Article Text

Abstract
Objectives The aim of this study was to assess the risk of incident rheumatological diagnoses (RD) associated with self-reported diarrhoea and vomiting during a first-time deployment to Iraq or Afghanistan. Such an association would provide evidence that RD in this population may include individuals with reactive arthritis (ReA) from deployment-related infectious gastroenteritis.
Design This case–control epidemiological study used univariate and multivariate logistic regression to compare the odds of self-reported diarrhoea/vomiting among deployed US military personnel with incident RD to the odds of diarrhoea/vomiting among a control population.
Setting We analysed health records of personnel deployed to Iraq or Afghanistan, including responses on a postdeployment health assessment and medical follow-up postdeployment.
Participants Anonymous data were obtained from 891 US military personnel with at least 6 months of medical follow-up following a first-time deployment to Iraq or Afghanistan in 2008–2009. Cases were defined using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis codes; controls had an unrelated medical encounter and were representative of the study population.
Main outcome measures The primary measure was an association between incident RD and self-reported diarrhoea/vomiting during deployment. A secondary measure was the overall incidence of RD in this population.
Results We identified 98 cases of new onset RD, with a total incidence of 161/100 000 persons. Of those, two participants had been diagnosed with Reiter's diseasei (3.3/100 000 persons) and the remainder with non-specific arthritis/arthralgia (157.5/100 000 persons). The OR for acute diarrhoea was 2.67 (p=0.03) after adjusting for important covariates.
Conclusions Incident rheumatological conditions, even those classified as ‘non-specific,’ are significantly associated with prior severe diarrhoea in previously deployed military personnel, potentially indicating ReA and need for preventive measures to reduce diarrhoeagenic bacterial exposures in military personnel and other travellers to the developing regions.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
Use of self-reported gastroenteritis instead of medical encounter data or culture-confirmed infectious gastroenteritis enabled inclusion of a larger portion of personnel potentially exposed to pathogens of interest.
-
Extraction of data from a health assessment completed by all military personnel returning from deployment allowed access to a large pool of respondents.
-
Broadly defining reactive arthritis by the specific and non-specific International Classification of Diseases, Ninth Revision, Clinical Modification codes increased the sensitivity.
-
Each of these study design decisions introduced the possibility of non-differential biases, including exposure misclassification, recall bias and outcome misclassification. This would likely bias the associations towards the null.
Introduction
Travellers’ diarrhoea (TD) is common among those travelling from the developed to the developing regions of the world. Incidence is broadly estimated at 20–40% of travellers per month but varies by country or region visited, duration of travel and sociodemographic factors.1–3 The aetiology of TD is predominantly bacterial, commonly caused by diarrhoeagenic Escherichia coli, Campylobacter spp., Shigella spp. and non-typhoidal Salmonella spp., although viral and parasitic infections also occur.3–5 While the acute symptoms associated with TD are predominately self-limited and may be shortened in duration by antibiotic therapy, sequelae associated with infection by pathogens of TD can cause long-term gastrointestinal, neurological and rheumatological health outcomes.6–8
Reactive arthritis (ReA) is a sterile asymmetric arthritis of one or more joints that can include inflammation of the tendons, eyes, genitourinary tract and skin.9 Joint inflammation is most common in the large joints of the lower limbs.9 ,10 The most strongly associated enteric bacteria are Campylobacter jejuni and coli, non-typhoidal Salmonella spp, Shigella spp and Yersinia enterocolitica.9–13 Reports of ReA following bacterial gastroenteritis are most common following large-scale outbreaks, and estimates of incident ReA outcomes range from 0% to 30% depending on the infecting pathogen, host characteristics, outcome definitions and other factors.10 ,14
Deployed military personnel represent a young, predominately healthy subset of the general travel population at high risk of TD and, potentially, of related sequelae. Given the prior reports of an increased risk of functional gastrointestinal disorders following infectious gastroenteritis during military deployment and a twofold increased risk of Reiter's diseasei and postdysenteric arthropathy among personnel deployed to high-risk regions, we sought to assess the risk of incident rheumatological diagnoses (RD) associated with self-reported diarrhoea and vomiting during a first-time deployment to Iraq or Afghanistan.15 ,16
Methods
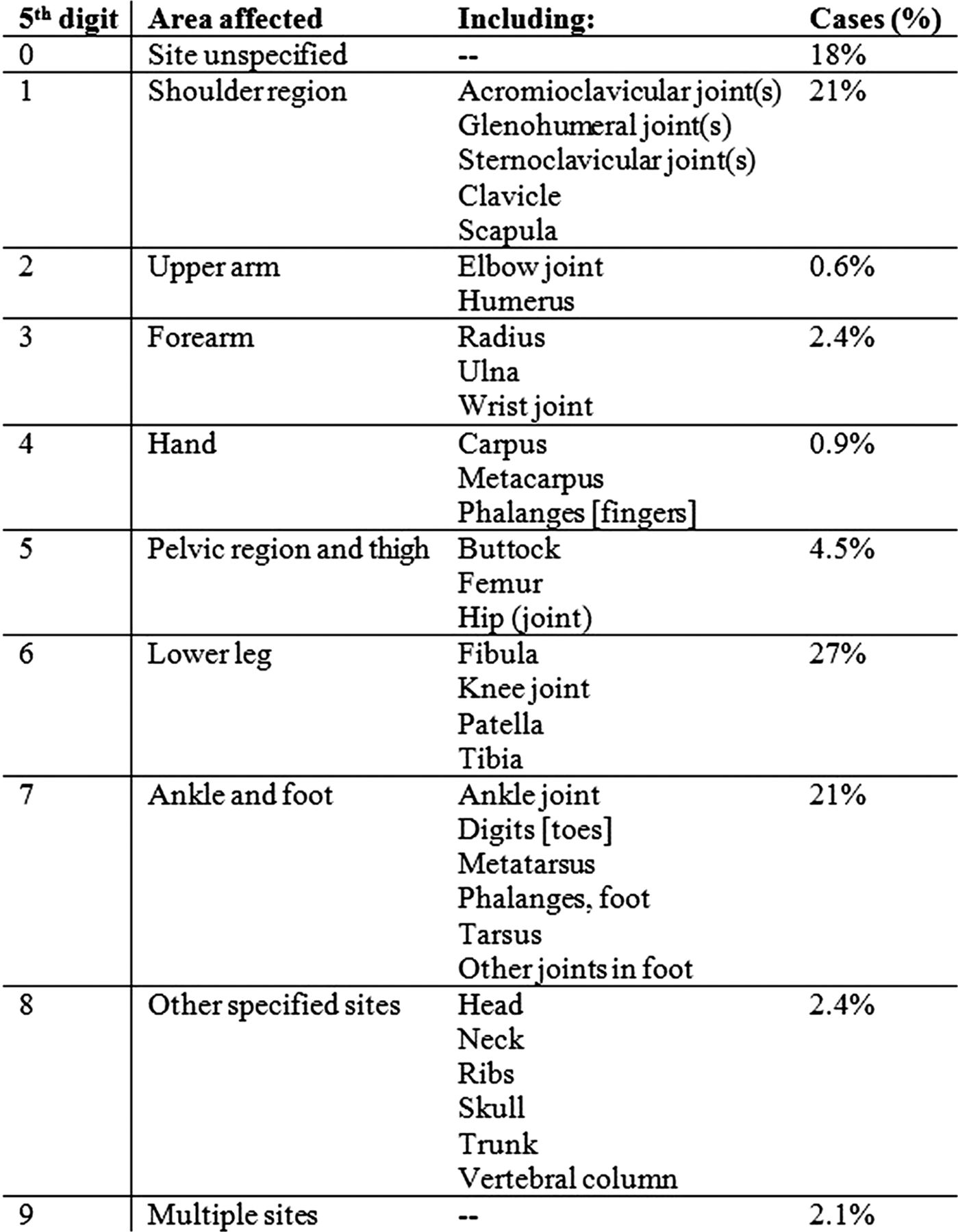
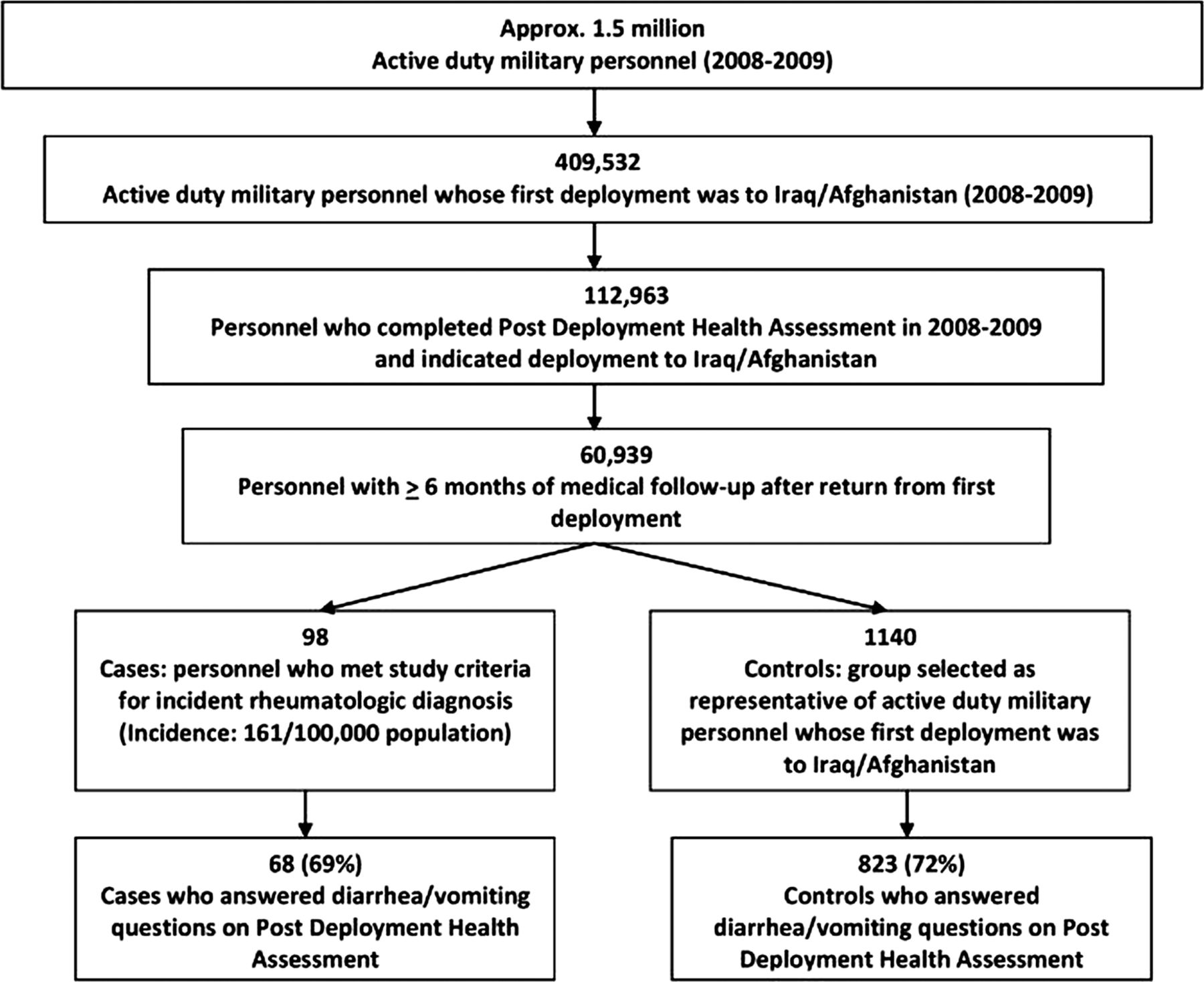
A case–control study of military personnel was designed to compare the odds of self-reported diarrhoea or vomiting during deployment among personnel with incident RD (cases) to the odds among those without such diagnoses (controls). All participants were active duty US military personnel on initial deployment between 2008 and 2009 with at least 6 months of postdeployment medical follow-up (figure 1). Cases were identified using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes for Reiter's diseasei (099.3 and 711.1), postdysenteric arthropathy (711.3) and, due to the confounding factors underlying Reiter's diseasei diagnoses, a category of non-specific arthritis/arthralgia (NAA) was included (716.4-.6, 716.8-.9).10 ,16 ,17 The ICD-9-CM codes for postdysenteric arthropathy and non-specific arthritis/arthropathy include a fifth digit subclassification indicating the body area affected (figure 2). Cases required a minimum of two separate outcome-specific medical encounters within 365 days with no concurrent diagnoses of Chlamydia trachomatis, Neisseria gonorrhoeae or Ureaplasma urealyticum. Controls were of a similar age, deployment location (Iraq or Afghanistan), had an unrelated medical encounter and were representative of the study population.

Schema of selection for analysis.
{kind=link}
{kind=link}
Fifth digit subclassification of body area affected.
All data were obtained from the Defense Medical Surveillance System (DMSS), a repository for medical surveillance data on US military personnel.18 Demographic variables, including age, gender, race, rank and marital status were analysed to assess their association with incident RD. Because acute enteric infections are under-reported through electronic medical records, exposure data were obtained from postdeployment health assessments (PDHAs), a self-administered survey completed by all US military personnel returning from deployment. Of specific interest for this study were questions about diarrhoea and vomiting during deployment. Respondents indicated whether during deployment, they had seen a healthcare provider for and/or had been ordered to remain in their quarters (bed rest) or placed on medically restricted duty status (light/limited duty) for diarrhoea or vomiting. Personnel who consistently did not respond to the exposure questions were excluded from the case–control analysis; for those who answered at least one exposure question, we considered missing responses as ‘no’ responses.
The incidence of RD was calculated based on the number of active duty US military personnel eligible for inclusion into this study. Multivariate logistic regression models were developed utilising a backward elimination approach in which all covariates were initially included. The final adjusted model was developed iteratively for the outcome of any diarrhoea or vomiting during deployment, and only variables with α ≤ 0.15 were retained. The final model was then applied to each exposure strata. Reference groups were chosen based on prior epidemiological studies as well as distribution of our data. Statistical analyses were conducted using SAS V.9 for Windows (SAS Institute, Cary, North Carolina, USA) and interpreted using α=0.05.
The study protocol was approved by the Naval Medical Research Center Institutional Review Board in compliance with all applicable Federal regulations governing the protection of human participants.
Results
We identified 98 cases of new onset RD among active duty military personnel with an initial deployment to Iraq and/or Afghanistan between 2008 and 2009 for a total incidence of 161/100 000 persons (figure 1). Two cases were diagnosed with Reiter's diseasei (3.3/100 000 persons) and the rest with NAA (157.5/100 000 persons). Of the nine possible subclassifications, the most frequently specified body areas affected were lower leg (27%), shoulder (21%) and ankle/foot (21%); 18% of diagnoses did not specify a body area (figure 2). The remaining 13% were composed of pelvic region/thigh (4.5%), forearm (2.4%), hand (0.9%), upper arm (0.6%), and other (2.4%) or multiple (2.1%) sites.
Excluding primary exposure non-respondents (ie, those who did not answer gastroenteritis questions) yielded 891 participants: 68 cases and 823 controls (figure 1). Overall, 28% of original participants were non-respondents: 31% of cases and 28% of controls. As intended, there was no difference in the average age of cases or controls (mean 27.6 years; SD 6.8; table 1). Compared with controls, cases were more predominately male (94% vs 70%; p<0.001) and tended to be married (60% vs 48%; p=0.06). The prevalence of self-reported gastroenteritis was relatively low across deployments (19.4%; table 2). However, personnel deployed to Afghanistan reported diarrhoea and/or vomiting more often than those deployed to Iraq (37% vs 17%, p=0.01).
Demographic and exposure characteristics of US military service members after their first deployment to Iraq or Afghanistan between 2008 and 2009
Frequency (n (%)) of self-reported, deployment-related exposures by deployment region (excluding six personnel deployed to both regions)
Univariate logistic regression showed that male gender (p<0.001) and rank (p=0.01) were associated with increased incidence of rheumatological outcomes (table 3). A greater per cent of cases than controls reported care-seeking (23.5% vs 15.2%; p=0.07) and being assigned light/limited duty (10.3% vs 5.0% p=0.07) for diarrhoea. Black or white race (p=0.15), junior officer rank (p=0.11) and being married (p=0.06) were also more common among those with RD. After adjusting for covariates, the prevalence of diarrhoea and vomiting was consistently higher among cases than among controls (table 4). In personnel reporting more severe diarrhoea (eg, being sick-in-quarters or placed on light/limited duty), there was an approximately 2.5-fold increased odds of RD compared with those who did not (aOR 2.67; p=0.03). Although the association with milder diarrhoea was not statistically significant, there was a trend suggestive of a dose–response effect. Self-reported vomiting was not a significant predictor of incident RD.
Unadjusted conditional ORs (95% CIs) for exposure variables and covariates from univariate analysis evaluating RD after first deployment to Iraq or Afghanistan between 2008 and 2009
Adjusted* ORs (95% CIs) for exposure variables from multivariate analysis evaluating incident RD after first deployment to Iraq or Afghanistan between 2008 and 2009
Discussion
We found that 16% of deployed service members sought care for diarrhoea, 38% of whom required a change in duty as a result of the acute illness. This is much lower than prior estimates of gastroenteritis in deployed military personnel.19 ,20 Specifically, Sanders et al19 found in 2004 that 77% of US personnel who served in Iraq and 54% of those deployed to Afghanistan reported any diarrheal illness; nearly half of those with diarrheal illness had sought care. Differences in study methods may have contributed to this difference. Use of a post-deployment questionnaire in our study is likely to have resulted in under-reporting of exposure, while Sanders et al utilised active case-surveillance through mid-deployment and post-deployment surveys to identify diarrheal cases. However, this could also indicate a true decrease in incidence due to decreased risk in theatre, which has been reported in a previous publication.21
We identified an overall incidence of RD of 161/100 000 (Reiter's diseasei: 3.1/100 000 and NAA: 157.5/100 000), similar to estimates reported by Curry et al.16 These estimates are greater than those from population-based studies within the USA, likely due to differences in study populations and methods utilised to classify exposures and outcomes.11 In addition, exposure to specific bacterial pathogens in deployed populations is likely more common than in the developed countries, where viruses are the dominant cause of acute gastroenteritis.3 ,22 ,23 Importantly, the body areas affected, primarily the lower leg, are consistent with other reports of ReA.10 ,14 ReA is known to commonly occur in multiple joints at once, but clinicians may have chosen to specify only one body area because it was the body area worst affected or because it was the body area in which the condition had persisted until that medical encounter.14
We found a nearly threefold increased risk (aOR 2.67, 95% CI 1.11 to 6.47) of exposure to severe diarrhoea during deployment for RD, elaborating on the findings by Curry et al16 of associations between prior infectious gastroenteritis and/or deployment to high-risk regions and Reiter's disease or NAA. Using the same outcome definitions, Curry et al reported an adjusted OR (aOR) of 1.76 (95% CI 1.49 to 2.07) for NAA risk in those with documented infectious gastroenteritis compared with those without.
The incidence of RD in this study was higher than in population-based studies, but possibly lower than the incidence in all deployed personnel due to our relatively young study population. Our sample was limited to personnel on first-time deployment, yielding a mean age of 27.6 years (SD 6.8); this is lower than the average age of ReA diagnosis in the general population (30–40 years).10 Curry16 observed that the rates of NAA and ReA increased significantly with age. In a prospective study of culture-confirmed Campylobacter, E coli O157, Salmonella, Shigella and Yersinia infections among patients >1 year, Townes et al14 observed a median age of 41 years among individuals with confirmed ReA. If younger persons are less likely to develop ReA, our incidence estimate may be lower than the incidence of ReA among all deployed service members and the broader travel population.
Although these data may not be directly generalisable to every travel population, our findings highlight ReA as an important TD sequela among travellers who stay for long periods in the developing regions of the world where bacillary diarrhoea is common. However, this study should be interpreted with a full appreciation of the inherent limitations. In using self-reported gastroenteritis instead of medical encounter data or culture-confirmed infectious gastroenteritis, we were able to include a larger portion of personnel potentially exposed to the pathogens of interest. This is especially important because medical encounter data in the deployment setting are not routinely recorded in electronic medical records capable of being linked with ambulatory and inpatient medical encounters. However, by using this exposure definition, we may have included an undefined number of non-bacterial gastroenteritis episodes resulting in exposure misclassification—likely non-differential and thus biasing towards the null. In addition, utilising data collected at the end of deployment, potentially months after the gastroenteritis episode, opened the study to non-differential recall bias. Similarly, broadly defining ReA by the specific and non-specific ICD-9-CM codes increased sensitivity, but likely increased outcome misclassification. ICD-9-CM codes are useful for health surveillance but have several known sources of error and variance which impact data reliability.24 ,25 Using the surveillance data available from the DMSS expanded our access to potential research participants and their records. However, response rates, particularly to the questions of interest in this study, were poor. Only 69% of cases and 75% of controls answered the gastroenteritis questions and the rest could not be included in case–control analyses. This design allowed us to examine the risk of ReA in active duty military personnel, a group of people who have a high rate of gastroenteritis and whose risk for ReA has not been well studied.
Further research is needed to define the incidence, risk factors, duration and costs of ReA in active duty military personnel and other travel populations. Improved characterisation of incidence and risk factors can be accomplished with study designs targeting more well-refined diagnoses of ReA and postdysenteric arthropathy, case-finding that does not depend on ICD-9-CM codes and more specific measures of bacterial gastroenteritis during travel than are available through the PDHA. In a US military population, a longitudinal study could utilise duration and cost of illness data extracted from the DMSS. Our study suggests that a significant proportion of individuals with ReA may currently be categorised as having NAA. This possibility should be investigated by clinically examining patients in a variety of target populations who have been diagnosed with NAA to determine whether they have ReA. Prospective studies expanding the work of Townes et al are warranted to further study individuals from the time they are diagnosed with infectious gastroenteritis through the time when some develop ReA.14 Consistent pathogen-specific attributable risk estimates are also needed to elaborate on the burden of ReA that could be eliminated through improved bacterial gastroenteritis prevention.
We have shown an increase in incident RD in active duty military personnel following severe diarrhoea during deployment to Iraq and/or Afghanistan. Even in a population of cases primarily diagnosed with NAA, there was a significant association with self-reported diarrhoea during deployment. This seems to confirm that a proportion of cases were experiencing ReA. Because our study population primarily represented younger military personnel and ReA is most common in 30-year-olds and 40-year-olds, the true incidence of ReA in active duty military personnel and the broader travel population may be higher than our estimate. Carefully designed future studies will help to further characterise the risk factors of ReA and its long-term health consequences and to identify interventions that could reduce the burden of chronic sequelae in at-risk travellers.
References
Footnotes
-
Contributors CKP and MSR designed the study and acquired the data. KHDY and CKP conducted the data analysis and interpretation. KHDP and CKP are guarantors of this manuscript. KHDP, CKP, MSR and LM collaborated in the interpretation of results and writing of the manuscript. All authors revised it critically for intellectual content and have given final approval of the version of the manuscript submitted.
-
Funding This study was conducted under support of the Military Infectious Disease Research Program and Department of Defense Global Emerging Infections Surveillance and Response System funding.
-
Competing interests None.
-
Ethics approval Naval Medical Research Center IRB.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.
-
↵i The terms Reiter's disease and Reiter's syndrome are being replaced with the more appropriate term Reactive Arthritis. Usage in this article strictly refers to their use in the International Classification of Diseases, Ninth Revision, Clinical ModificationICD-9-CM diagnostic codes (099.3 and 711.1) and is not an endorsement of the terms.