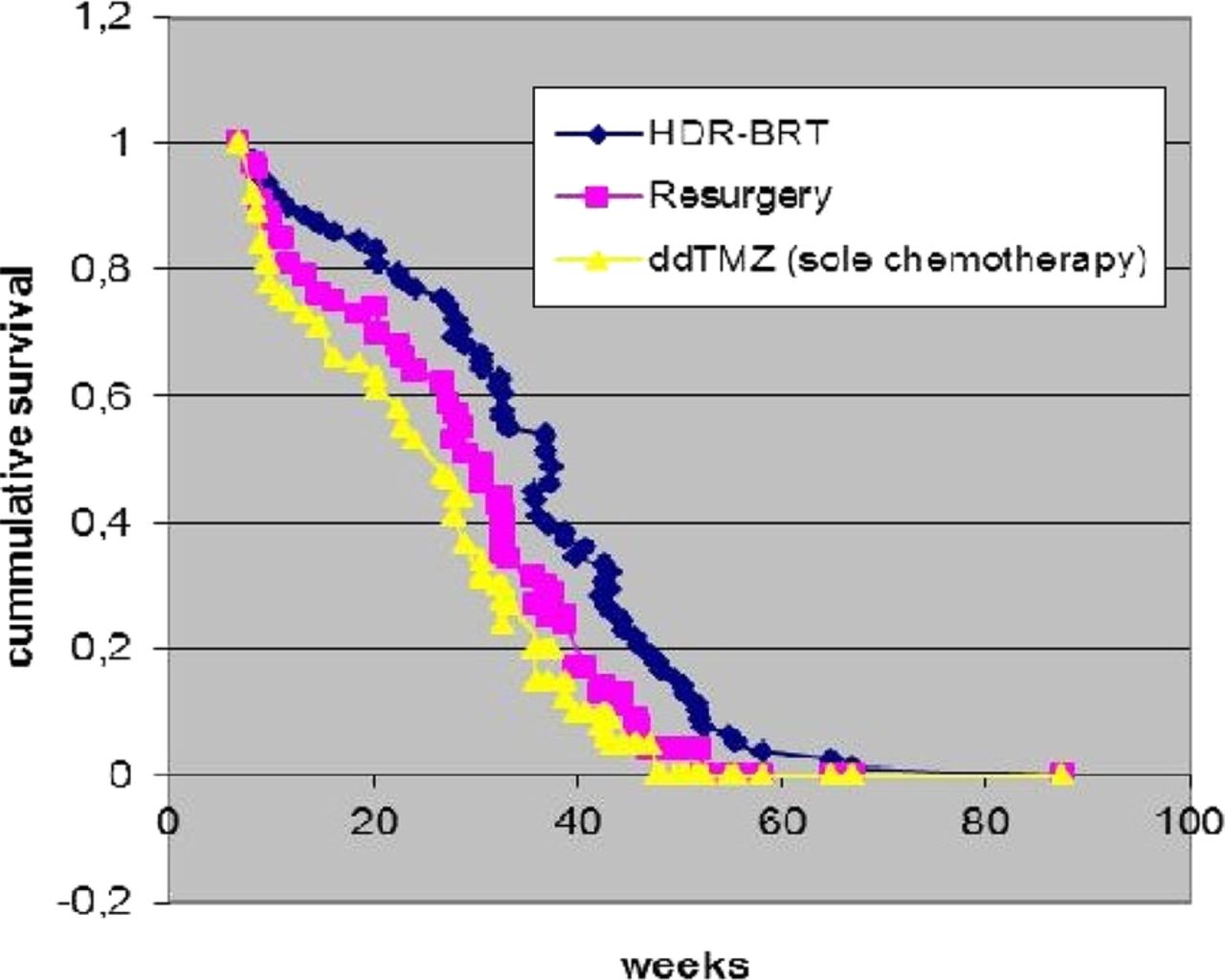
Overall survival was defined as the time from primary surgery to the time of death or last follow-up. After a median follow-up of 49 months, the median overall survival was 82 weeks in the HDR-BRT group, 64 weeks in the resurgical group and 48 weeks in the sole chemotherapy group whereas the median survival after salvage therapy of the recurrence was 37, 30 and 24 weeks, respectively (Kaplan-Meier survival curves in Ofigure 1). The HDR-BRT group did significantly better than both the reoperation (p<0.05) and the chemotherapy groups (p<0.05).
{kind=link}
Kaplan-Meier survival analysis after salvage therapy.
The radiographic response rate (CR and PR), using the Macdonald criteria, 3 months after initiation of the salvage therapy was 24% in the HDR-BRT group, 28% in the resurgical group and 8% in the ddTMZ alone group (Table 4). The baseline scan was the MRI within the first 48 h after the initial treatment (primary surgery) which was compared with the MRI scan at 3 months after the initiation of the salvage treatment.
Radiographic response in patients with recurrent glioblastoma, 3 months after initiation of the salvage treatment
The time to develop progression (PFS) was 32 weeks in the HDR-BRT group, 21 weeks in the resurgical group and 15 weeks in the chemotherapy alone group. By excluding recurrent tumours with volume larger than 30 ml (n=76, 68%) and tumours that were subtotal resected (n=30, 27%) during treatment for the primary glioblastoma, the times to develop progression were extended in the re-resection and sole chemotherapy groups to 24 and 18 months, respectively but were not significantly different in the HDR-BRT. The survival rate after HDR-BRT was also independent of age (≤50 years vs >50 years). In the subgroup of patients ≤50 years we observed an extension of the PFS in the re-resection and sole chemotherapy groups to 25 and 19 months, respectively.
The PFS-6 rate after treatment of glioblastoma recurrence in the HDR-BRT group was 64%. The corresponding rates in the re-resection and sole chemotherapy groups were 41% and 29%.
Univariate analysis of five clinical and radiological parameters (Table 5) showed that time to progression after first treatment and time to the second recurrence (progression) after treatment of the first recurrence were significant clinical factors that adversely affected overall survival in all groups. Age (≤50 years vs >50 years) and tumour volume (≤30 vs >30 ml) affected overall survival only in the resurgery and sole chemotherapy groups. In the multivariate analysis, recurrence with tumour volume of more than 30 ml, age >50 years remained an independent unfavourable prognostic factor for overall survival in the resurgery and sole chemotherapy groups (p<0.05).
Clinical and radiological parameters
The median KPS of the entire patient population was 80 at the time of salvage treatment. At the first 2-month evaluation periods, the median KPS was 80 for the HDR-BRT group, 70 for the resurgery group and 70 for the sole chemotherapy group, respectively. Therefore, there was no severe deterioration regarding function in the first 2 months immediately following salvage treatment in any of the groups.
Discussion
Salvage treatment of recurrent glioblastoma with HDR-BRT achieved in this retrospective study a better survival outcome and comparable radiographic response and complication rates in comparison to those seen with re-resection or ddTMZ.
Despite multimodality treatment of glioblastoma and the refinements of surgical techniques by using 5-aminolevulinic acid for fluorescence-guided surgery over the past years, the reported median survival is about 14–18 months.2 Nonetheless, treating the patients in an attempt to improve the quality of life and longevity is of utmost importance. Tumour recurrence is common, with a 2-year survival rate of only 2.2%.16 In all, survival time after manifestation of recurrence is extremely limited,10 ,18 hence it is important for neurosurgeons to select the most appropriate treatment for patients with recurrent glioblastoma. Variables of the primary surgery predicting longer survival in several studies include extent of resection (gross total), younger age (<50 years), higher KPS, normal mental status, smaller tumour volume and MGMT methylation.7 ,19
Treatment of glioblastoma recurrence poses several technical challenges, including bigger tumour volumes, significant gliosis and adhesions from the previous operation and proximity of the tumour to eloquent brain areas. The latter may be a condition which is a relative contraindication to re-resection. Surgery, if attempted, and usually in combination with other regimens, has limited success, while the risk of mortality and postoperative morbidity is high.11 ,12 Similarly, chemotherapy as sole treatment for recurrent glioblastoma20 ,21 gives predominantly unsatisfactory results. On the other hand, Wick et al have shown that a rigorous regimen (150 mg/m² daily on a week on/week off cycle) may yield a PFS of 6 months as high as 48% with an overall survival for 12 months of 81%. We decided to use temozolomide in this recurrent setting because it is well tolerated, has good oral bioavailability and is convenient to administer as an outpatient regimen. Our study showed a lower benefit of ddTMZ in recurrent glioblastoma in comparison to other treatment modalities. Of course, one may assume that the majority of these patients would have an unmethylated MGMT promoter. Thus, if ddTMZ would have been effective in overcoming that resistance, one would expect a more favourable outcome in these patients, regardless of the MGMT promoter status. Other trials also expressed doubt on the usefulness of intensified dosing regimens.5
In view of the limited success rates of surgery and chemotherapy, the role of reirradiation, stereotactic radiosurgery and BRT is gaining more importance. Gutin et al suggested that brachytherapy is promising for certain recurrent malignant gliomas. The authors implanted temporarily 125I sources using stereotactic techniques.22 However, radiation necrosis dampened the results of HDR temporary 125I seed implants which also require a stereotactic frame placement for seed delivery. Repeated operations for radionecrosis were observed and may be explained by inhomogeneous dose distribution and slight migration of seeds over time. Previous studies show the effectiveness of fractionated stereotactic radiosurgery (FSRS) as an option for treatment of recurrent glioblastoma.23–25 Combs et al23 reported 5 months PFS after FSRS and 21 months median overall survival. However, SRS is not recommended for recurrent lesions >40 mm in diameter26 and the fulfilment of this restriction immensely limits patient’s eligibility for treatment. Low dose rate (LDR)-BRT is an applied method to deliver additional dose while sparing healthy tissue.27 ,28 In a previous study we demonstrated a significant improvement in overall survival after HDR-BRT.14 In spite of notably larger tumour size in comparison to previous seed, LDR and SRS trials and expanded eligibility criteria, the results were encouraging. Furthermore, the radiobiological advantages of HDR-BRT in comparisson to the other treatment modalities are due to shorter treatment duration and higher isodoses (eg, >150%) in the main/central part of the target volume. Despite the retrospective nature and selection bias of this study we aimed to offer data on survival rates of different treatment groups and to facilitate decision making for salvage treatment on recurrent glioblastoma.
Our present study showed that HDR-BRT could achieve better long-term survival outcomes to those seen with re-resection and sole temozolomide chemotherapy in patients with recurrent glioblastoma. It is obvious that a retrospective comparison with HDR-BRT with resurgery and ddTMZ on which the above conclusions are drawn is complicated by bias of patient selection. Although the cases of HDR-BRT group included in this study were more demanding because of bigger tumour volumes and involvement of eloquent regions, this, however, did not translate into increased perioperative morbidity and mortality or complication rates compared with resurgery. After excluding confounding factors (incomplete resection of recurrent tumour) for further progression, the survival benefit of HDR-BRT remained unchanged. There are several reasons why HDR-BRT is a promising treatment option for glioblastoma recurrence. First, HDR-BRT can be delivered percutaneously, under local anaesthesia and sedoanalgesia, thereby avoiding a second operation. Second, HDR-BRT is applicable even to tumours proximal to eloquent brain areas. Third, HDR-BRT has the ability to precisely deliver high doses of radiation even in large tumour volumes, exploiting the radiobiological advantage of fractionation over a period of 4 days, and thus minimising the risk of serious side effects. Fourth, HDR-BRT for recurrent disease using 192Ir implants through interstitial placed catheters has been shown to improve median survival in selected patients to around 8 months.4 ,29 Fifth, HDR-BRT is a safe method with low complication rates. In our experience, about 10% of the patients undergoing HDR-BRT showed complications, one (2%) bacterial meningitis and two (4%) haemorrhages (one of them with fatal extent) were observed in these patients. These five factors contribute to the safety and feasibility of HDR-BRT in the management of recurrent glioblastoma following primary surgery and radiochemotherapy.
The incidence of radionecrosis was remarkably low in our HDR-BRT group. In studies reporting results of 125I seed implantation, 40–50% manifested symptomatic focal radiation damage. The fact that we used stereotactically implanted catheters which were removed after completion of reirradiation instead of seeds which may slightly migrate over time may play an important role in reducing radionecrosis.
Re-resection still remains in our hands as a very important palliative care for selected patients. The decision to treat with surgery was dependent mainly on whether eloquent brain areas were affected and based on morphology and topography of the tumour progression in relation to speech, motor areas, brainstem and sylvic fissure. Ideally, with technological support (functional MR, diffusion tenson imaging and fibre tracking), we can detect and locate the exact position of brain functions before deciding to perform tumour resection, allowing us to recommend surgery only in those patients with the prospect of radical or grossly subtotal resection. This point is of utmost importance in order to minimise morbidity and mortality and to maximise postoperative quality of life.
Despite the fact that the chance of survival was improved by further surgical treatment or HDR-BRT, early recurrence after gross total removal and radiochemotherapy and early second recurrence after either HDR-BRT or re-resection, remained poor prognostic factors for overall survival in patients with recurrent glioblastoma. Further research should therefore focus on adjuvant treatment after resection of glioblastoma. In fact, many chemotherapeutic agents, either as single agents or in combination, have been used to treat recurrent malignant gliomas. Temozolomide, procarbazin, lomustin and vincristin (PCV) and bevacizumab are some of the treatment options.4 Erlotinib and other epidermal growth factor receptor (EGFR) inhibitors have been studied in combination with radiation therapy.30 A recent study demonstrated the survival benefit of vaccine therapy in relapsed tumours.31 Alternatively, small trials reported that a tumour B cell hybidoma vaccine against tumour stem cells elicited a specific tumour immune reaction, thus enhancing immune response to the disease32 and results from the larger trials might identify a new avenue in the area of adjuvant treatment in the future.
The encouraging results of HDR-BRT including survival prolongation stress the need for randomised phase 2 trials to address the role of HDR-BRT in the recurrent setting.The fact that SRS is not recommended for lesions >40 mm in diameter26 and given the extent of recurrent tumours, constitute HDR-BRT more applicable in this patient population due to the fact that SRS is not recommended for lesions >40 mm in diameter26 and the fulfillment of this restriction would immensely limit patients' eligibility for treatment in extended recurrent tumours.
Weaknesses
Our study design was not without pitfalls: non-randomisation regarding choices of treatment, and selection bias. Patients eligible for surgery may be usually better than those who are not candidates and this may bias the results towards a better outcome. The lack of prospectivity and randomisation condemn this study to low statistical power in demonstrating a benefit of one therapy relative to another. However, a randomised controlled trial might be difficult to conduct given the obvious symptomatic benefits that surgery can provide in many instances and the survival benefits that HDR-BRT has shown in our recent retrospective studies.14 ,15 Another limitation of our study is that data on therapies administered after reoperation or brachytherapy were not included in our analysis. Given the overall lack of efficacy of phase II tested therapies for recurrent gliomas, their contribution to postoperative survival is likely to have been negligible.6 ,33
Conclusions
HDR-BRT achieved in this retrospective study a better survival outcome in comparison to those seen with re-resection or ddTMZ in the treatment of glioblastoma recurrence after primary surgery and radiochemotherapy. Salvage treatment of recurrent GBM remains a challenging issue for neurosurgeons and needs a multidisciplinary approach including radiotherapists and oncologists. However, a persevering attitude is mandatory in the management of glioblastoma to improve the chance of longevity for recurrent disease. The fact that HDR-BRT can be delivered percutaneously under local anaesthesia and mild sedoanalgesia and its relative safety render it a promising treatment option which should be further evaluated in patients with glioblastoma recurrence.
References
Footnotes
-
Contributors EA participated in conception and design. EA and NT participated in acquisition of data. GB, PU, DB and NZ participated in critically revising the article. EA, GB, PU, DB and NZ participated in the reviewed final version of the manuscript and approved it for submission. EA, NT and DB participated in statistical analysis. EA, NT and DB participated in administrative/technical/material support.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethics approval was provided by the Klinikum Offenbach ethics board.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statements No additional data are available.