Article Text

Abstract
Objectives We aimed to conduct a meta-analysis of human papillomavirus (HPV) as a risk factor for oesophageal squamous cell carcinoma (OSCC) in China, using all eligible studies published in the English and Chinese language literature.
Design The random effect model was used to analyse the pooled OR. The I2 and Q tests were included in the subgroup analyses.
Setting Literature searches of databases including MEDLINE, PUBMED, EMBASE and Chinese National Knowledge Infrastructure (CNKI) and other available resources were performed to retrieve studies investigating OSCC tissue from Chinese participants for the presence of HPV DNA.
Primary outcome measure A collective analysis of OSCC cases and control specimens was carried out from 15 case–control studies (6 in the English language and 9 in the Chinese language) for HPV prevalence.
Results Of a total of 1177 OSCC and 1648 oesophageal control samples, 55% (642/1177) of cancer specimens and 27% (445/1648) of control samples were positive for HPV DNA. A positive strong association between HPV DNA and OSCC was observed among the included studies, with a pooled OR of 3.69 (95% CI 2.74 to 4.96). Heterogeneity and publication bias were not observed in the analysis. Subgroup analyses of the included studies also supported the measure of association of causal links between HPV and OSCC.
Conclusions This meta-analysis provides the strongest evidence until now of an association between HPV and OSCC in the Chinese population. China has a high burden of OSCC, making this an important research finding. A strength and new contribution of this study is combining data from the English and Chinese language literature to analyse all studies conducted in China. These findings may inform the population level use of prophylactic HPV vaccination to reduce the burden of OSCC in China.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
The use of observational epidemiological studies in the meta-analysis.
-
Other limitations may include the inclusion of heterogeneous and small-scale studies, and the inter-laboratory variation of methodology between studies for HPV detection.
-
The study pertains to the inclusion of only the most appropriate study design (case-control methodology) in the analysis, and for the first time, the inclusion of studies published in both the English and Chinese languages, thereby providing a more comprehensive evidence base than previously available.
Introduction
Oesophageal carcinoma (OC) is the eighth most common malignancy in the world with an estimated incidence of 500 000 new cases annually.1 Oesophageal squamous cell carcinoma (OSCC) is the most common histological type of OC. There is a large variation in the incidence rates of OSCC between countries as well as between different regions of the same country. China has the highest global burden of disease from OSCC.2 An annual incidence of approximately 250 000 cases are reported in China alone3 ,4 with a national average incidence rate of 13/100 000.4 OSCC represents more than 99% of all OC cases in China.5 In 2008, it was reported that oesophageal malignancy was responsible for 406 000 deaths worldwide, making it the sixth highest cause of cancer-related deaths.1 In China, OSCC causes 150 000 deaths a year and is the fourth leading cause of all cancer-related deaths.6 ,7
The multifactorial aetiology of OSCC is thought to contribute to its highly variable incidence around the world. There have been reports of up to a 500-fold variation in the incidence of OSCC between low-risk and high-risk regions across the globe, with China being one of the highest risk regions in the world.8 ,9 Even within China, however, there are large regional variations in the incidence of OSCC, thought to be due to variations in cofactors such as diet and environmental risk factors.4 ,10–12 Established risk factors for OSCC include smoking and alcohol, but a range of other risk factors have also been identified.13–19 Human papillomavirus (HPV) as a risk factor for OSCC was first suggested in 1982,20 with detection of HPV DNA in OSCC tissue ranging from 15% to 80% globally.21
HPV is the one of the most significant infectious causes of cancer, particularly cervical cancer.8 ,22 The main oncogenic HPV genotypes are HPV 16 and 18, which, other than being the cause of cervical cancer, have been implicated in malignant tumours of the head and neck and oropharyngeal and anogenital cancers.2 ,8 ,22 It has been estimated that HPV is responsible for 5.1% of the global cancer burden.22 One cancer in which the role of HPV has been widely studied, but not resolved, is OSCC.
China has one of the highest rates of HPV prevalence in OSCC of 41.8% compared to 10.1% in the USA/Canada, 17.7% in Europe and 39.6% and 30% in South Africa and South America, respectively.23 Despite the high overall rate of HPV detection in OSCC in China, different studies have found a geographical variation in the rates of HPV in OSCC, possibly a real variation, but possibly in part reflecting the different detection methods used.19 ,10 However, a recent study found no significant impact of the different detection methods on the detection rates of HPV.23 This complexity and the high disease burden of OSCC in China highlight the need to better understand the relationship of HPV to OSCC in China.
Questions of aetiology are best addressed using case–control methodology, but relatively few case–control studies have been conducted on HPV and OSCC.19 We previously conducted a global meta-analysis of the few case–control studies published in the English language literature and showed a strong association between HPV and OSCC across all regions of the world.24 This study showed that the association, while consistent, varied in magnitude across regions of high and low OSCC incidence. As such, it is important to further study the association in the country with the highest burden of OSCC, China. We aimed to conduct a meta-analysis of all published case–control studies in China from the English and Chinese language literature, to determine the association between OSCC and HPV infection in the Chinese population.
Methods
Literature search
Searches of the English and Chinese language databases including MEDLINE, PUBMED, EMBASE and CNKI were carried out by investigators to retrieve case–control studies investigating OSCC tissue from Chinese participants for the presence of HPV DNA, as published in peer-reviewed journals. Search terms included “human papillomavirus”, “HPV”, “oesophageal neoplasms”, “carcinoma, squamous cell” and “China”. Only English and Chinese language papers were included. There were no restrictions placed on the date of publication and studies were sourced from the earliest available papers on the databases up to February 2012. Reference lists of all case–control studies obtained were reviewed and relevant English language journals, including Lancet Oncology, Annals of Oncology, Gastroenterology, International Journal of Cancer, BMC Cancer, Diseases of the Esophagus, Anticancer Research, Cancer Epidemiology Biomarkers & Prevention and Journal of Clinical Pathology, were hand searched for any articles which may not have been electronically indexed. In addition, a search of the grey literature did not produce any further relevant data for our analysis.
Selection criteria
All English language papers were retrieved by one of the authors (SSL) and each paper was reviewed independently by two authors (SSL and IR). Chinese language papers were sourced by a third collaborative party and reviewed by two of the authors who are fluent in Mandarin Chinese (ZG and YZ). Only studies which compared OSCC tissue (cases) and normal oesophageal tissue from healthy participants (controls) in Chinese populations, for the presence of HPV DNA, were included in this meta-analysis. Case series and reports describing morphological evidence, animal models, serological and in vitro studies on this topic were excluded. This meta-analysis reports on a collective analysis of 1177 OSCC and 1648 control specimens from the 15 identified case–control studies (9 Chinese language and 6 English language). Our previous global meta-analysis included only the six studies published in the English language.24
A confirmed histological diagnosis of OSCC was required for classification of participants as cases. Controls were identified as healthy individuals with no significant past or concurrent chronic illness. As endoscopy is not widely utilised across China to investigate discomforts such as gastro-oesophageal reflux symptoms, control participants recruited to a majority of the identified case–control studies were volunteers with no medical requirement for endoscopy. Any studies which classified control tissue as tumour-adjacent tissue, which appeared macroscopically normal in OSCC cases, were excluded from our analysis.
Data extraction
Relevant data from the 15 case–control studies were extracted and summarised in table 1 as follows
-
General information—Name of first author, year of publication, region of China;
-
Study design—Case–control methodology, HPV detection method(s) utilised, number of cases and controls studied;
-
Exposure assessment—Types of HPV detected;
-
Findings—Number of HPV-positive cases and controls detected;
-
Analysis—Methodology, if any, of adjustment for confounding factors, calculation of ORs with 95% CIs and p values.
Case–control studies examining HPV DNA in OSCC*
Quality assessment
A quality assessment tool (quality scoring form) which we developed previously in our global meta-analysis on HPV and OSCC was used for this study, and is published as a supporting document with the paper.24 This standardised scoring instrument, to assess the quality of each case–control study, was designed by the authors to account for issues specific to case–control methodology based on guidelines for evaluation of observational studies25–27 and incorporating clinical and epidemiological knowledge of HPV and OSCC.
The scoring instrument consisted of four main domains of quality assessment adding up to a total of 100 points: selection of participants (40 points), measurement of exposure (HPV) and outcome (OSCC; 40 points), adjustment for confounding factors (15 points) and data analysis (5 points). Each of the 15 case–control studies included in our analysis was evaluated against these categories of quality assessment and the final score assigned to each study reflected the general quality of the study. The sections assessing selection and measurement were allocated the highest possible scores, as these are areas of relatively greater significance in observational studies. The analysis section received the lowest weighting based on the rationale that a study which scores well in the other three areas of quality assessment could potentially have the data reanalysed if required.
The scores for the four main categories of quality assessment were comprised of weighted subsections. For example, within the measurement section, the methodology for evaluation of exposure (HPV) was allocated 65% of the total section score while the remaining 35% was ascribed to measurement of outcome (OSCC). This is primarily because, for a study which aims to assess the aetiological role of HPV in a given disease, the methods used to ascertain HPV involvement are vital to the validity of the study.
A detailed written guide and instructions on how to complete the form were attached to the quality assessment instrument. All case–control studies which met the inclusion criteria for the analysis were individually and independently scored by four blinded assessors (SSL, IR, ZG and YZ). The six English language papers were scored by SSL and IR while the remaining nine Chinese language papers were scored by ZG and YZ. Summary information from the nine Chinese language papers was translated into English by ZG and YZ for consideration by all authors. Once all the papers had been assessed, any discrepancies in the answers were identified and discussed between the scorers to reach consensus on the single best option. Any points of assessment on which the scorers could not reach an agreement were resolved by a third scorer (BR). In order to determine the degree of variation in responses between the four scorers, we carried out calculations of interobserver correlation. This scoring tool was validated in our previous meta-analysis and it demonstrated a very good reliability with an intraclass correlation (ICC) of 87% for the total quality.24
Statistical analysis
The average scores for quality domains were calculated via Excel.28 The SPSS (version 20.0) software program29 was used for calculation of ICC coefficients which provided information on the degree of interobserver agreement. Stata V.10.1 SE30 was used for all other statistical analysis. The random effects model was utilised to pool ORs for the 15 case–control studies. The I2 and Q tests were the statistical methods used to assess heterogeneity between studies.
Of the 15 studies included in our analysis, only four papers reported an OR.31–34 Therefore, we carried out calculations of effect estimates for all studies, based on the data provided in the papers. Only one study by Li et al35 had an OR which was incalculable as a result of a zero value for one of the four variables (a, b, c and d) used in the calculation of OR. In accordance with the standard measures for meta-analysis in such cases, a value of ‘0.5’ was added to each of the four cells in the 2×2 table to enable calculation of an OR for this study.36 Analysis of the Li et al35 study was carried out separately to the remaining 14 reports to determine whether manipulation of the data, which was necessary to calculate the OR, made any difference to the pooled OR for HPV–OSCC association. We examined the effect of the geographical region (north, north-west, south and east) of China in a separate analysis.
The effects of study quality on effect estimates were investigated by conducting metaregression analysis to highlight potential associations between the OR and the total as well as four quality scoring domains. Cumulative meta-analysis was performed to demonstrate cumulative evidence at the time of publication of each study and to identify any trend of the results over the time. Influence analysis, where one study at a time was omitted in the calculation of the pooled OR, was used to determine the individual effect, if any, of each study on the summary outcome. Begg's and Egger's tests were used to assess for any existing publication bias. In addition, funnel plots constructed to demonstrate the relationship between individual log ORs and their SE were examined for the irregularities which could indicate publication bias.37 ,38
Results
Literature searches identified a total of 64 published studies evaluating a possible HPV–OSCC link in China. Of these, most were ineligible for inclusion—40 studies were case series, 1 was a case report, 3 did not specify the histological subtype of oesophageal cancer tested and 5 studies were not eligible for inclusion due to misclassification of the control specimens (ie, use of paraoesophageal tissue, oesophageal tissue from patients with oesophagitis and known head and neck malignancies as controls), 1 study did not specify or describe the participants from whom control tissue had been obtained (ie, cadavers, normal volunteers, paraoesophageal tissue from patients with cancer). Figure 1 illustrates the stages of selection of studies for inclusion in this meta-analysis. Fifteen case–control studies (6 from the English literature and 9 from the Chinese literature),31–35 39–48 testing a total of 1177 OSCC and 1648 oesophageal control specimens met our inclusion criteria and are described in table 1. From these studies, 55% (642/1177) of the cancer samples and 27% (445/1648) of the control samples were positive for HPV DNA.

Flow diagram of the selection in the meta-analysis.
Quality scoring
The average quality scores calculated for all 15 studies are recorded by category in table 2. The main section percentages and, where relevant, the subsection percentages referred to below represent the average percentage of the maximum possible score for that category of quality assessment. The overall quality of studies scored a total average percentage of 58% for quality assessment. Compared to all other sections, the measurement category scored the highest quality percentage of 79%. Investigation of outcome (92%) and exposure (71%) were both conducted well. While the subsection of the study base was relatively well described (77%), selection of cases (43%) and controls (43%) were poorly conducted, lowering the overall quality score of the selection category (54%). Adjustment for confounding factors (23%) and analysis of data (24%) both scored comparatively poorly. Nearly 40% of studies35 ,40 ,44–47 did not adjust for any confounding factors and only four case–control studies reported an OR,31–34 contributing to the low scores in quality assessment for these two categories.
Average quality scores and interobserver agreement on scoring for all studies included in the meta-analysis
The total ICC of 0.69 (95% CI 0.09 to 0.90) indicates good interobserver agreement and suggests that the scoring instrument utilised in quality assessment of the studies is reliable (table 2). The ICCs for the four quality assessment sections ranged from 0.61 to 0.83. The relatively low ICC score (0.61, 95% CI −0.15 to 0.87) allocated to the measurement section was attributed to misinterpretation of the assessment of control specimen validity and equivocal reporting of specimen storage and retrieval methodology in several studies. Similarly, a misconception of methodology relating to adjustment for confounding factors by one assessor resulted in a lower than expected ICC score of 0.66 (95% CI 0.00 to 0.89) for this section.
Pooled ORs and meta-analysis
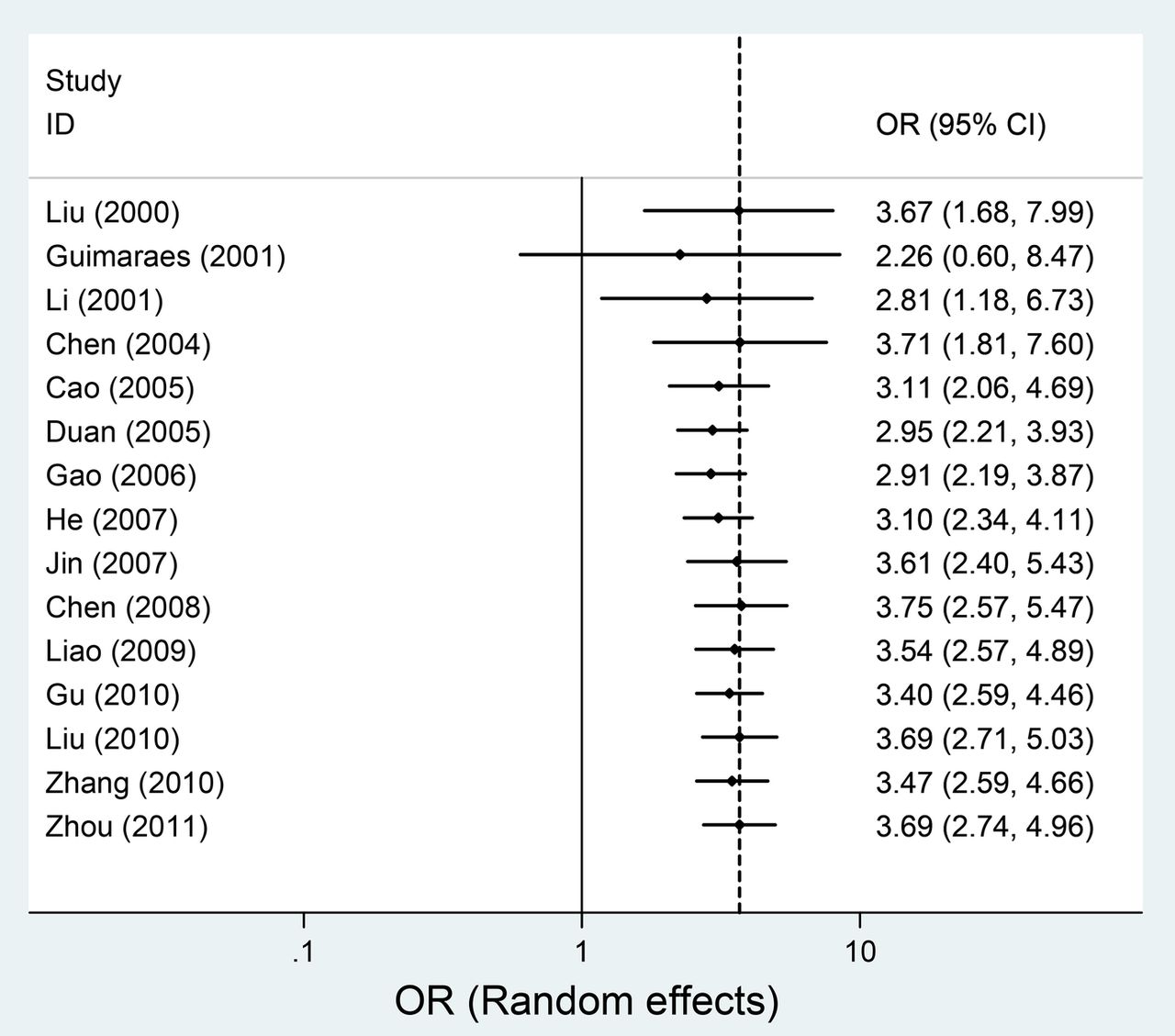
Individual and pooled OR estimates derived from a random effect model analysis have been illustrated in a forest plot (figure 2). The ORs for the case–control studies analysed ranged from 0.75 to 17.13. The pooled estimate was 3.69 (95% CI 2.74 to 4.96), indicating a significant association between HPV and OSCC. Cochrane's Q test for heterogeneity was not significant across all studies (Q=21.82, p value 0.082) and the I2 value was 35.83%. This can be interpreted as 35.83% of the variation across the studies being attributed to heterogeneity rather than chance. An I2 value of 25–50% is generally considered to be low to moderate, suggesting that there is a low to moderate probability that any variability in this meta-analysis is due to chance.49 Geographical region did not predict an association of HPV and OSCC (data not shown).

Forest plot for meta-analysis of the association of human papillomavirus with oesophageal squamous cell carcinoma in 15 case–control studies.
Meta-analysis of studies based on calculable and incalculable OR
There were 14 studies31–34 39–48 for which ORs could be calculated using data provided in the papers. A meta-analysis of these studies alone (figure 2) produced a pooled OR of 3.69 (95% CI 2.72 to 5.00) and an I2 value of 40. The remaining study35, which required manipulation of data using standardised techniques, in order to calculate individual ORs, was also analysed separately (figure 2), resulting in an OR of 6.19 (95% CI 0.29 to 131.84). When we combined all the studies, the pooled estimate was 3.69 (95% CI 2.74 to 4.96). Therefore, an independent analysis of both sets of studies showed a significant HPV–OSCC association, independent of the presence of the other subset, adding further weight to the evidence of an HPV–OSCC association.
Meta-regression
The meta-regression analysis investigated the association between study-specific ORs and the quality scoring domains that is, selection, measurement, confounding, analysis and overall study quality, to test whether any of the quality assessment sections were associated with the ORs from the individual studies (table 3). The regression coefficient for none of the quality domains is statistically significant. Therefore, we can conclude that ORs were not affected by the quality of the studies.
Results of meta-regression analysis of OR for HPV–OSCC association on scores from quality domains of all studies included in the meta-analysis
Cumulative meta-analysis
A cumulative random-effects meta-analysis of the 15 studies revealed the trend of the results over time. At the time of publication of all the studies, the cumulative evidence demonstrated a positive HPV–OSCC association and over the last decade, the Chinese population has demonstrated a relatively steady HPV–OSCC association with the earliest study in 200045 showing a cumulative estimate of 3.67 (95% CI 1.68 to 7.99) and the most recent study in 201148 also generating a cumulative estimate of 3.67 (95% CI 2.74 to 4.96). However, in general, earlier studies showed a slightly weaker trend of HPV–OSCC linkage than more recent investigations. From 2005 onwards, cumulative studies have resulted in a tighter CI for the summary estimate (figure 3).

Cumulative meta-analysis of case–control studies for the evidence of human papillomavirus involvement in oesophageal squamous cell carcinoma.
Influence analysis of individual studies
The meta-analysis result of the pooled OR was not significantly affected by omission of any of the 15 individual studies analysed (figure 4).

Influence analyses for individual studies on the summary effect.
Publication bias
There was no evidence of publication bias as demonstrated by the non-significant p values for Begg's (1.29) and Egger's tests (0.159) and the near-symmetric funnel plot (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plot for analysis results of publication bias.
Discussion
China has the highest burden of OSCC globally, which was the rationale for studying HPV in China as a potentially preventable risk factor for this highly lethal cancer. The unique contribution of this study is in combining all published case–control studies in the Chinese and English language literature. Our previous global meta-analysis was restricted to studies published in the English language and identified only six eligible studies from China.24 We identified an additional 9 eligible studies in the Chinese language literature, thereby increasing the number of studies to 15. We found an almost fourfold increase in the risk of OSCC in China when it was associated with the presence of HPV DNA within the oesophageal tissue. A significant pooled ORs of 3.69 (95% CI 2.74 to 4.96) with random effects model and I2 value of 40 in the meta-analysis, are highly suggestive of a positive link between OSCC and HPV in the Chinese population. Furthermore, this finding is supported by the analyses of all subcategories in the study. The influence analysis also showed that no single study, on its own, affected the summary effect significantly. In addition, the generation of an almost symmetric funnel plot for analysis of publication bias suggests that this was not a significant factor among the included studies. It was also determined that no single domain of quality assessed in each study influenced the estimated ORs by meta-regression analysis. Geographical region within China did not predict an association with HPV, but this may be because the published studies were mostly conducted in high-incidence regions. The separate analysis of both studies with calculable and incalculable ORs yielded independently significant pooled ORs suggestive of an association between HPV and OSCC. Further, our previous global meta-analysis confirms the association of HPV and OSCC in all countries, with an OR of a similar magnitude.24 The result of this meta-analysis provides the strongest evidence until now of an HPV–OSCC association in China. One of the high-risk oncogenic HPV types (HPV 16) was the most commonly detected HPV genotype among the Chinese studies.39–48 In view of the high incidence of OSCC in China and the availability of HPV prophylactic vaccines, this finding has important implications for potential prevention of OSCC in China.
Of the 130 publications worldwide, China has contributed the largest number of studies until now to the investigation of the role of HPV in OSCC.19 Although the literature offers 64 studies from China on this topic, any potential association of HPV and OSCC has been inadequately studied due to the inappropriate study design, high variability in laboratory techniques and methodology used to detect HPV, interlaboratory differences when using the same detection methods, variation in the specimen type tested, tissue storage, histological classification of malignant tissue and inaccurate definition of normal oesophageal tissues in case–control studies.21 The important contribution of our study is in identifying the few published studies with appropriate design (case–control methodology), and in identifying all studies on the subject published in the English and Chinese literature, thereby increasing the pool of available studies performed in China for analysis. Our previous global meta-analysis was limited to studies published in the English language, and contained only 6 studies from China, whereas this analysis includes 15 studies.
The limitations of this study include the use of observational epidemiological studies in the meta-analysis. However, case–control methodology is the most suitable method to investigate an HPV–OSCC association as it allows investigation of multiple cofactors in diseases with a multifactorial aetiology, such as OSCC.50 Also, a case–control study design offers a practical, time-efficient and cost-effective method of assessment of diseases with long latency periods, such as in OSCC, as the diagnosis has already been established at the start of the study.25 Most of the case–control studies identified for this meta-analysis were small-scale and heterogeneous with the largest comprising only 357 controls and 265 cases.34 Another limitation of this meta-analysis is the inability to adjust for confounders in the included studies. Approximately 40% of the studies in our meta-analysis did not adjust for known confounders such as gender, age, alcohol drinking, smoking, socioeconomic status and lifestyles of the studied population. Consequently, without controlling for the potential confounders, these factors may impact on the measurement of association between HPV and OSCC. In addition, other limitations include suboptimal study design, heterogeneous and small-scale studies, inconsistent laboratory methods for HPV detection, variations in specimen retrieval and storage and variable histological classification of tumour tissue. A final limitation is that since this study was conducted, further case–control studies have been published.51–54 However, we included 15 studies, with no single study having influence over the meta-analysis.
The results of our meta-analysis demonstrated that there is an almost fourfold association of HPV with OSCC in China. The public health implications of our findings are the potential for prevention of OSCC with prophylactic HPV vaccines in a high-incidence country such as China. The use of HPV vaccination is unlikely to be cost-effective in a country with low OSCC incidence, but may well be in the range of cost-effective interventions in China if clinical efficacy against OSCC can be determined, given that OSCC is one of the country's leading causes of cancer-related mortality. The lessons learnt with the world's first vaccine against an infectious cause of cancer, hepatitis B vaccine, where dramatic reductions have been observed in the reduction of hepatocellular carcinoma after decades of vaccination in high-risk countries like Taiwan,55 may well be applicable to HPV vaccine in China.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors CRM, BR, ATN and SSL conceived and designed the experiments. BR, SSL, IR, YZ and ZG performed the experiments. BR and SSL analyzed the data. SSL, BR, IR, ATN and QL contributed the reagents/materials and/or analysis tools. SSL, AM, CRM and BR wrote the manuscript. BR, IR, ATN, ZG, YZ, QL, J-FL, HS, AM and CRM were involved in the critical review and comments. AM was involved in the design of the consort diagram. AM, SSL and CRM were involved in the editing of this manuscript.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests CRM has been on advisory boards for Merck, GlaxoSmithKline (GSK) and Pfizer for vaccines other than human papillomavirus (HPV). She has received funding for investigator-driven research on HPV vaccine from Merck. She has received funding for investigator driven research for other vaccines from GSK, CSL Biotherapies and Pfizer. IR holds a National Health and Medical Research Council (NHMRC) Early career (630 739) and has received funding for investigator-initiated research from GSK and for consultation from Merck. ATN holds a NHMRC Training Fellowship (630 724—Australian Based Public Health Fellowship). HS currently holds a NHMRC Training Fellowship (1 012 631)—Australian Based Public Health Fellowship.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.