Article Text

Abstract
Objectives To describe the demographic characteristics and incidence of unintentional fall-related fractures among older adults treated in the US hospital emergency departments (EDs).
Design Retrospective observational study.
Settings Hospitals’ ED participants in the National Electronic Injury Surveillance System All Injury Program (NEISS-AIP).
Participants The NEISS-AIP was used to generate national estimates of hospital ED visits for unintentional fall-related fracture among adults aged 65 years or older between 2001 and 2008. Census population estimates were used as the denominator to calculate age-specific and age-adjusted fracture rates per 100 000 persons.
Main outcome measures Fall-related fracture rates and ED disposition.
Results On the basis of 70 199 cases, an estimated 4.05 million older adults were treated in US hospital EDs for fall-related fracture during the 8-year period. Two-thirds of the injuries occurred at home and 69.5% (95% CI 59.7% to 77.8%) of the affected individuals were white. Fall-related fracture rates increased gradually with age and were on average twofold higher among women. Of those hospitalised, women and fractures of the lower trunk represented 75.2% and 65.1% of the admissions, respectively. The estimated number of fall-related fractures treated in EDs increased from 574 500 in 2001 to 714 800 in 2008, a 24.4% increase. By gender, a non-significant upward trend in age-adjusted fall-related fracture rates was predominantly seen among men at an annual rate of 1.9% (95% CI −0.1% to 4.0%), whereas fracture rates among women remained stable at 0.9% (95% CI −0.7% to 2.5%) per year.
Conclusions The oldest old, women and lower trunk fractures account for the majority of fall-related fractures among persons aged 65 years or older treated in US hospital EDs. Increasing ED visits and hospitalisations for fall-related fracture among older adults deserve further research.
- Geriatric Medicine
- Accident & Emergency Medicine
- Epidemiology
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Article summary
Article focus
-
The aim of this study was to describe the demographic characteristics and incidence of unintentional fall-related fracture among persons aged 65 years or older treated in the US hospital EDs.
Key messages
-
An estimated 4.05 million older adults were treated in hospital EDs for fall-related fracture between 2001 and 2008.
-
The oldest old, women and lower trunk fractures account for the majority of fall-related fractures among persons aged 65 years or older treated in EDs.
-
EDs visits and hospitalisations for fall-related fracture among older adults increased in the USA during the study period.
Strength and limitations of this study
-
The present study reports national estimates of fall-related fracture by gender and body part among older adults.
-
ICD-9-CM diagnosis codes were not available in the medical records at the time these data were collected; therefore, specific types of injuries (eg, hip fracture) could not be accurately identified.
Introduction
One-third of people over the age of 65 years who live in the community fall each year; this proportion increases to 50% by the age of 80 years.1 Although not all falls of older persons are injurious, about 5% of them result in a fracture, and other serious injuries occur in 5–10% of falls.2 In 2001, an estimated 1.64 million older adults were treated in hospital emergency departments (EDs) for unintentional fall-related injuries in the USA. Of these, fractures accounted for 37.8% of women's and 28.3% of men's injuries.3
Between 2001 and 2008, fractures were the most frequent primary diagnosis (63%) among older adults hospitalised after being treated in hospital EDs for fall-related injuries.4 Similarly, a prior study showed that fractures accounted for 84% of hospitalisations for fall-related injuries among older adults in the USA between 1988 and 2005. Moreover, hip fracture was the leading diagnosis in both genders, resulting in an estimated 1 581 600 (47.6%) hospitalisations during the 18-year study period.5
About 1–14% of falls in women result in hip fracture and over 90% of hip fractures are the result of a fall.6 Although hip fracture rates and subsequent mortality are declining in the USA, information is scarce about the epidemiology of other fall-related fractures nationwide among older adults.7 ,8 Thus, the aim of this study was to describe the demographic characteristics and incidence of unintentional fall-related fracture among persons aged 65 years or older treated in hospital EDs between 2001 and 2008.
Methods
The National Electronic Injury Surveillance System All Injury Program (NEISS-AIP) is designed to provide national incidence estimates of all types and external causes of non-fatal injuries and poisonings treated in US hospital EDs. Data on injury-related visits were obtained from a national sample of 66 of 100 NEISS hospitals, which were selected as a stratified probability sample of hospitals in the USA with a minimum of six beds and 24 h EDs. Data are weighted by the inverse of the probability of selection to produce national estimates. The sample includes separate strata for very large, large, medium and small hospitals, defined by the number of annual ED visits per hospital. Data obtained on each case include age, race/ethnicity, gender, principal diagnosis, primary body part affected, consumer products involved, disposition at ED discharge (ie, hospitalised, transferred, treated and released, observation and died), locale where the injury occurred, work-relatedness and a narrative description of the injury circumstances, also, major categories of external cause of injury (eg, motor vehicle, falls, cut/pierce, poisoning and fire/burn) and of intent of injury (eg, unintentional, assault, intentional self-harm and legal intervention). Trained, onsite hospital coders took data for injury-related cases from ED records at NEISS hospitals. The coders coded all data elements, except for cause of injury. These coded data and a narrative were electronically transmitted to Consumer Product Safety Commission (CPSC) headquarters. NEISS-AIP quality assurance coders at CPSC headquarters reviewed all of the data elements as well as a narrative (description) for each case from each of the 66 NEISS-AIP hospitals. Quality assurance coders then used the narrative and other data to assign codes for the precipitating and direct causes/mechanisms of injury for each case. The present study included persons 65 years or older treated in US hospital EDs for unintentional fall-related fractures between 2001 and 2008. National estimates are considered unstable and potentially unreliable if the number of records is based on fewer than 20 NEISS-AIP cases, national estimates fewer than 1200 (based on weighted data) or the coefficient of variation of the estimate is greater than 30%. The NEISS-AIP public use files were downloaded from the Inter-University Consortium for Political and Social Research.9
Statistical analysis
All statistical analyses were performed using SPSS Complex Sample software, V.17 (SPSS Inc, Chicago, Illinois, USA) and incorporated population-based sampling weights to obtain unbiased, nationally representative estimates from the NEISS-AIP sampling design. The sample weight has been adjusted for hospital non-response within each NEISS-AIP sample stratum and changes in the number of ED visits annually in the sampling frame of US hospital EDs. Means and proportions were used to describe demographic and clinical characteristics of the study sample. The US Census Bureau population estimates were used as the denominator to calculate fall-related fracture rates per 100 000 persons.10 Fracture rates were then standardised by the direct method to the US population for the year 2000 to account for changes in the age distribution of the population over time. Linear regression was used to examine the statistical significance of trends in fall-related fracture rates over the study period. The results are presented as the annual percentage change in rates and corresponding 95% CI. The annual percentage change is one way to characterise trends over time in which the rates are assumed to change at a constant percentage of the rate of the previous year. All analyses were performed by using Joinpoint software, V.3.5.0.11
Results
On the basis of 70 199 cases, an estimated 5.04 million adults with a mean age of 80.0 (SD 8.2) years were treated in US hospital EDs for unintentional fall-related fracture between 2001 and 2008. Women accounted for 75.2% (95% CI 74.2% to 76.2%) of these cases and 69.5% (95% CI 59.7% to 77.8%) of the affected individuals were white. Overall, 58.7% (95% CI 54.0% to 63.3%) of these injuries occurred at home. Moreover, after a fall-related fracture, 50.6% (95% CI 47.7% to 53.5%) of the patients were treated and released from the ED and 44.2% (95% CI 40.9% to 47.7%) required hospitalisation. Of those hospitalised, women and fractures of the lower trunk (lumbar spine, pelvis and hip) represented 75.2% (95% CI 73.9% to 76.5%) and 65.1% (95% CI 62.0% to 68.1%) of the admissions, respectively.
The number, national estimates and fall-related fracture rates according to gender and primary body part affected are shown in table 1. In general, lower trunk fractures were the most frequently reported injuries in both genders, representing 37.3% (95% CI 37.2% to 39.5%) of fall-related fracture visits to EDs in the US during the study period. Moreover, wrist and upper trunk fractures (thoracic spine, ribs and sternum) accounted for a considerable proportion of fall-related fractures among women, whereas among men, upper trunk fracture was the second most frequent reason for fall-related fractures ED visits, representing an estimated 197 000 fractures.
Emergency department fall-related fracture estimates and incidence rates according to gender and body part, NEISS-AIP 2001–2008
The incidence of fall-related fracture rates increased with advancing age and were on average twofold higher among women (figure 1). In fact, compared with those in the age group of 65–69 years, fracture rates in the age group of 85 years or older were fourfold higher among women and fivefold higher among men. After adjusting for age, fall-related fracture rate varies by race. The highest rates per 100 000 persons were 1268.9 among non-Hispanic whites, whereas the lowest rates of 876.6 were seen among Asians. Blacks and American Indians had rates that were similar but intermediate between those of whites and Asians.
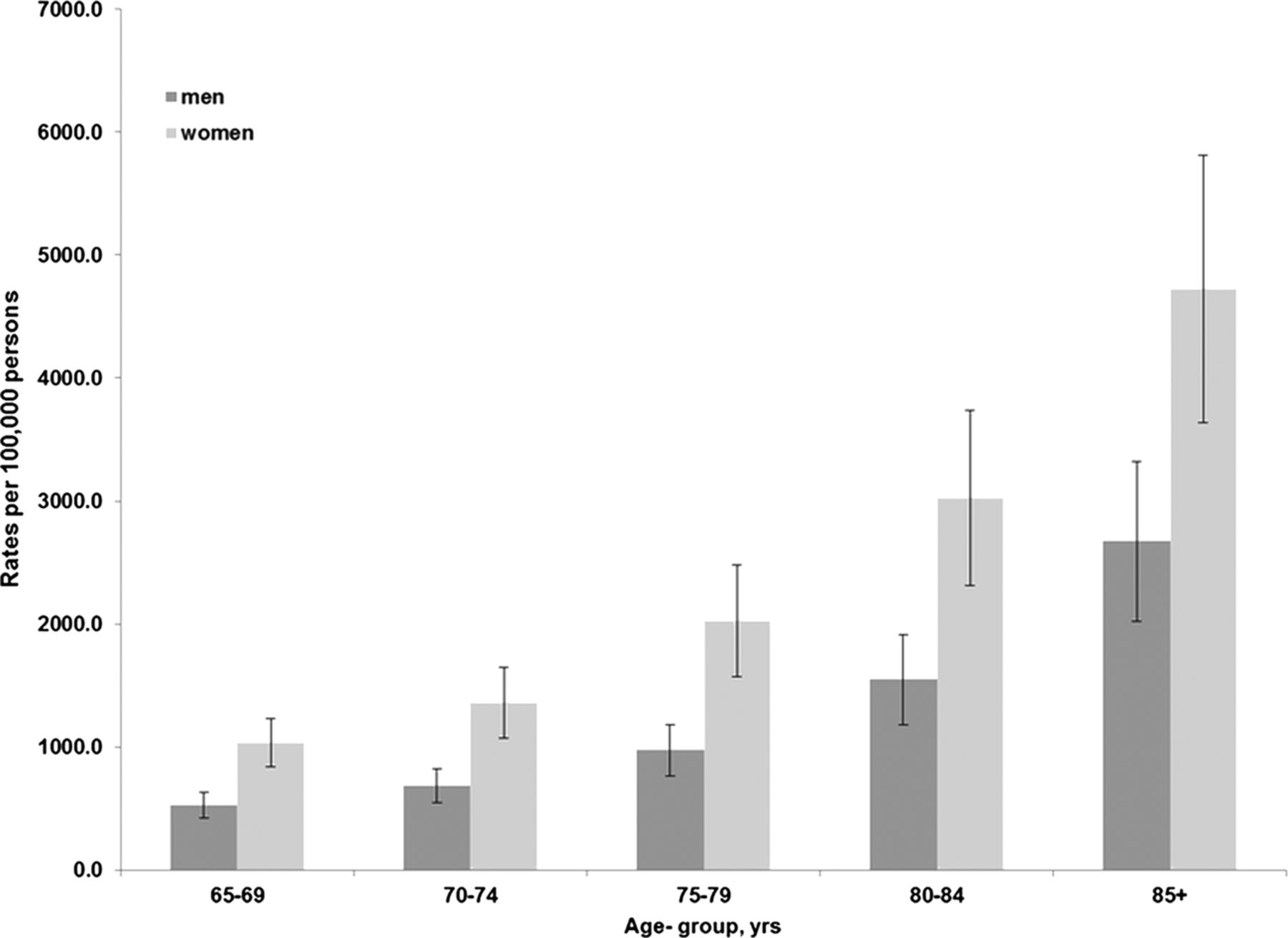
Fall-related fracture rates and 95% CI among older adults treated in US emergency departments.
The estimated number of fall-related fractures treated in EDs increased from 574 500 in 2001 to 715 000 in 2008, a 24.4% increase. However, the population of older adults also increased by 9.8% in the USA during the same period. After age adjustment, fall-related fracture rates increased from 1618.7 in 2001 to 1789.4/100 000 persons in 2008, a 10.5% increase. By gender, a non-significant upward trend in age-adjusted fall-related fracture rates was seen among men at an annual rate of 1.9% (95% CI −0.1% to 4.0%), whereas fracture rates among women remained stable at 0.9% (95% CI −0.7% to 2.5%) per year (figure 2).
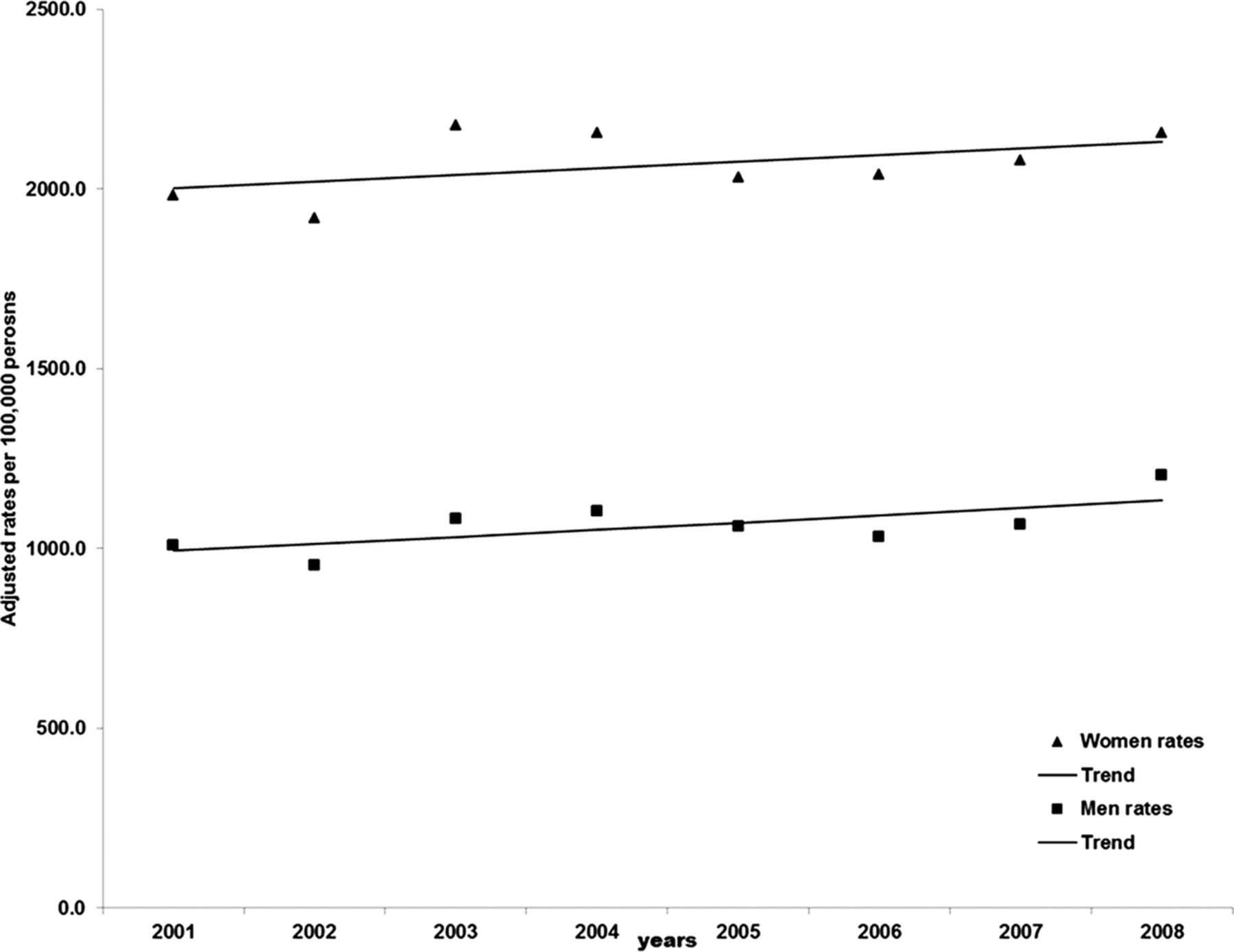
Trends in fall-related fracture rates treated in US emergency departments, 2001–2008.
As shown in figure 3, the proportion of patients hospitalised for fall-related fracture increased from 43.5% (95 CI 42.4% to 44.5%) in 2001 to 48.4% (95 CI 47.4% to 49.3%) in 2008, with a corresponding decrease in the proportion of patients released from EDs from 53.4% (95 CI 52.3% to 54.5%) to 48.7% (95 CI 47.7% to 49.7%) during the same period. The proportion of patients transferred to other facilities remained stable over time.

{kind=link}
{kind=link}
{kind=link}
Disposition of older adults treated in US hospital emergency departments for fall-related fracture.
Discussion
In this nationally representative sample, an estimated 5.04 million older adults were treated for fall-related fractures in the US hospital EDs between 2001 and 2008. Fall-related fracture rates increased gradually with advancing age and were on average twofold higher among women. The gender differences in fall-related fracture rates were mainly attributed to higher proportions of upper extremity and lower trunk fractures (lumbar spine, pelvis and hip) among women. In fact, lower trunk fractures in women accounted for 28% of all fall-related fractures among older adults treated in EDs during the 8-year period. The present findings are consistent with a report from the Healthcare Cost and Utilization Project Nationwide Emergency Department Sample on ED injury visits among older adults in which women were more likely to have ED visits for upper extremity and hip fractures than older men. In addition, women were two to three times more likely than men to have a fall-related ED visit for most types of fracture. Overall, hospitalisation occurred in 51.3% of older adults with a fall-related fracture ED visit.12 Similarly, a recent study using data from the NEISS-AIP showed that fall-related forearm and wrist fracture rates among persons 50 years or older treated in hospital EDs nationwide were on average 3.3 higher in women than those rates in men.13 Possible explanations for the marked gender differences in fractures are the higher prevalence of osteopenia and osteoporosis among women and the 40–60% higher fall-related injury rates reported among women.3 ,14
The racial differences in fall-related fracture rates found in this study are also consistent with results from previous investigations in which white women had the highest fracture rates, whereas black and Asian women had the lowest fracture rates.15 ,16 Although many risk factors for fracture have been identified in white women, less is known about risk factors for fracture in non-white women. In a prospective study of 159 579 women aged 50–79 years enrolled in the Women's Health Initiative study, three risk factors common to all racial groups were older age, positive history of prior fracture after the age of 55 years and a positive history of two or more falls.14 ,17 Among fallers, an increasing amount of leisure-time physical activity and wearing proper shoes with low, wide heels that cover and stay on the foot in the event of a fall have been associated with decreased risk of fractures at the foot, distal forearm, proximal humerus, pelvis and shaft of the tibia/fibula compared with fallers who do not fracture.18 Moreover, among older white women, walking for exercise, reducing caffeine intake, quitting smoking, avoiding long-acting sedatives agents, treating impaired vision and preserving bone mass were reported to reduce the risk of hip fractures.19
Several studies have reported that fractures of the hip, spine or wrist are predictors of subsequent fractures.20–23 Recently, investigators have demonstrated that besides typical osteoporotic fractures, prior non-hip and non-spine fractures in both genders are associated with the incidence of traditional fragility fractures, as well as with fractures of the humerus and tibia/fibula.20 Moreover, prior rib and upper leg fracture fractures are associated with increased risk of subsequent vertebral and hip fracture, respectively. Among women, a history of ankle fracture increased the risk of future fracture of a weight-bearing bone.21
Of interest, 44.2% of patients treated in EDs for fall-related fracture required hospitalisation and the proportion of older adults hospitalised for these injuries increased during the 8-year study period. Although the present analysis was limited to fall-related fractures, these findings are consistent with a recent study that reported an increase by 50% in the estimated number of fall-related hospitalisations among older adults in the USA between 2001 and 2008. Of these, hospitalisations for fractures accounted for 63% of the diagnoses.4 Similarly, fractures were the most common admitting diagnosis among persons aged 65 years or older hospitalised for fall-related injuries in the USA between 1988 and 2005, representing 84% of the admissions.5 Moreover, fall-related injury hospitalisation rates increased in both genders during the 18-year period.
Overall, the number of fall-related fractures among older adults treated in EDs increased between 2001 and 2008. After age adjustment, a non-significant upward trend in fall-related fracture rates was seen among men. The precise reason for this finding is unknown. However, differences in osteoporosis recommendations for screening and prevention between men and women may account for increasing fall-related fracture rates seen among men.24 These results contrast with a previous study among Medicare beneficiaries that reported a significant decrease in hip fracture rates among men and women between 1995 and 2005.7
The increased proportion of older Americans with physical limitations (stooping, lifting, reaching, grasping and walking) over time may also partly explain these findings. In fact, data from the Medicare Current Beneficiary Survey indicate that the age-adjusted proportion of non-institutionalised adults aged 65 years and older with physical limitations increased from 32.7% in 1992 to 38.4% in 2009.25 Similarly, a recent study using data from the National Health and Nutritional Examination Survey demonstrated an increased prevalence of self-reported disability over time among older Americans in basic activities of daily living, instrumental activities of daily living and mobility.26 Disability of the lower extremities has been associated with increased risk for falls among those aged 75 years or older living in the community and with fall-related hip fracture in women.6 ,27 Moreover, adequate physical activity has been associated with a reduced risk of fractures among fallers, possibly because physical activity can increase physical functioning, maintain mobility, increase muscle strength and balance, improve bone mineral density and improve reaction time.18
Several limitations of this study must be mentioned in interpreting the present findings. First, the number of fall-related fractures among older adults may be underestimated because it includes only those persons who were treated in hospital EDs; the NEISS-AIP does not include persons treated in a physician's office or other outpatient settings. Second, some fractures may have been missed because the NEISS-AIP includes the principal diagnosis and primary body part noted during the initial injury visit. In cases with multiple injuries, data for only the most severe injury are recorded. Third, the NEISS-AIP coding system has a fixed number of categories for the primary body part affected and for the principal diagnosis relevant to consumer–product-related injuries. ICD-9-CM diagnosis codes were not available in the medical records at the time these data were collected; therefore, specific types of injuries (eg, hip fracture) could not be accurately identified.3 Fourth, the present findings may be generalised to hospital ED visits for fall-related injuries among older adults in the USA. However, regional or fracture rates by state cannot be determined. Finally, the NEISS-AIP does not evaluate healthcare services and medical outcomes after this type of injury.
Despite these limitations, this study describes the demographic characteristics and incidence of fall-related fractures nationwide among older adults treated in hospital EDs. Since the population of 65 years and older in the US will increase more than double by 2050, rising from 39 million today to 89 million, these demographic changes alone will increase the number of fall-related fractures unless interventions to prevent falls among older adults are effectively implemented.28 Although specific interventions on modifiable risk factors among older adults have shown to markedly decrease the prevalence of falls, healthcare providers should recommend exercise or physical therapy and vitamin D supplementation to prevent falls in community-dwelling older adults who are at increased risk of falling.27 ,29
In conclusion, the oldest old, women and lower trunk fractures account for the majority of fall-related fractures hospital ED visits among persons aged 65 years or older in the USA. Increasing ED visits and hospitalisations for fall-related fracture among older adults deserve further research.
Acknowledgments
The author would like to thank Mrs Patricia Gutierrez from UTHSC Laredo campus for librarian assistance.
References
Footnotes
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The NEISS-AIP files are publicly available for analysis at http://www.icpsr.umich.edu/icpsrweb/ICPSR/series/198/studies/30544?q=neiss&permit%5B0%5D=AVAILABLE&paging.startRow=1.