Article Text

Abstract
Objectives To evaluate whether four types of low-cost interventions in the working environment can promote the small everyday lifestyle adaptations that can halt the epidemics of obesity and hypertension when maintained long term.
Design A single-blind uninterrupted time-series intervention study consisting of four study periods: run-in (2 weeks), baseline (2 weeks), intervention (2 weeks), and after intervention 2 weeks).
Setting University Medical Centre with over 11 000 employees, over 1000 hospital beds and over 2000 customers visiting the hospital restaurant each day.
Participants Hospital staff and visitors.
Interventions (1) Point-of-decision prompts on hospital elevator doors promoting stair use. (2) Point-of-purchase prompts in the hospital restaurant promoting reduced-salt soup. (3) Point-of-purchase prompts in the hospital restaurant promoting lean croissants. (4) Reversal of the accessibility and availability of diet margarine and butter in the hospital restaurant.
Main outcome measures (1) Number of passages through 15 different parts of the hospital staircases. (2) Number and ratio of normal-salt and reduced-salt soup purchased. (3) Number and ratio of butter croissants and lean croissants purchased. (4) Number and ratio of diet margarine and butter purchased.
Results Elevator signs increased the mean 24-h number of stair passages per measurement site (baseline: 992 ± 479 on week days and 208 ± 116 on weekend days) by 11.2% (95% CI 8.7% to 13.7%). This effect was maintained at least 2 weeks after the point-of-decision prompts were removed. Point-of-purchase prompts promoting low-salt soup and lean croissants did not result in altered purchase behaviour. The ratio between the purchase of margarine and butter was changed sevenfold (p<0.01) by reversing the positions of these products in the hospital restaurant.
Conclusions Healthy lifestyle adaptations in the working environment can be effectively promoted by making healthy choices easier than unhealthy ones. Educational prompts at points-of-decision moderately increase stair climbing, but do not affect healthy food choices.
Protocol registration Clinicaltrials.gov identifier number: NCT01574040.
- Health Promotion
- Occupational & Industrial Medicine
- Physical Activity And Exercise Methodology
- Preventive Medicine
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
- Health Promotion
- Occupational & Industrial Medicine
- Physical Activity And Exercise Methodology
- Preventive Medicine
Article summary
Article focus
-
To evaluate whether four types of low-cost interventions in the working environment can promote the small everyday lifestyle adaptations that can halt the epidemics of obesity and hypertension when maintained long term.
Key messages
-
Because adults spend much of the day working, small lifestyle adaptations in the work environment can potentially halt the epidemics of obesity and hypertension on the long term.
-
Educational prompts at points-of-decision moderately increase use of the stairs instead of the elevator, but do not affect choices between healthy and unhealthy food alternatives in the worksite restaurant.
-
Accessibility of healthy food items in the worksite restaurant has a major impact on purchase behaviour.
Strengths and limitations of this study
-
Four different types of interventions were evaluated simultaneously using a single study design.
-
The study was performed in a large University Medical Centre with over 11 000 employees who were unaware of the study taking place and, thus, completely blinded to the study hypotheses.
-
Although randomisation of the interventions was not feasible, extraneous factors were kept constant and adjusted for.
Introduction
In modern sedentary society, middle-aged men and women on average gain approximately one pound weight each year.1 ,2 Resultantly, up to 28% of European men and up to 37% of European women are classified as obese (body mass index >30 kg/m2).3 The cumulative gap between energy intake and expenditure causing this yearly 1 pound weight gain, however, is approximately 3500 kcal or less depending on a person's initial body weight.4 This means that the obesity epidemic on average is caused by a daily energy imbalance between intake and expenditure of about 10 kcal.5 This amount of energy expenditure can be achieved by as little as 1 min stair walking.6 Moreover, the reduction of energy intake that can be achieved by choosing a lean food product alternative often exceeds 10 kcal by far. Prospective studies support that small changes in dietary pattern or physical activity are indeed associated with concomitant weight change.7 Yet, the increasing prevalence of obesity demonstrates that adopting such seemingly easy lifestyle changes in every day life is in fact tremendously challenging.
Another thread to public health that has arisen in recent years is excess salt consumption, causing hypertension and cardiovascular disease.8 ,9 Because salt is frequently used for preservation and seasoning of processed food products, excess sodium intake often goes unnoticed and is difficult to avoid. Although health-policy makers are well aware of the dangers of consuming too much salt, they too consume more than 6 g salt per day themselves. This follows from a recent study in The Netherlands, showing that the mean salt content of a single hot meal in staff canteens of health policy makers is 7.1 g.10 Excess salt consumption, in part, explains the current increase of the worldwide prevalence of hypertension.11
To ‘eat less and exercise more’ means changing individual lifestyle behaviours that have gradually been adopted over decades. This is often found difficult and rarely maintained long term. Because adults spend approximately half their waking hours working, we aimed to evaluate whether several types of low-cost interventions in the working environment can stimulate the healthy lifestyle adaptations in everyday life that may contribute to halting the epidemics of obesity and hypertension.
Methods
We performed a single-blind time-series intervention study in the University Medical Centre in Utrecht, The Netherlands, with over 11 000 employees and over 1000 hospital beds. Participants were a dynamic study population of staff and visitors of this hospital who were not informed about the study taking place. The study started 13 February 2012 and lasted 8 weeks, not including public holidays. During this 8 weeks period, the effect of four types of interventions was studied simultaneously. The study period was subdivided in four phases of 2 weeks each: a run-in period, a baseline period, an intervention period and an after-intervention period (figure 1). Outcome measurements were performed on a daily basis before (baseline period), during (intervention period) and after the interventions (after-intervention period).
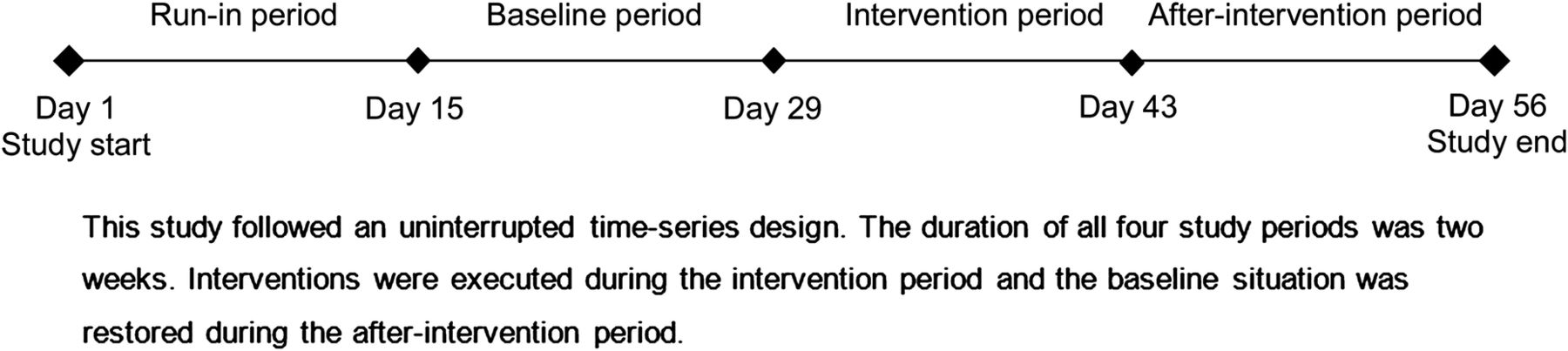
Flow cart of the study design.
The first intervention was aimed at promoting stair climbing. The energy expenditure during 1 min stair climbing is approximately 10 kcal.12 Thus, the problem of weight gain during adult life could on average be prevented by one additional minute stair climbing each day. Each of the three wings of the hospital where the study took place is equipped with three fast, parallel-operating and spacious elevators. Opposite all elevator doors is a broad, well-lit staircase, decorated with photographs on the walls and not portioned off by a door. Stair use between each of the six floor levels of the three main hospital wings (ie, 15 measurement spots) was defined by the number of passages (both up or down), measured by Fastcount SP RS wireless infrared interruption counters (Solvatronics B.V., Amsterdam, The Netherlands). The cumulative value of each interruption counter was recorded each day of the study period at 17:30. During the intervention period, signs were placed right above the elevator buttons stating ‘Stair climbing increases energy expenditure 11-fold’ (see online supplementary appendix figure 1). These signs were removed during the after-intervention period.
The second intervention was aimed at reducing salt intake. A previous study showed that the average salt content of a hot lunch (soup and non-vegetarian hot dish) in our hospital restaurant is as much as 8.5 g.10 Pilot sampling for the present study revealed that this constitutes of an average 2.4 (SD 0.3) grams salt in an average 200 ml soup cup. The restaurant in the hospital where this study took place welcomes over 2000 staff members and visitors each week day. Every day, two types of soup are offered side by side, a clear soup (eg, chicken, vegetables, noodle,, etc) and a cream soup (eg, mushroom, asparagus, tomato,, etc). During the entire study period, the salt content of the cream soup (but not the clear soup) was reduced by approximately 30% to 1.7 (SD 0.1) g on average. During the 2 weeks of the intervention period, signs were placed at the soup counter stating ‘The cream soup contains 30% less salt and contributes to a healthy blood pressure’ (see online supplementary appendix figure 2). Both types of soup were priced equally and available in excess until closure time of the restaurant. The number of normal salt (clear) soup cups and reduced salt (cream) soup cups purchased on each week day was recorded from the pay-desk computer system.
The third intervention was aimed at reducing calorie intake and consumption of saturated fatty acids. Butter croissants are a popular lunch item in The Netherlands. Yet a 40 g butter croissant contains 8 g fat.13 Half of the 157 kcal in one butter croissant are, thus, derived from its fat content.13 Therefore, a lean croissant, containing 30% less fat (approximately 20 fewer kilocalories), was introduced in the hospital restaurant prior to this study. The lean and the butter croissants were similar in price, appearance and taste. Each week day, a standard amount of 45 butter croissants and 45 lean croissants were placed in separate baskets next to each other without signs pointing out the difference between the two. Each type had its own baskets and the positions of these baskets remained unchanged during the study period. During the intervention period, promotional signs were placed on the baskets of the lean croissants, stating ‘The saturated (unhealthy) fat content of this croissant is 30% lower’ (see online supplementary appendix figure 3). Once the first type of croissants was sold out (ie, once the choice option disappeared), the remaining croissants of the other type were counted by the investigator and considered unsold.
Finally, the fourth intervention was also aimed at reducing calorie intake and consumption of saturated fatty acids. Sandwiches are a major constituent of a typical Dutch lunch and consumption of at least 10 g margarine or butter each day (sufficient for one sandwich) is not unusual.14 One serving of 10 g butter, however, contains 8 g (mostly saturated) fat (74 kcal).13 Alternatively, the hospital restaurant where this study took place offers diet margarine containing 6 or even 4 g (mostly unsaturated) fat per 10 g serving (54 or 34 kcal, respectively).15 Because margarine compared to butter has a longer shelf life outside the refrigerator, margarine cups are normally presented at four centrally located and easy-to-reach positions in the hospital restaurant, while butter cups are placed in one of the fridges and are, thus, harder to reach. During the 2 weeks intervention period, we observed how changing the positions of these products (ie, the accessibility) affected the purchase of butter and margarine as recorded from the pay desk computer system. Both margarine and butter cups were available in abundance during the entire course of the study. Thus, customers who preferred one or the other product for its taste were able to purchase it at any time during the course of the study.
As a measure of the number of staff and visitors in the hospital on each day, the number of restaurant customers was recorded from the pay desk computer system. The institutional review board of the University Medical Centre Utrecht approved the study. The study was registered on http://www.clinicaltrials.gov; unique identifier NCT01574040.
Data analyses
The number of persons passing through the staircases was expressed per 24 h. Because the absolute number of passages differed substantially between the 15 different measurement sites, counts were expressed as percentage of baseline average. Baseline average was defined as the mean number of passages per 24 h over all days of the baseline period at each measurement site. After rescaling, all separate observations were included in linear regression models that were used to calculate the average percentage change in stair use over all measurement sites during the intervention period and during the 2 weeks thereafter. To increase model precision, a variable ‘weekend day (yes/no)’ was included to account for the reduced number of staff during the weekends. Similar to one previous study,16 results are presented with and without additional adjustment for the number of hospital restaurant customers on each day, reflecting variations in building occupancy. Results were stratified by hospital wing and floor level to assess the consistency of our findings. Recordings of the number of passages through the staircases from one measurement site were missing on three separate days (0.4% of all measurements) owing to technical failure of the person counter. These were excluded from the analyses.
The average numbers of clear soup cups and cream soup cups purchased on weekdays during each study period were expressed per 1000 restaurant visitors and as the ratio between the two. Similarly, the average numbers of butter and margarine servings purchased on weekdays during each study period were also expressed per 1000 restaurant visitors and as the ratio between the two. The average numbers of butter croissants and lean croissants, however, were expressed as the average number purchased until the first type was sold out and the ratio between those two. p Values for difference between the intervention period and the baseline period and between the after-intervention period and the baseline period were based on unpaired t tests. Few missing data on consumption of croissants (n=2; 7%), soup cups (n=1; 3%) and margarine or butter (n=1; 3%) that occurred due to study personnel's incidental incompliance with the study protocol were excluded from the analyses.
Analyses were conducted with R statistical software V.2.11.1 (http://www.R-project.org).
Results
The main characteristics of the three study periods are demonstrated in table 1. The number of week days and weekend days in each study period was exactly equal and no difference was observed in the average number of hospital restaurant customers. Yet, more sunny days occurred during the intervention period and maximum temperature was a few degrees higher during the intervention and after-intervention period compared to baseline.
Characteristics of the study periods
During the baseline period, the mean 24 hr number of stair passages per measurement site was 992 (± an SD of 479) on week days and 208 (± 116) on weekend days. Table 2 shows that stair use increased during the intervention period by 8.5% (95% CI 5.8% to 11.1%) on average or 11.2% (95% CI 8.7% to 13.7%) when adjusted for the number of restaurant customers, reflecting the number of staff and visitors inside the hospital building on each day. The largest increase in stair use was observed in the second hospital wing, whereas no change was observed in the first hospital wing (p value for overall difference between the hospital wings <0.01). Similarly, an increase was observed at all floor levels except between levels 0 and 1, although the difference between the floor levels was not significant (p value 0.26). Floor level 0 is the basement level of the hospital building that is mainly used for transportation of goods. After the elevator signs were removed, increased stair use was maintained during the after-intervention period.
Effect of the intervention on stair use
Figure 2 demonstrates that promotion of the reduced-salt cream soup did not affect the number of normal salt clear soup cups or reduced-salt cream soup cups sold or the ratio between them. Observed differences were in the hypothesised direction, but not statistically significant. This is also true for the number of butter croissants and lean croissants that were purchased. Compared to baseline, the ratio between lean and butter croissants was unchanged during the intervention period, but increased during the after-intervention period from 0.67 ± 0.18 to 0.90 ± 0.18 (p=0.02). Reversing the positions of margarine and butter, making the unhealthy food option (ie, butter) temporarily better accessible, decreased the ratio of margarine and butter servings that were sold from 7.3 ± 1.9 to 1.1 ± 0.2 (p<0.01), thus leading to unhealthy behaviour. This effect completely disappeared after the baseline situation was restored during the after-intervention period.

{kind=link}
{kind=link}
Effect of the interventions on reducing salt, calorie and (saturated) fat intake in the hospital restaurant.
Discussion
Although the actual energy expenditure deficit may differ between individuals and from day to day, gradual weight gain of one pound per year during adult life could on average be prevented by consumption of 10 fewer kilocalories or expenditure of 10 additional kilocalories on a daily basis. In this time-series study, that was performed in a large University Medical Centre, we have evaluated the effects of four low-cost interventions in the work environment aimed at promoting healthy lifestyle modifications that could make this 10 kcal difference. Point-of-decision prompts on elevator doors were shown to increase the number of hospital staff and visitors taking the stairs by 11.2% and the behavioural change was maintained at least until 2 weeks after the intervention. Signs promoting healthy food alternatives in the hospital restaurant, on the other hand, did not have a major effect on food choices. Indeed, a somewhat increased consumption of lean compared to butter croissants was observed in this study. Yet, although a delayed effect of the intervention cannot be excluded, the relation between this increase and the promotional intervention is uncertain because it was observed only after the promotional signs were already removed. Strikingly, however, the largest effect on health behaviour was achieved by modification of the accessibility of a healthy food product and its unhealthy alternative. Diet margarine compared to butter was consumed seven times less often when it was presented at a single, somewhat distant position in the hospital restaurant instead of multiple, centrally located and easy-to-reach positions.
The present study was performed in a single centre and the intervention was non-randomised. Yet, this single study centre was a large University Medical Centre with over 11 000 employees, over 1000 hospital beds and over 2000 customers visiting the hospital restaurant each day, thus contributing to a large number of study observations. Randomisation was not feasible owing to the nature of the intervention. Instead, extraneous factors were kept as stable as possible. For example, the study period was scheduled in such a way that public holidays were not included. Also, results were adjusted for the number of customers of the hospital restaurant as a measure of building occupancy, like was done in one previous study also.16 Thus, although no data about elevator use were obtained during the study, we were able to ascertain that changes in the number of passages through the staircases were not just due to changes in building occupancy. A factor that could not be stabilised, however, was the weather type. Warmer weather during the intervention period may have influenced food choices. Especially, hot soup may be more popular on colder days. Although this may explain why promotional signs did not increase the consumption of low-salt cream soup, a concomitant (stronger) reduction of the consumption of normal-salt was not observed. Still, the ratio between normal-salt and low-salt soup moved in the hypothesised direction during the intervention period and it is not inconceivable that a significant difference would have been observed if more observations were made. The interventions in this study lasted 2 weeks and it could not be inferred from this study whether any effects last if the interventions are continued long term. Similarly, measurements went on until 2 weeks after the interventions. Whereas promotion of stair climbing still exerted positive effects during those 2 weeks while the elevator signs were already removed, it remains uncertain whether those effects are maintained after a longer period. Unfortunately, we were unable to discriminate whether the effect of the elevator signs was due to increased stair use by hospital employees or by visitors or both. The largest increase was observed in the hospital wing that is closest to the main entrance and attracts the largest number of visitors. Yet, the fact that stair use remained increased after removal of the point-of-decision prompts suggests a behavioural change of hospital staff. Also, we were unable to assess whether changes in stair use were caused by increased stair climbing, stair descent or a combination of both. Notably, stair climbing requires at least twice the energy expenditure of stair-descent making climbing the preferred public health target.17 A final limitation of this study is that we were unable to assess whether the interventions affected weight or blood pressure. This is because the follow-up period was too short and because we did measure these outcomes. A notable strength of this study is that the participants (ie, employees and visitors of the hospital) were unaware of the study taking place and, thus, completely blinded to the study hypotheses. This is important, because such awareness during the before-intervention and the after-intervention periods could potentially result in underestimation of the effect of the interventions. Moreover, a unique feature of this study is that four types of interventions are evaluated simultaneously so that a comparison can be made as to which type of intervention is most effective.
Promoting stair climbing in public buildings or at the work site has since long been a well-recognised opportunity for increasing engagement in physical activity by adults.18 The effect of point-of-decision prompts, like the elevator signs in the present study, have been evaluated by previous studies.18 ,19 Like the present study, most of these studies follow a time-series design, but study settings vary substantially. Studies in settings where elevator use is the alternative to stair use, like in the present study, show that point-of-decision prompts increase stair use by a median of 5%, which is lower than the 11.2% that was observed in the present study.18–20 Much larger effects are typically observed in settings where escalators are the alternative to stair use (median increase of 77%), but escalators are uncommon in work environments.18–20 Enhancements to stairs or stairwells (eg, foot steps, adding artwork, painting walls, etc) have been proposed to reinforce the effect of point-of-decision prompts, but there is insufficient evidence to support their effectiveness.18 Studies, evaluating point-of-purchase educational interventions aimed at promoting healthy food items, suggests that product health information does not have significant effects on actual purchase behaviour in supermarkets or restaurants.21 ,22 This is in accordance with our observations that consumption of reduced-salt soup and lean croissants was unaffected by the promotional signs. The effect of increasing the availability of and access to healthy food items on purchase behaviour is less well studied, but available evidence supports our observation that increased ease of access to an unhealthy option results in less healthy choices.23 ,24 One type of point-of-purchase intervention that was not evaluated in the present study is the effect of financial reward by discounting healthy compared to unhealthy food, which may also be effective.24–26 In addition, decreasing portion sizes has been proposed as a method to reduce caloric intake, but the effect of such intervention is compromised because smaller meals are often compensated by purchasing additional food items.27 Finally, it may well be that the effects of isolated interventions can be enhanced by combining them with a promotional campaign.
In conclusion, the present study shows that educational prompts at points of decision are moderately effective or ineffective for promoting a more healthy lifestyle. The accessibility of healthy food items in the worksite restaurant, however, had a major impact on purchase behaviour. Small changes in everyday behaviour may on the long term have important impact on body weight and blood pressure.
Acknowledgments
We gratefully acknowledge the contribution of Tim Leegwater (restaurant floor manager), Stef Baan (chef cook of the restaurant kitchen), Jan de Bruin (cluster manager nutrition), Leonie J Braskamp (restaurant department manager) and other employees of the hospital restaurant for their enthusiasm and collaboration. Furthermore, we express our gratitude to Corrie AMP Scholman and Frans R Urban (Department of Human Resources) for their involvement in organising and funding this study. This study provided the two outcome assessors of this study with the opportunity to burn an estimated 30 000 kcal during data collection over an 8 weeks period, thereby achieving a higher level of physical fitness.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix 1
- Data supplement 2 - Online appendix 2
- Data supplement 3 - Online appendix 3
Footnotes
-
Contributors JANDwas involved in conception of the research question, data collection and data handling, design and execution of data analyses, interpretation of the results, drafting of the manuscript. YvdG and WS were involved in conception of the research question, interpretation of the results, revision of the manuscript for important intellectual content. KLZ carried out data collection and data handling, design and execution of data analyses, revision of the manuscript for important intellectual content. FLJV was involved in conception of the research question, design of data analyses, interpretation of the results, revision of the manuscript for important intellectual content.
-
Funding This study was supported by a grant from the Human Resource Department of the University Medical Centre Utrecht, who had no role in the conduct of the analyses or drafting of the report. All statistical analyses were carried out by the investigators.
-
Competing interests None.
-
Ethics approval The Ethics Committee of the UMCU approved the study.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement There are no additional data available.