Article Text

Abstract
Objectives To establish an accurate and comprehensive injury incidence registry of all rugby union-related catastrophic events in South Africa between 2008 and 2011. An additional aim was to investigate correlates associated with these injuries.
Design Prospective.
Setting The South African amateur and professional rugby-playing population.
Participants An estimated 529 483 Junior and 121 663 Senior rugby union (‘rugby’) players (population at risk).
Outcome measures Annual average incidences of rugby-related catastrophic injuries by type (cardiac events, traumatic brain and acute spinal cord injuries (ASCIs)) and outcome (full recoveries—fatalities). Playing level (junior and senior levels), position and event (phase of play) were also assessed.
Results The average annual incidence of ASCIs and Traumatic Brain Injuries combined was 2.00 per 100 000 players (95% CI 0.91 to 3.08) from 2008 to 2011. The incidence of ASCIs with permanent outcomes was significantly higher at the Senior level (4.52 per 100 000 players, 95% CI 0.74 to 8.30) than the Junior level (0.24 per 100 000 players, 95% CI 0 to 0.65) during this period. The hooker position was associated with 46% (n=12 of 26) of all permanent ASCI outcomes, the majority of which (83%) occurred during the scrum phase of play.
Conclusions The incidence of rugby-related catastrophic injuries in South Africa between 2008 and 2011 is comparable to that of other countries and to most other collision sports. The higher incidence rate of permanent ASCIs at the Senior level could be related to the different law variations or characteristics (eg, less regular training) compared with the Junior level. The hooker and scrum were associated with high proportions of permanent ASCIs. The BokSmart injury prevention programme should focus efforts on these areas (Senior level, hooker and scrum) and use this study as a reference point for the evaluation of the effectiveness of the programme.
- PREVENTIVE MEDICINE
- EPIDEMIOLOGY
- SPORTS MEDICINE
- AUDIT
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
Incidence of all catastrophic rugby-related injuries in South Africa between 2008 and 2011 and correlates that accounted for a high proportion of both all and permanent acute spinal cord injuries.
-
This study serves as a reference point for evaluating the effectiveness of the BokSmart programme going forward.
Strengths and limitations of this study
-
The strengths of the paper were the prospective design and comprehensive inclusion criteria for catastrophic injuries.
-
Another strength was the novel statistical comparison and the finding of a higher incidence of catastrophic injury at the Senior level.
-
A weakness of the study was the fact that the player numbers were assumed to have been constant for the entire period of investigation (2008–2011).
Key messages
-
The rate of catastrophic injuries in South African rugby is comparable to other collision sports.
-
Catastrophic injuries occurred more often in Senior than Junior players. The hooker positional grouping and scrum phase of play were associated with high proportions of catastrophic injury.
-
Current findings should guide and focus BokSmart's prevention efforts.
Introduction
While catastrophic events rarely occur in sport,1 the long-term consequences and implicit severity of these events make them the most devastating of all injuries to the player, their family and friends.2 Up until the third decade of life, sport is associated with a large proportion of all catastrophic spinal injuries. Of all sports, collision games such as American Football, Ice Hockey and Rugby account for a large proportion of these sport-related catastrophic events.3–,5 Furthermore, Rugby Union (henceforth ‘Rugby’) is currently the most popular collision sport worldwide6 and has an enormous participant base with 118 active international Unions (http://www.irb.com).
Despite these participation levels, a recent review concluded that the level of risk of suffering a catastrophic injury while playing rugby in the UK was ‘acceptable’ (0.8 per 100 000 participants). Furthermore, this annual incidence was not higher than that of other collision sports such as Rugby League (1.9 per 100 000 participants), Ice Hockey (4.1 per 100 000 participants) or American Football (1.0 per 100 000 participants).1 For South Africa in 2007, the average annual incidence of rugby-related permanently disabling spinal cord injury was estimated to be lower (0.6 per 100 000 participants) than other rugby-playing nations such as New Zealand, Ireland and Australia.1 ,7 Despite these ‘endorsements’ of the relatively low risk of catastrophic injury associated with rugby, an early South African study8 concluded that 56% of all rugby-related spinal cord injuries reported could potentially have been prevented. It is these predictable and preventable catastrophic injuries that are the priority focus for injury prevention strategies.5 ,9
As a result, New Zealand's RugbySmart programme (http://www.nzrugby.co.nz/the_game/safety/rugbysmart) was developed and proved successful in reducing catastrophic injuries.1 ,9 ,10 ,11 Based on this success, the South African Rugby Union (SARU) developed their own programme, BokSmart (http://www.boksmart.com),12 ,13 modelling it on a comparable intervention approach to New Zealand with additional components to suit the South African rugby landscape, making it an example of a national sports organisation intervention.14 Other catastrophic injury prevention strategies for rugby include Rugbyready (International Rugby Board (IRB)), Smart Rugby (Australia) and Tackling Safety (England).1 To evaluate the effectiveness of the BokSmart programme, one first needs to establish the incidence and severity of catastrophic events.15
Therefore, the primary aim of this paper was to establish an accurate and comprehensive injury incidence registry of all rugby union-related catastrophic events in South Africa between 2008 and 2011. An additional aim was to investigate correlates associated with these injuries.
Methods
Data for this study were collected through the BokSmart programme, which is a joint initiative between the SARU (http://www.sarugby.co.za) and the Chris Burger/Petro Jackson Player's Fund (CBPJPF) (http://www.playersfund.org.za). The CBPJPF is a non-profit public benefit organisation, developed to aid players who have been permanently disabled while playing rugby in South Africa.16 Permission to analyse the data was obtained, with SARU and CBPJPF's permission, by the UCT Human Research Ethics Committee.
This is a descriptive study in which injury incidences are described from data that were collected prospectively. Risk factors between players that suffered catastrophic events and those that did not suffer these events were not investigated. The following definitions were adopted for this manuscript (a more detailed description of the game of rugby union is available elsewhere17):
Catastrophic injury
BokSmart and the CBPJPF use the following definition for recording catastrophic injuries:
Any head, neck, spine or brain injury that is life-threatening, or has the potential to be permanently debilitating and results in the emergency admission of a rugby player to a hospital or medical care center.
An event that satisfied the above definition, but was established to be a cardiac-related injury (not head, neck, spine or brain), was also recorded and classified as a ‘cardiac event’. Injuries (includes cardiac events) represented both amateur and professional levels. Catastrophic injuries were classified into three different groups: (1) Acute Spinal Cord Injury (ASCI), (2) Traumatic Brain Injury (TBI) and (3) Cardiac events. ASCIs were further grouped into outcomes, listed in the order of increasing severity: near miss (full recovery expected, ambulant), neurological deficit (some deficit remains, may walk with or without the requirement of assistive devices), quadriplegic and fatal. TBI outcomes were divided into, with increasing severity: fully recovered, disability (remaining neurological deficit) and fatal. ASCIs and TBIs were further grouped into ‘non-permanent’ (near misses/fully recovered) and ‘permanent’ (residual disability, including fatalities). Non-fatal permanent injuries—neurological deficit (ASCI), quadriplegia (ASCI), residual disability (TBI)—would be classified as morbidities and all fatalities would be classified as mortalities.
The outcomes presented are the hospital-confirmed diagnoses within 1 month after the initial injury date as this time frame was thought to be able to provide a more accurate diagnosis.
Incidence
The numerator was calculated as the number of catastrophic injuries and the denominator was the population at risk (total number of rugby players in South Africa). These player numbers were obtained from the IRB website (http://www.irb.com/unions/index.html). Incidences were presented as an annual average (over the 4 year period) per 100 000 players.
Age group
This term distinguished between Juniors and Seniors. ‘Junior’ is synonymous with ‘schoolboy’ in the South African context (under-7 to under-19), and included ‘pre-teen’ and ‘teen’ males and females (as per the IRB website). ‘Senior’ comprised anyone who was not in the definition for ‘Junior’ for males and females (older than under-19) and also included both amateurs and professionals. This term was used to describe the age group of the match where the injury event occurred, regardless of whether the player was legitimately participating in that age group at the time.
Event
This term described the phase of play where the injury occurred and included scrum, ruck, tackle (this included both ball-carriers and tacklers) and collisions (an unintentional or intentional clash—which is distinct from a ‘tackle’).
Positional grouping
Owing to the small sample sizes, the 15 general positions were grouped into nine positional groupings as per Durandt et al18: prop (loose-head and tight head prop; 2 positions), hooker (1 position), lock (left and right lock; 2 positions), loose-forward (open-side flank, blind-side flank and eighth man; 3 positions), scrumhalf (1 position), flyhalf (1 position), centre (inside and outside centre; 2 positions), wing (left and right wing; 2 positions) and fullback (1 position).
Statistics
Incidences with 95% CIs were calculated using the standard formulae19 suggested for rugby union injury studies.20 Incidences were considered significantly different if the 95% CIs did not overlap. Any negative lower 95% confidence limits were presented as ‘0’. To confirm these comparisons using 95% CIs, p values were also calculated for comparisons of Junior and Senior groups using VRP injury statistics software.8 ,21 If a p value was less than 0.05, the difference between groups was considered significantly different, even if the overlap existed between 95% CIs.22
All presented proportions were calculated after excluding missing data (if present) for a particular section—the denominator is always indicated to remove ambiguity.
Results
Since 2008, there have been 54 catastrophic injuries (24 in Juniors and 30 in Seniors) recorded in total in South Africa (table 1), the majority of which (n=45) were ASCIs. In Juniors, the highest number of injuries occurred in 2009 (n=8), while for Seniors the highest number (n=9) occurred in both 2009 and 2010.
Absolute numbers of serious/catastrophic injuries in Junior and Senior Rugby levels in South Africa by year, between 2008 and 2011 (4 years, inclusive)
Owing to the small changes in numbers per year, incidences were calculated on the annual average of injuries over the 4-year period (table 1).
With an estimated 651 146 players at both levels (Junior: n=529 483; Senior: n=121 663) in South Africa, the average annual incidence for all catastrophic injuries (TBI, cardiac events and ASCIs) was 2.07 per 100 000 players (95% CI 0.97 to 3.18). Senior players had a significantly higher incidence of these events (6.16, 95% CI 1.75 to 10.58) than Junior players (1.13, 95% CI 0.23 to 2.04; p=0.03). The average annual incidence for all TBIs and ASCIs combined (excluding cardiac events) was also significantly higher at the Senior level (5.96, 95% CI 1.62 to 10.30) than the Junior level (1.09, 95% CI 0.20 to 1.97) (p=0.03) (combined=2.00 per 100 000 players, 95% CIs 0.91 to 3.08) between 2008 and 2011. In combination, permanent TBIs and ASCIs occurred significantly more often at the Senior level (5.14 per 100 000 players, 95% CIs 1.11 to 9.16) than the Junior level (0.33 per 100 000 players, 95% CIs: 0 to 0.82; p=0.02) between 2008 and 2011 (combined: 1.23 per 100 000 players; 95% CIs: 0.38 to 2.08).
The incidence of TBIs was 0.19 per 100 000 Junior players (95% CI 0 to 0.56) and 0.62 per 100 000 Senior players (95% CIs 0 to 2.01). The incidence of cardiac events was 0.05 per 100 000 Junior players (95% CIs 0 to 0.23) and 0.21 per 100 000 Senior players (95% CI 0 to 1.01). The point estimates calculated for TBIs and cardiac events should be interpreted with caution due to the low numbers of these events (table 1). Half of the TBIs in Junior players (50%, n=2 of 4) had full recoveries, while all outcomes in Senior players (100%, n=3) were fatal. Both cardiac events to date (n=2) had fatal outcomes.
Owing to the low numbers of cardiac and TBI outcomes (n=9), subsequent analyses only focus on ASCIs.
Correlates of ASCIs (TBIs and cardiac events excluded): 2008–2011
All of the ASCIs were sustained by males. Seven per cent of the ASCIs (n=3 of 42) were fatal, 26% (n=11 of 42) resulted in quadriplegia, 31% (n=13 of 42) resulted in neurological deficit and the remaining 36% (n=15 of 42) were classified as ‘near misses’ (outcome not provided in n=3 cases; table 1). Henceforth, for further comparison, outcomes of ASCI were also grouped as either ‘Permanent’ (neurological deficit, quadriplegia, fatal) or ‘Non-Permanent’ (near miss).
The Senior level accounted for 58% (n=26 of 45) of all ASCIs. Considering the population at-risk numbers, the average annual incidence of all ASCIs (including ‘not provided’ outcomes) was significantly higher at the Senior level (5.34 per 100 000 players, 95% CI 1.24 to 9.45) compared with the Junior level (0.90 per 100 000 players, 95% CI 0.09 to 1.70; p=0.04) between 2008 and 2011 (table 2).
Average annual incidences (based on IRB estimated numbers) of acute spinal cord injury (ASCI) from 2008–2011 in South Africa (4 years, inclusive). Incidences include 95% CI
In Senior players, 85% (n=22 of 26) of all ASCIs had permanent outcomes (neurological deficit, quadriplegia or fatal) in comparison to 26% (n=5 of 19) in Junior players. When considering the different numbers for the populations at risk, permanent ASCIs occurred significantly more often in Senior players (4.52 per 100 000 players; 0.74–8.30) than Junior players (0.24 per 100 000 players; 0–0.65; p=0.04; combined: 1.04 per 100 000 players, 95% CI 0.25 to 1.82) between 2008 and 2011 (table 2).
Matches, as opposed to training, were associated with 88% (n=38 of 43) of all ASCIs (information not available for n=2 cases). The training injuries occurred either in a scrum (n=2), tackle (n=2) or ruck (n=1). Owing to the low numbers of training injuries and the fact that their mechanisms were similar to those that occurred in matches, these injuries were combined with match injuries for further analyses (figures 1 and 2).

(A) The phase of play (Collision, Ruck, Scrum or Tackle) that accounted for all acute spinal cord injuries (ASCI) (n=45) and (B) permanent ASCI outcomes at the Junior and Senior levels. Segments add up to 100%.
{kind=link}
{kind=link}
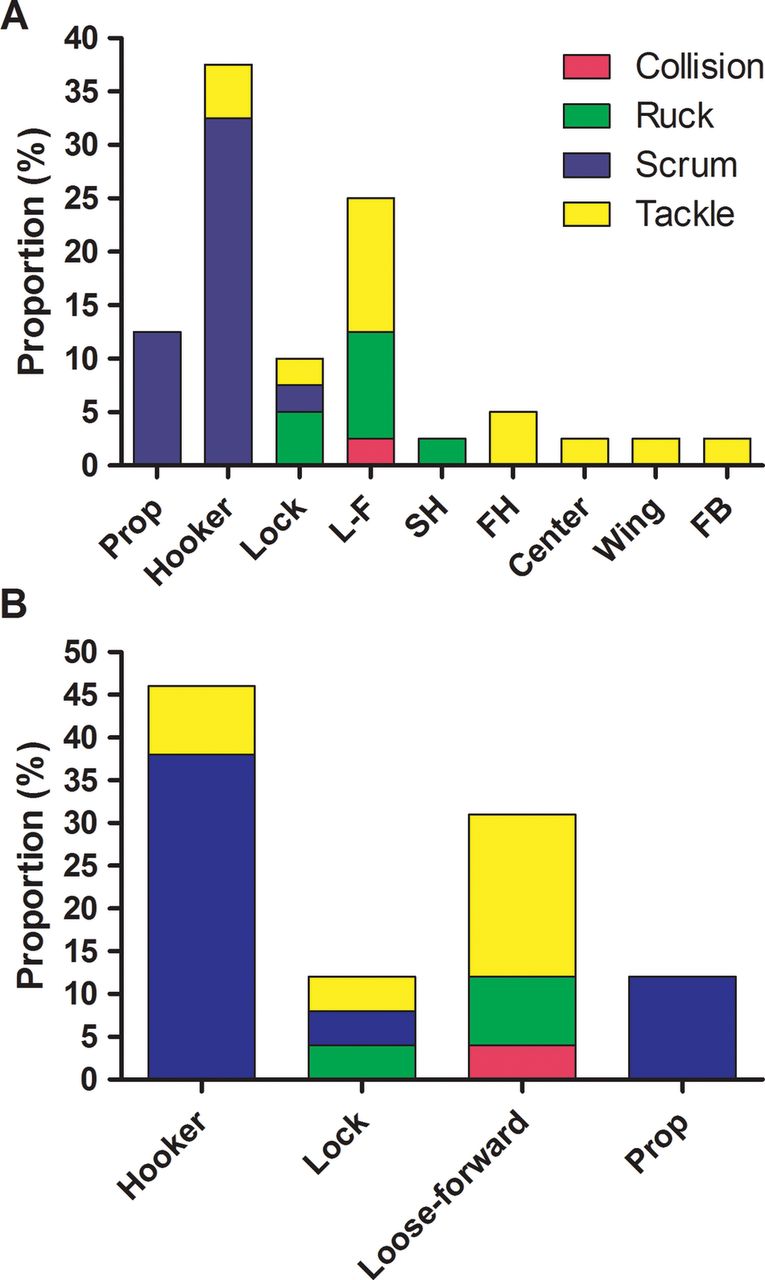
(A) The positional grouping, and the phase of play (tackle, scrum, ruck or collision) that accounted for all acute spinal cord injuries (ASCI) (n=40) and (B) permanent ASCI (n=27) outcomes. For all ASCI outcomes, four cases were excluded from the analysis as three were from seven-a-side rugby and one was from Mini rugby. One case was excluded from both all ASCI and permanent outcomes as the event was ‘unclear’. All segments, in combination, add up to 100%. L-F, Loose-Forward; FH, Flyhalf; SH, Scrumhalf.
The scrum was involved in 42% (n=19 of 45) of all ASCIs. Sixty-three per cent (n=12 of 19) of scrum-related ASCIs occurred to Senior players, which equates to an incidence of 2.47 injuries per 100 000 Senior players (95% CI 0 to 5.26) between 2008 and 2011. Together, the scrum and tackle accounted for 80% (n=36 of 45) of all ASCIs for both levels combined (Junior and Senior; figure 1A). Eighty-two per cent (n=14 of 17; outcome ‘not provided’ for n=2) of scrum-related injuries had permanent outcomes compared with 50% of tackle injuries (n=8 of 16; outcome ‘not provided’ for n=1; table 1B). The 14 scrum-related permanent ASCI outcomes equated to an average annual incidence of 0.54 permanent scrum ASCIs per 100 000 players (95% CI 0 to 1.10) between 2008 and 2011.
The Senior age group accounted for 79% (n=11 of 14) of the permanent scrum injuries and 88% (n=7 of 8) of the permanent tackle injuries. Of all the scrum injuries, scrum engagement and a collapsed scrum contributed to 56% and 39% of cases, respectively (n=10 and 7 of 18, respectively; n=1 case was attributed to popping out, and information was not provided for n=1 case). The tackle events were evenly split between the tackler and ball-carrier (n=8 for each).
For further analyses, only n=40 cases were considered because four cases occurred in positional groupings that are not the conventional 15-a-side rugby (n=3 ‘seven-a-side’, n=1 Mini-rugby) and the event responsible was ‘unclear’ for one case.
The hooker and loose-forward positional groupings were associated with 38% (n=15 of 40) and 25% (n=10 of 40) of all ASCIs (figure 2A). Eighty per cent of all ASCIs to the hooker position were permanent injury outcomes (n=12 of 15). Together, the hooker, prop and lock positional groupings (tight five) accounted for all the scrum injuries. The tackle injuries were shared between all positional groupings except prop and scrumhalf.
When examining permanent ASCIs in isolation (figure 2B), only the forward positional groupings were represented (prop, hooker, lock and loose-forward). Of these permanent outcomes, the hooker alone accounted for 46% (n=12 of 26) of all injuries, 83% of which (n=10 of 12) were as a result of the scrum. The loose-forward positional grouping accounted for 31% (n=8 of 26) of all permanent outcomes, 63% (n=5 of 8) of which came from the tackle.
Discussion
In South Africa, we found that the average annual incidence of all rugby-related catastrophic outcomes (excluding cardiac events) was 2.00 per 100 000 players (95% CI 0.91 to 3.08) between 2008 and 2011. This is comparable to the rate reported for Argentina (1.90 per 100 000 players)23 between 1977 and 1997 and Ireland (0.89 per 100 000 players)5 between 1995 and 2004. These are the only rugby-related catastrophic injury papers that included ‘near miss’ outcomes, and the incidences were only subsequently estimated by a recent review article.1 While the current consensus statement for rugby injury data collection recognises the importance of calculating incidences for comparability across playing nations,20 it still does not include ‘near miss’ outcomes in the definition of catastrophic injury. The small difference between non-permanent and permanent outcomes, and therefore the epidemiological importance of including these outcomes, has been stated by various authors in the past3 ,24 and was clearly illustrated in a recent UK study of spinal injuries in junior players.25
For comparative purposes, the average annual incidence of permanent ASCIs and TBIs was 1.23 per 100 000 players (95% CI 0.38 to 2.08) between 2008 and 2011. On a Health and Safety Executive scale1 which categorises risk in ascending order, from ‘negligible’ (0.001–0.1 cases per 100 000 population) to ‘acceptable’ (0.1–2.0 cases per 100 000 population); ‘tolerable’ (2.0–100.0 cases per 100 000 population); and ‘unacceptable’ (>100 cases per 100 000 population), this incidence would be classified as ‘acceptable’. This average incidence is also comparable to the rates reported in a review of rugby-related permanently disabling head and spinal injuries1 in the UK (0.48–1.50 per 100 000 players), but was on the lower end of rates reported for other countries (0.89–13.00 per 100 000 players) in the same review. However, although this aforementioned review1 intended to include both permanent TBIs and ASCIs, the majority of studies that were included only investigated the latter type of injury.
Therefore, the average annual incidence of permanent ASCIs in the present study (1.04 per 100 000 players, 95% CI 0.25 to 1.82) is the more comparable incidence to those presented in the review.1 The incidence of permanent ASCIs in the present study is also similar to that reported for comparable outcomes in Australia between 1997 and 2002 (3.2 per 100 000 players)26 and New Zealand before (between 1.6 and 3.9, per 100 000 players, per year) and after the introduction of RugbySmart (between 0.8 and 1.7, per 100 000 players, per year).10 The incidence data of New Zealand is particularly believable and accurate due to their comprehensive no-fault insurance system.27 The annual average incidence of the present study is also greater than the estimated incidence of permanent spinal cord injuries for South Africa between 2001 and 2005 (0.6 per 100 000 players),7 although the earlier study had a different method of data collection to that of the present.
For further comparison, the annual average incidence of non-fatal permanent ASCIs (excluding near misses and fatalities) for the present study was 0.92 per 100 000 players (95% CI 0.18 to 1.66), which is significantly lower than the rate reported for comparable outcomes (ASIA scale A–D, excluding fatalities) in Australia between 1995 and 2003 (6.8 per 100 000 players, 95% CI 4.0 to 10.7),28 but comparable to France before (2.1 per 100 000 players, per year) and after the introduction of modified laws and guidelines for the scrum (1.4 per 100 000 players, per year).
The main finding of the present study was the higher incidence of catastrophic injuries at the Senior level, in comparison with the Junior level. This associated factor, along with other relevant factors, is described in the following section.
Senior (as opposed to Junior) level
The novel conclusion of the present study is that the annual average incidence of all (including ‘near misses’) and permanent ASCI outcomes between 2008 and 2011 was significantly higher at the Senior level than Junior level. Although incidences at the Senior level have previously not been statistically compared with those at the Junior level, the preceding literature in Australia26 and France29 have indeed also reported higher incidences in the Senior age group compared with Junior age group. The best comparison to the present study was an American Football study30 that investigated a comparable range of all ASCI outcomes per 100 000 players: fatal to serious, with full recovery outcomes (equivalent to ‘near miss’ in the present study). This American Football study had similar annual average incidences per 100 000 high school and college players, respectively, to the present study: 1.10 (present study: 0.90 per 100 000 players, 95% CI 0.09 to 1.70) and 4.72 (present study: 5.34 per 100 000 players, 95% CI 1.24 to 9.45).
It was interesting to note that this study presents the first documented incidence of catastrophic injury in mini rugby,1 although this injury had a ‘near miss’ outcome.
The reason for the higher incidence rates at the Senior level may, in part, be related to more stringent law variations, in particular with respect to the scrum, at Junior levels.31 Under-19 law variations for the scrum include, but are not limited to: not being able to push a scrum more than 1.5 m and not being allowed to wheel a scrum.32 These law changes decreased the numbers of spinal cord injuries in New Zealand.33 However, the consistent finding that all (non-catastrophic as well as catastrophic) injury incidence rates are higher at the Senior level than Junior level34–36 suggests that this finding is not unexpected. Studies investigating general injuries have suggested that increased speed36 and increased competitiveness and aggression34 ,35 may be responsible for the differences in incidences at these levels. Other factors such as ‘weekend warriors’ (adults only playing sport at the weekend, without sufficient training, coaching and conditioning) and the low numbers of players at the senior level, which could force players to play in unfamiliar positions, are potential contributing factors, although these require further investigation.
Hooker positional grouping
While the many positional groupings of rugby do not allow for statistical comparisons, the hooker positional grouping accounted for the highest proportion of all ASCIs (38%) in the present study, which is alarming considering the small proportion (7%, n=1 of 15) that this position represents in a traditional 15-man starting line-up. Furthermore, this finding and comparison has been made in previous research in South Africa7 and other countries.2 Moreover, this position also accounted for the majority of all permanent ASCIs (46%) in the present study, regardless of the age group, and 83% of these (n=10 of 12) were in the scrum.
While the findings could not be investigated statistically, common sense would argue that the large proportion of ASCIs attributed to this one specific playing position represents an alarming finding that is a matter for concern.
The Hooker's role and position in the scrum could place this player at more risk of suffering scrum-related ASCI than any other positional groupings. During engagement, the hooker has each arm bound around a prop, and is driven into the gap between the opposition hooker and prop by his/her teammates. During this period, and the subsequent shove, there are a number of forces experienced by the front-row including lateral, vertical and compressive. Depending on the level, the compressive forces can be between 8.7 and 16.5 kN.37 At these large impulsive forces, with the hooker unable to adjust his/her position due to the scrum structure, a slight miscalculation or deliberate foul play could result in a catastrophic event to this player.
Scrum (as opposed to any other phase of play)
The scrum alone accounted for a rate of 0.73 ASCIs per 100 000 players and for 42% of all ASCIs. The high proportion of scrum-related catastrophic injuries has previously been shown in South Africa7 and other countries2 ,1 Additionally, there was a higher proportion of scrum-related catastrophic injuries in the present study (42%) in comparison to other studies which also included ‘near misses’, for example, in Ireland (17%, 2 of 12).5
However, studies that only investigated permanent outcomes found that the scrum accounted for 37% (68 of 183) of all cases in South Africa, 51% (19 of 37) of all cases in France, and 61% of all cases in Argentina,23 which were comparable in proportion to that of the present study (52%).
Independently, a higher proportion of scrum compared with tackle-related ASCIs resulted in permanent outcomes (82% vs 50%). Considering that scrums occur relatively infrequently in comparison to tackles and rucks,38 these findings are noticeably understated.
While the hooker, prop and lock positional grouping (tight five) accounted for all the scrum-related permanent ASCIs, the tackle-related injuries were shared between all positional groupings except prop and scrumhalf, which represents the more generalised risk in the latter phase of play. While the incidence was not significantly different between age groups, 79% of all permanent scrum-related ASCIs occurred at the Senior level rather than the Junior level. The engagement sequence accounted for the largest proportion of scrum-related injuries (56%) in the present study, which is consistent with previous findings,2 ,39 and has been attributed to the high forces experienced by the front row during this phase of the scrum.29 ,40 The high forces (and thus acceleration) during engagement would exacerbate any predisposing risk factor.
The premature degeneration of the cervical spine, particularly in front row players,10 ,41 mismatches in size between front-row players,2 ,12 and high impact forces40 ,42 have been mentioned as potential factors for the relative over-representation of scrum-related injuries in the previous literature, but other factors such as refereeing experience, coaching experience, scrum laws, technical preparation, appropriate player selection and specific conditioning of players should also be scrutinised more carefully.
While the four phase ‘crouch, touch, pause, engage’ refereeing sequence has been shown to have some positive effect on injury incidences,39 the results of the present study warrant considering further law changes with potentially greater effect, especially for the amateur game. The modification of scrum laws/regulations in amateur rugby in France: removal of the high impact on engagement, linking the two packs together before the scrum commences and a ‘rugby passport’ licence to certify the capacity of front-row players significantly reduced scrum-related catastrophic cervical spine injuries, including those to the front-row and hooker positions.29 Furthermore, the exemplary nationwide injury prevention programme of New Zealand, RugbySmart, had a significant reduction in scrum-related spinal injuries,10 and it is hypothesised that the BokSmart programme can produce a similar effect over time.12 This paper serves as a reference point for the BokSmart programme going forward.
Although all ASCIs occurred to males in the present study, this may simply be an artefact of disproportionate participation levels: there are only 17 917 females in comparison to 633 229 males (http://www.irb.com/unions/index.html).
The average annual incidence of cardiac death rates in the present study in Junior players (0.05 per 100 000 players) is less than the rates published previously for competitive athletes younger than 18 years of age.42 There were no prospective incidences available for adult/senior populations.
Limitations
Player numbers were assumed to remain constant over the 4 years of investigation. While they may have fluctuated between years, it is unlikely that the numbers have declined appreciably, thereby ensuring that incidences were not underestimated. The estimation of player numbers (population at risk) may also be open to error. However, owing to the fact that these rare events are shown as an incidence per 100 000 players, the inaccuracy would have to be enormous to affect the results presented in the current study. Furthermore, errors in numbers would probably be consistent at both levels (Junior and Senior) and should not drastically affect between-level comparisons.
It is plausible to suggest that some catastrophic events might not be reported to BokSmart and the CBPJPF. However, the Serious Injury Protocol, and the potential benefit of financial assistance that is associated with reporting injuries in South Africa, would make this possibility very small. Information dissemination via social media and other more formal communication channels regarding catastrophic rugby injuries would generally pick up any shortfall potentially missed.
Conclusion
In conclusion, the rates of all (including near-miss) and permanent (excluding near-miss) rugby-related ASCIs in South Africa from 2008 to 2011 are comparable to the rates in most other countries and to the rates in other collision sports such as American Football. Despite this finding, three factors were strongly associated with catastrophic injury and warrant further attention for prevention strategies: Senior players, hooker playing position and the scrum phase of play. This 4-year registry will serve as a reference point for the evaluation of the BokSmart injury prevention programme going forward.
Acknowledgments
The authors would like to thank the board of the Chris Burger/Petro Jackson Player's Fund (CBPJPF) and especially the former Springbok captain, Morne Du Plessis, for his foresight in initiating the fund. The authors would also like to thank Ms Gail Ross, in her current position as Serious Injury Case Manager, for her dedication and effort in collecting the information that has been presented in this study.
References
Footnotes
-
Contributors JB was granted access to analyse the data, was involved in conceptualising the manuscript, conducted statistical analyses and wrote the initial drafts of the manuscript. He is also the guarantor. CR and WV collected and entered the data. All authors (ML, EV, CR, WM and WV) were involved in conceptualising and editing drafts of the paper, in the order that they appear on the author list.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Ethics approval UCT Human Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Depersonalised data are available at the following URL: http://images.supersport.com/Website%20Serious%20injury%20table%20updated%2031%20December%202011.pdf. Owing to the sensitive nature of the information and appropriate medical ethics, access to a more detailed aspect of the available dataset will be reviewed upon request and on a discretionary basis. Sharing of only depersonalised and non-relatable data will be considered, once permission has been received from WV or CR (can be contacted through the corresponding author).