Article Text

Abstract
Objectives The aim of this study was to evaluate if the use of antitransglutaminase (tTG) and antiendomysium (EM) antibodies has modified the profile of coeliac disease (CD) in children.
Design Retrospective cohort study.
Setting Monocentric study, in one major tertiary centre in Paris. Two cohorts of patients were compared; the first included patients before the use of antibodies, and the second included patients after the use of antibodies.
Participants All patients from the same physician diagnosed with a CD between 1976 and 1992 (historical cohort), and between 1994 and 2007, were included in the study. 56 patients were included in the historical cohort, 59 in the recent cohort.
Primary and secondary outcome measures Clinical, biological and histological profiles at diagnosis have been studied.
Results The recent cohort diagnosis of CD was based in 27% on a systematic screening (type I diabetes, n=10; CD in siblings, n=6). On comparison of CD patients in the historical to the recent cohort, the following significant differences were observed: Median age at diagnosis increased from 1 year to 2.7 years (p<0.0001). Patients in the historical cohort had more gastrointestinal symptoms (93% vs 63%, p=0.0001) and failure to thrive (98% vs 80%, p=0.0025). Nutritional deficiencies and morphological lesions were more severe in the historical cohort (90% subtotal or total villous atrophy vs 51%, p<0.0001). Differences observed between the two cohorts were mainly due to the presence of screened patients.
Conclusions A new type of patients, with a paucisymptomatic or asymptomatic CD, has been identified using serological tests. Silent disease has been diagnosed by screening in a target population. In the other patients of the recent cohort, symptoms were similar but less severe than those observed before. Long-term risks of untreated silent CD are not well determined as yet, and have to be evaluated in prospective studies.
- child
- serological tests
- screening
- gluten-free diet
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
The discovery in the early 1990s of antiendomysial (EM) and antitransglutaminase (tTG) antibodies has changed the diagnostic conditions of coeliac disease (CD), formerly based on three sequential biopsies.
-
The aim of this unicentre retrospective French study was to evaluate the impact of the use of serological tests in the diagnostic conditions of CD in children.
-
All children treated for CD in one centre in Paris (Necker Hospital) before the use of antibodies (historical cohort) and after (recent cohort), were included in this retrospective study. Clinical, biological and histological profiles at diagnosis have been studied.
Key messages
-
In the recent cohort, diagnosis of CD was based in 27% on a systematic screening.
-
On comparison of CD patients in the historical to the recent cohort, we observed an increase in the median age at diagnosis from 1 to 2.7 years, and a decrease in the prevalence of gastrointestinal symptoms and failure to thrive. Nutritional deficiencies and morphological lesions were more severe in the historical cohort. Differences observed between the two cohorts were mainly due to the presence of screened patients.
-
A new type of patients, with a paucisymptomatic or asymptomatic CD, has been identified by the use of serological tests. Silent and latent disease has been diagnosed by screening in a target population. In symptomatic patients of the recent cohort, symptoms were similar but less severe than those historically observed.
Strengths and limitations of this study
-
This study is the first one in France that determines the profile of CD in children since the use of serological tests.
-
It comprised limits inherent in retrospective studies, especially the presence of missing data, and the existence of an eventual recruitment bias in a very specialised centre like the Necker Hospital. The two cohorts have, however, been exposed to the same recruitment bias.
Introduction
The discovery in the early 1990s of antiendomysial (EM) and antitransglutaminase (tTG) antibodies has changed the diagnostic conditions of the disease, formerly based on three sequential biopsies.1 ,2
Recent epidemiological studies have observed a higher incidence of coeliac disease (CD) compared to what was known before. The prevalence of all forms of CD would be about 10-fold more than what was initially assessed.3 A prospective study conducted in France in 1994 had estimated the annual incidence of the symptomatic form of childhood CD to 1/2500.4 The prevalence of CD, all forms included, is actually estimated between 1/100 and 1/400 depending on the country.5 In France, there is currently no study that has evaluated this prevalence in children.
Since the initial Finnish study that showed the modifications of presentation of CD in children since the use of serological tests in the 1980s,6 similar results have been obtained in several European and North-American studies.7–9 However, no such study has been fulfilled in France.
The aim of this study was to measure in children the impact of the use of serological tests on the presentation of CD at the time of diagnosis and to answer to the question as to whether it is the appearance of symptomatic forms that has changed, or whether serological tests have given rise to certain forms of the disease that were not diagnosed earlier. We carried out a retrospective monocentric study to analyse the clinical, biological and histological presentation of the disease at the time of diagnosis in the two cohorts of children. The first one was constituted by patients who had a CD diagnosis before the use of serological tests (between 1976 and 1992), and the second one after their widespread use (from 1994 to 2007).
Material and methods
Patients
All children treated by the same physician at Necker Hospital (Paris, France) for a CD diagnosis made between 1 January 1976 and 31 December 1992 (historical cohort), and between 1 January 1994 and 31 December 2007 (recent cohort), have been initially considered. The inclusion period initially planned for the first cohort was from 1977 to 1987. However, some medical charts of this period were missing. To have a sufficient number of patients in the historical cohort, close to the number of patients in the recent cohort, we have extended the inclusion period by 1992.
All children were younger than 15 years of age at the time of diagnosis. Only patients who had a histological proof of diagnosis were included.
Data collection and analysis
Data were collected retrospectively, from information contained in medical records. Circumstances of diagnosis of CD were noted, as well as clinical, biological and histological information at the time of diagnosis. Collection of data included patient gender, age at diagnosis, the growth curve (failure to thrive was defined as a loss of more than 1 DS in weight or height) and initial symptoms. The presence of other diseases associated with CD, especially autoimmune diseases, was noted, as well as identification of CD in first-degree relatives. Biological abnormalities at diagnosis (anaemia, folic acid deficiency, selective IgA deficiency) were collected when they were available in the medical charts. Small intestine biopsies were collected with Crosby's capsule in first patients of the historical cohort, then since the end of the 1980s through an upper gastrointestinal fiberendoscopy. Morphological lesions compatible with a CD were divided into four groups, considering one of the classification commonly used to evaluate the severity of villous atrophy: normal villus−crypt ratio (>2) but hypercellularity in the lamina propria and increased number of intraepithelial lymphocytes (IEL) (>30 IEL for 100 enterocytes), partial villous atrophy (PVA, 1≤villus−crypt ratio ≤2) and subtotal (STVA, villus−crypt ratio <1) or total villous atrophy (TVA, flat mucosa).
Statistical analyses
Statistical analyses were made with the help of GraphPad Prism 5 and Microsoft Office Excel 2003 software. The results of the median values were accompanied by values of 25th and 75th percentiles (P25 and P75), or sometimes by extreme values. The results of the averages were accompanied by 95% CI.
The two cohorts were considered as unpaired samples. Pearson's χ2 test was used to analyse qualitative variables, or Fisher's exact test if the number of patients in subgroups was insufficient. For quantitative variables, Mann-Whitney test was employed to compare the two cohorts. α Risk threshold (mentioned as ‘p’) was set in the whole study at 0.05.
Results
Demographic data
In all, 56 patients were included in the historical cohort, 59 in the recent cohort. Among the 59 patients of this latter, 43 were suspected because of clinical symptoms (‘symptomatic’ patients), and 16 (27%) were screened in an evocative familial or autoimmune context (‘screened’ patients). Among these 16 patients, CD was searched because of a type I diabetes in 10 patients, and because of a CD in siblings in 6 patients.
Age at diagnosis
The median age at diagnosis increased from 1 year (extremes 0.6–8) in the historical cohort to 2.7 years (0.8–14) in the recent one (p<0.0001, table 1). If considering only symptomatic patients of the recent cohort, the median age at diagnosis was 1.8 years as against 9 years in screened patients only (p<0.0001).
Age and clinical presentation at the time of coeliac disease (CD) diagnosis in the historical (1976−1992) and recent (1994–2007) cohort of patients
Gastrointestinal symptoms
Totally 93% of patients (52 of 56) in the historical cohort had gastrointestinal symptoms at diagnosis, against 63% of patients (37 of 59) in the recent cohort (p=0.0001; table 1). Diarrhoea, the most typical symptom in CD, was more frequent in patients of the historical cohort than of the recent one (84% as against 47%, p<0.0001). If considering the symptomatic patients of the recent cohort, 32 patients of 43 (74%) had gastrointestinal symptoms at diagnosis. The difference with patients of the historical cohort remained significant (p=0.02). Among these 32 children, 27 had diarrhoea (p=0.01). Among the 16 screened patients, 4 were not completely asymptomatic: diarrhoea was observed in 1 patient, and abdominal pain or constipation in the others.
Failure to thrive and other signs of malnutrition
Failure to thrive was more often observed in patients of the historical cohort than in the recent one (table 1). However, if considering only the symptomatic patients in the recent cohort, the difference was not significant anymore (p=0.6). At the time of diagnosis, 50% (28 of 56) of children in the historical cohort had extraintestinal symptoms, especially clinical signs of malnutrition, against 17% in the recent cohort (p=0.0003). Altogether, among the 16 screened patients in the recent cohort, 8 were totally asymptomatic at diagnosis (‘silent’ patients), 7 were paucisymptomatic. The last patient, screened in a context of the discovery of a type I diabetes, had diarrhoea and severe failure to thrive, but it was not possible to identify if these symptoms were due to the diabetes or to the CD.
Biological abnormalities
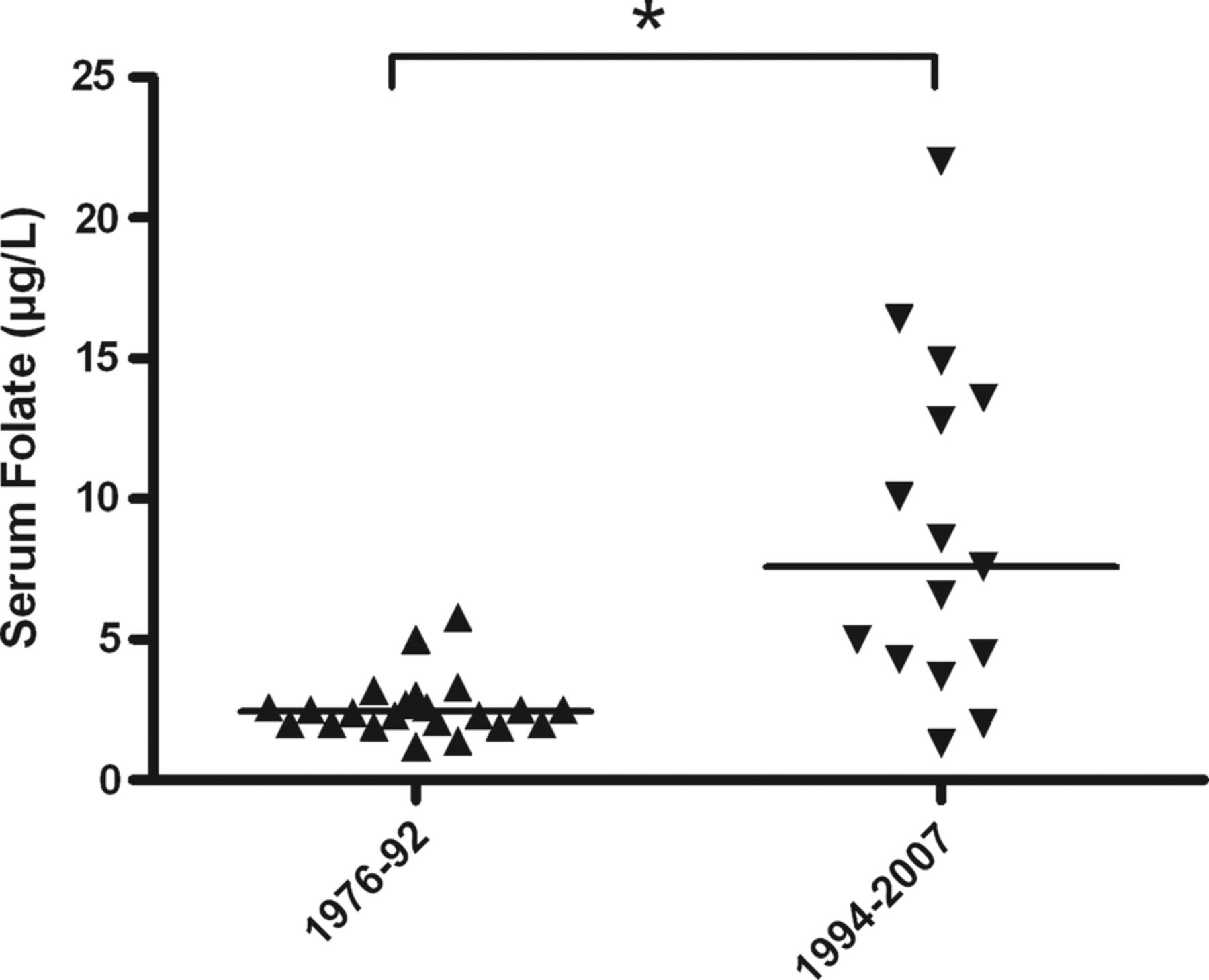
Serum folic acid and haemoglobin levels were significantly lower in patients of the historical cohort than in the recent one (p<0.01; figures 1 and 2). One patient of the historical cohort had a partial IgA deficiency, associated with hypogammaglobulinaemia (table 1).
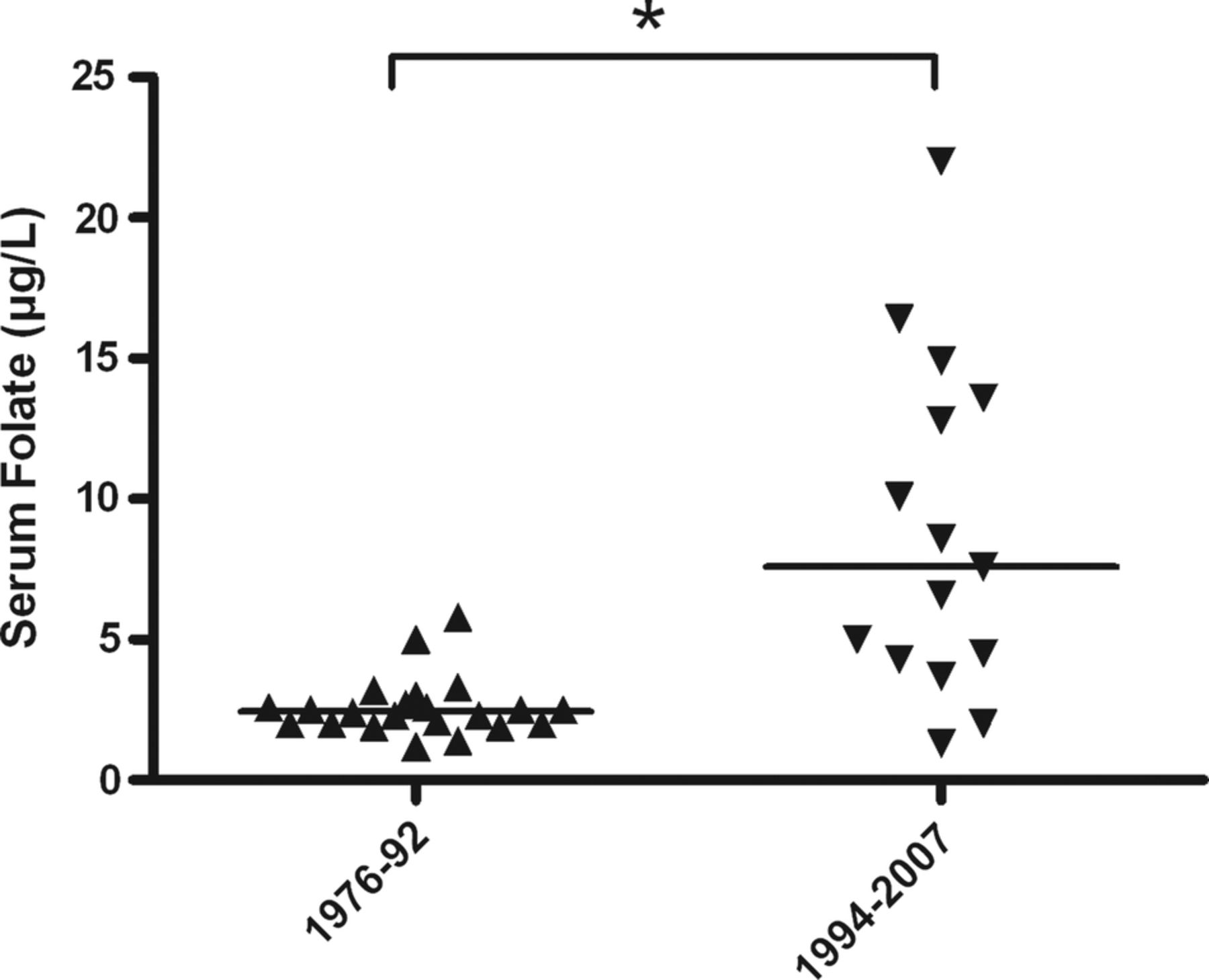
Serum folate levels (μ/l) at time of diagnosis in patients of the historical cohort (1976–1992, ▴) and of the recent one (1994–2007, ▾).

Serum haemoglobin levels (g/dl) at time of diagnosis in patients of the historical cohort (1976–1992, ▴) and of the recent one (1994–2007, ▾).
Morphological lesions
Among the 51 patients of the historical cohort for which morphological results were available at the time of initial care, 5 patients (10%) had a PVA, and the remaining 46 had severe lesions of STVA or TVA (figure 3). In the recent cohort, 1 patient had no villous atrophy, but showed hypercellularity in the lamina propria and an increased number of IEL, 28 patients (47%) had a PVA and 30 patients (51%) a STVA or a TVA. Finally, there were significantly more severe morphological lesions (STVA or TVA) in patients of the historical cohort than in patients of the recent one (p<0.0001). In the latter, lesions of PVA were predominantly observed in screened patients: actually, 11 of 16 screened children (69%) had a subnormal mucosa or a PVA, as against 18 on 43 symptomatic patients (42%). The difference was however not significant (p=0.07).

{kind=link}
{kind=link}
{kind=link}
Morphological lesions at time of diagnosis: results compared between patients of the historical (1976–1992) and recent (1994–2007) cohort, depending on the severity of lesions: normal mucosal morphology (but increased number of intraepithelial lymphocytes (IEL)). PVA, partial villous atrophy; STVA, subtotal villous atrophy; TVA, total villous atrophy.
Familial history and associated diseases
The presence of other diseases, especially autoimmune diseases, in patients, or of CD in first-degree relatives, is summed up in table 1.
Initial diet
A gluten-free diet has been initiated in all patients of the historical cohort as soon as the diagnosis was morphologically confirmed, because all of these patients were symptomatic. Among patients of the recent cohort, the eight silent patients were left on a normal diet after discussion between the physician and the patient and his family, and always only if they agreed to do so. The 51 other patients started a gluten-free diet. The patients left on a normal diet were regularly followed, at least twice a year for physical examination, and once a year for biological monitoring. A bone densitometry was performed if possible every 2 years. Patients who went on a gluten-free diet were also regularly clinically and biologically followed. At the time of data collection, none of the eight silent patients left on a normal diet had to start a gluten-free diet.
Gluten challenge
A gluten challenge was performed in 55 patients of the historical cohort (98%), against only 20 patients in the recent cohort (39%). This challenge was most often made several years after the diagnosis, not to confirm this one but to check if the gluten sensitivity was always there.
The median age at the time of gluten reintroduction was higher in the recent cohort than the historical one (6–4 years, table 2).
Age of patients at the time of gluten reintroduction and relapse modalities in patients of the historical (1976−1992) and recent (1994–2007) cohort
Until the end of follow-up, the relapse rate was not different in the two groups (table 2). The more frequent grounds for relapse were gastrointestinal symptoms or failure to thrive. Among the patients of the historical cohort who have clinically well tolerated the gluten challenge, six have normalised their morphological results (latent disease). EM and antigliadin IgA were checked in four patients among the six, and were negative in the four cases.
The patients who have been allowed to follow a normal diet were closely watched over to check the tolerance of this diet. They were submitted to a clinical examination every 6 months, with growth monitoring, to a biological check-up every year (complete blood count, serum iron and folate, serum vitamin levels, albuminaemia, SGOT/SGPT) and to an x-ray absorptiometry every 2 years. The level of antitransglutaminase IgA was measured every year, but biopsies were rarely performed. The patients were considered as ‘silent’, and thus allowed to continue a normal diet, when all those tests were normal (except the level of serological tests).
Discussion
This study compared two cohorts of children with a diagnosis of CD made respectively before or after the widespread use of anti-TGt and anti-EM antibodies. Therapeutic and follow-up strategies for patients in the two cohorts during both periods were similar. This study contains some limits inherent in retrospective analyses, especially the presence of missing data, and the existence of an eventual recruitment bias in a very specialised centre like the Necker Hospital. However, the two cohorts have been exposed to the same recruitment bias, because both were cohorts from the same tertiary centre.
A new type of patients has been identified in the recent cohort, diagnosed by screening in people at risk: type I diabetes in the patient or CD in siblings. These screened children represented more than a quarter of patients in the recent cohort. The median age at diagnosis has almost tripled in this cohort compared to the historical one, predominantly owing to the higher age of screened patients. The age at diagnosis was however higher too in the symptomatic patients of the recent cohort than in patients of the historical one. This could be explained by the later administration of gluten in infants between the 1960s and the 1990s (from 3 to 4–6 months), that could postpone the symptoms revealing CD.10 ,11 In the recent cohort, patients had a milder clinical picture at diagnosis than those of historical cohort, with less frequent gastrointestinal symptoms. Half of the screened patients were really asymptomatic, and the other part had often subtle but evocative clinical signs, like diarrhoea or growth abnormalities. Failure to thrive was less frequent in the recent cohort compared to the historical one. Finally, differences between clinical symptoms observed in the two cohorts were predominantly due to the milder symptoms observed in the screened patients, while symptomatic patients in the recent cohort had a clinical picture similar to the one observed in the historical cohort. Biological abnormalities like anaemia and folic acid deficiency were less marked in patients of the recent cohort than in the historical cohort. Furthermore, morphological lesions were less severe in the recent cohort, and the difference was still here due to the milder lesions observed in the screened patients.
At the time of the study, some paediatric gastroenterologists thought that silent patients could be maintained on a normal diet if they were regularly followed. This attitude has been chosen by the physician following the patients included in this study.
Indeed, several studies have now shown that the risk of cancer in coeliac patients is not proven in children, and that in adults it comes back to normal after 5−10 years of gluten-free diet.12 ,13 The impact of a gluten-containing diet compared with a gluten-free diet on the risk to develop other autoimmune diseases remains discussed.14 ,15 At last, a recent study showed that fertility in women is decreased in the 2 years preceding CD diagnosis, but comes rapidly back to normal after starting a gluten-free diet.16 At the time of data collection, the eight silent patients were submitted to a strict regular follow-up, and all their clinical, biological and radiological tests were normal.
The results of our study show that the clinical, biological and morphological presentation of CD has been transformed since the use of serological screening tests, owing to the discovery of new clinical forms of the disease, especially the silent form. The typical form of the disease still exists and has hardly changed, but it represents now only a minor part of the patients. New patients, who were not diagnosed by the physicians before, are older and paucisymptomatic or asymptomatic. These changes in the clinical presentation of the disease have already been observed in several European countries6–8 ,17 ,18 but the impact of the screened patients in these changes was not clearly identified. Recently, similar results have been obtained in North America.9
In conclusion, the widespread use of serological screening tests in the early 1990s has changed the presentation of CD at the time of diagnosis. This has led to an important increase in the prevalence of the disease, without any change in the disease itself. The discovery of silent forms of the disease has affected the face of the disease, raising the question of the systematic indication of a gluten-free diet in children with silent CD. In the future, new therapeutic strategies, as oral enzyme administration capable of helping gluten digestion, could modify the management of CD.
References
Footnotes
-
Contributors HGL, NB, SC, OG, FMR and JS contributed to the conception and design of the study. HGL and JS contributed to the acquisition of data and performed the statistical analysis. HGL, OG, FMR and JS contributed to the analysis and interpretation of data. HGL, JS and FMR contributed to drafting the article. HGL, NB, SC, OG, FMR and JS contributed to revising the article critically for important intellectual content and final approval of the version to be submitted.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Ethics approval This study is a retrospective study.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.