Article Text

Abstract
Objectives The present study attempts to identify appropriate elements that may contribute to clarify the broad clinical features (diagnosis, care, complication and prognosis) of Takotsubo-like cardiomyopathy for improving its management.
Design study Observational study.
Setting Primary level of care referred to the emergency department of Vannini Hospital, Rome, Italy.
Participants The study population consisted of 75 patients, 72 of the them were women and 3 were men with a mean age of 71.9±9.6 years.
Methods From February 2004 to November 2010, prospectively included 84 consecutive patients diagnosed for suspected Takotsubo-like cardiomyopathy. To be eligible, patients had to meet all the Mayo clinic criteria in the absence of neurological trauma or intracranial haemorrhage. Moreover, those patients that at follow-up still presented alteration of acute phase at ECG and echocardiogram were excluded. Thus, 75 patients comprised the study population. To follow-up 19 patients were lost.
Results None of 75 patients died in acute phase. All patients were promptly discharged (8.4±4.4 days), since they recovered their normal functional status without symptoms. Follow-up information was available for 56 patients. At a mean follow-up time of 2.2±2 years (range, 0.1–6.8 years) two octogenarian patients (2.6%) died because of sudden cardiac death and pulmonary embolism, respectively. The Takotsubo-like cardiomyopathy recurred in one patient.
Conclusions The results of this study support the previous reports about the good prognosis, also in critically ill patients, of Takotsubo-like cardiomyopathy. Further assessment will be needed to determine a careful and sustained follow-up for choosing the best care and foreseeing the recurrences of this emerging condition.
- apical ballooning
- stress
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
The present study attempts to identify appropriate elements that may contribute to clarify the broad clinical features (diagnosis, care, complication and prognosis) of Takotsubo-like cardiomyopathy (TC) for improving its management.
-
Only few studies have followed patients after hospital discharge.
-
The aim of the current study is, also, to define more completely the broad clinical features, recurrence and survival, after hospital discharge.
Key messages
-
The prognosis of patients with TC, in our study, is as good in acute phase as in follow-up and the recurrence is low.
-
It is unclear why recurrences of TC do not occur when similar stressful circumstances occur again after the initial episode.
-
The treatment for patients with TC in acute phase and in follow-up is not established yet.
Strengths and limitations of this study
-
Strengths of our study are a mean follow-up time of 2.2±2 years (range 0.1–6.8 years) and the number of patients in follow-up.
-
Our results must be considered in the light of some study limitations: (1) this study was observational and (2) it was performed at a single centre.
Background
Takotsubo-like cardiomyopathy (TC) is an enigmatic cardiomyopathy, characterised by a reversible left ventricular (LV) dysfunction triggered frequently by physical or emotional stress, mimicking an acute coronary syndrome (ACS).1–7
This is characterised by transient wall-motion abnormalities involving apical and/or mid-portions or basal segments of the left ventricle in the absence of significant obstructive coronary disease or, conversely, in the presence of stenosis not related to the myocardial-involved region.8–13 Affected patients are generally postmenopausal women, whose symptoms and ECG changes mimic an acute myocardial infarction (AMI). However, the release of the myocardial enzyme is limited if compared with the extent of LV dysfunction. Moreover, the ECG does not reproduce the typical evolution of an AMI because ST elevation or ST depression, prominent negative T waves with long QT interval, and Q waves disappear in the follow-up.14–16 The lack of history of cardiac disease, and the reversibility of ventricular dysfunction make this syndrome very difficult to explain from a pathophysiological point of view. Mortality and complication are extremely low if compared with either AMI-related in-hospital or out-of-hospital 1-year mortality. Prior reports suggest that TC accounts for 1.5–2.2% of patients presenting with symptoms that initially appeared to be an ACS. Furthermore, it has been estimated that as many as 6% of women presenting with an apparent ACS may actually have TC.17 Several pathophysiological mechanisms have been proposed. However, the real aetiology has yet to be defined. Moreover, only few studies have followed TC patients after hospital discharge and the follow-up of TC has been poorly described. The aim of the current study was to assess the recurrence rate of TC after initial presentation and define more completely the broad clinical features of this recently recognised condition.
Methods
The study population consisted of 75 patients referred to the emergency department of Vannini Hospital; 1.3% of all patients presented ACS, between February 2004 and November 2010. TC was diagnosed according to the Mayo clinic criteria (box 1) and the patients did not have neurological trauma or intracranial haemorrhage. Moreover, those patients that at follow-up still presented alteration of acute phase at ECG and echocardiogram were excluded. Echocardiograms were performed in a standard fashion to assess the LV systolic function and wall motion abnormality at presentation and follow-up in all patients.18 LV ejection fraction was determined using the modified Simpson rule; absence of significant coronary artery disease as assessed by angiograms, an ST-segment elevation and an ST-segment depression were defined as deviation >1 mm in amplitude in more than two contiguous leads and deep T-wave inversion was defined as inversions >3 mm in amplitude in at least three contiguous leads. All other ECG changes that did not fulfil these criteria were grouped under non-specific ST/T-wave changes. QT interval was defined as the interval from the beginning of the QRS complex to the end of the T wave and was corrected for heart rate by Bazett's formula. Blood samples for measurement of troponin T levels were obtained on admission and at 3 h intervals during the first 24 h, and then daily until discharge. Clinical, ECG and echocardiographic follow-up were completed at a median follow-up time 6 months from the event. Categorical variables are expressed as number and percentage. Normally distributed variables are presented as mean±SD.
The Mayo clinic criteria
-
Transient akinesis or dyskinensis of the left ventricular apical and mid-ventricular segments with regional wall-motion abnormalities extending beyond a single epicardial vascular distribution.
-
Absence of obstructive coronary disease or angiographic evidence of acute plaque rupture.
-
New ECG abnormalities (either ST-segment elevation or T-wave inversion).
-
Absence of:
-
Recent significant head trauma.
-
Intracranial bleeding.
-
Pheochromocytoma.
-
Obstructive epicardial coronary artery disease.
-
Myocarditis.
-
Hypertrophic cardiomyopathy.
-
Results
Seventy-two of the patients were women and 3 were men with a mean age of 71.9±9.6 years; 53 (70.6%) presented a history of hypertension, 20 (26.6%) of hypercholesterolaemia, 22 (29.3%) of disthyroidism, 12 (16%) of diabetes mellitus and 14 (18.6%) of tobacco use. No patient had previous or a family history suggestive of TC.
The most common presenting cardiovascular symptoms were substantial chest pain (n=48; 64%), in these patients the ECG, on admission, showed: ST-segment elevation (n=28), diffuse ST-segment depression (n=4), T-wave inversion (n=11), left bundle brunch block (n=1) and non-specific abnormality (n=4). In the patients who went with exertional dyspnoea (n=11; 14.6%), the ECG showed an ST-segment elevation (n=6), a diffuse ST-segment depression (n=1), T-wave inversion (n=2) and non-specific abnormality (n=2). The remaining 16 (21.3%) patients were identified during the management or monitoring of non-cardiac conditions.
Based on the presentation suggestive of TC, patients were asked whether a stressful event had preceded the admission. There were identifiable precipitating events in 62 (82.6%) of them (table 1), but 13 patients (17.3%) did not have any identifiable stressor at time of presentation.
Emotional and physical stressors triggering TC
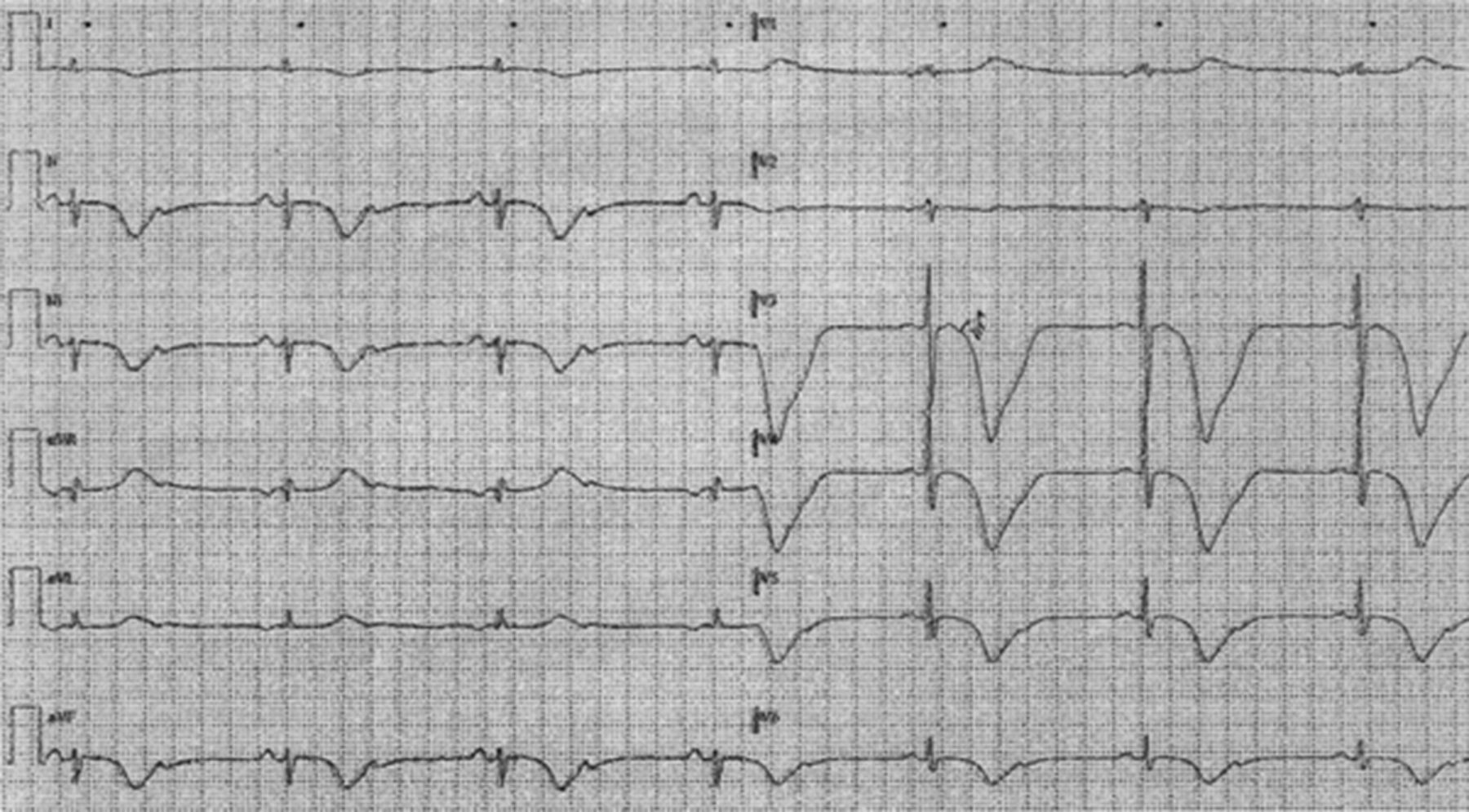
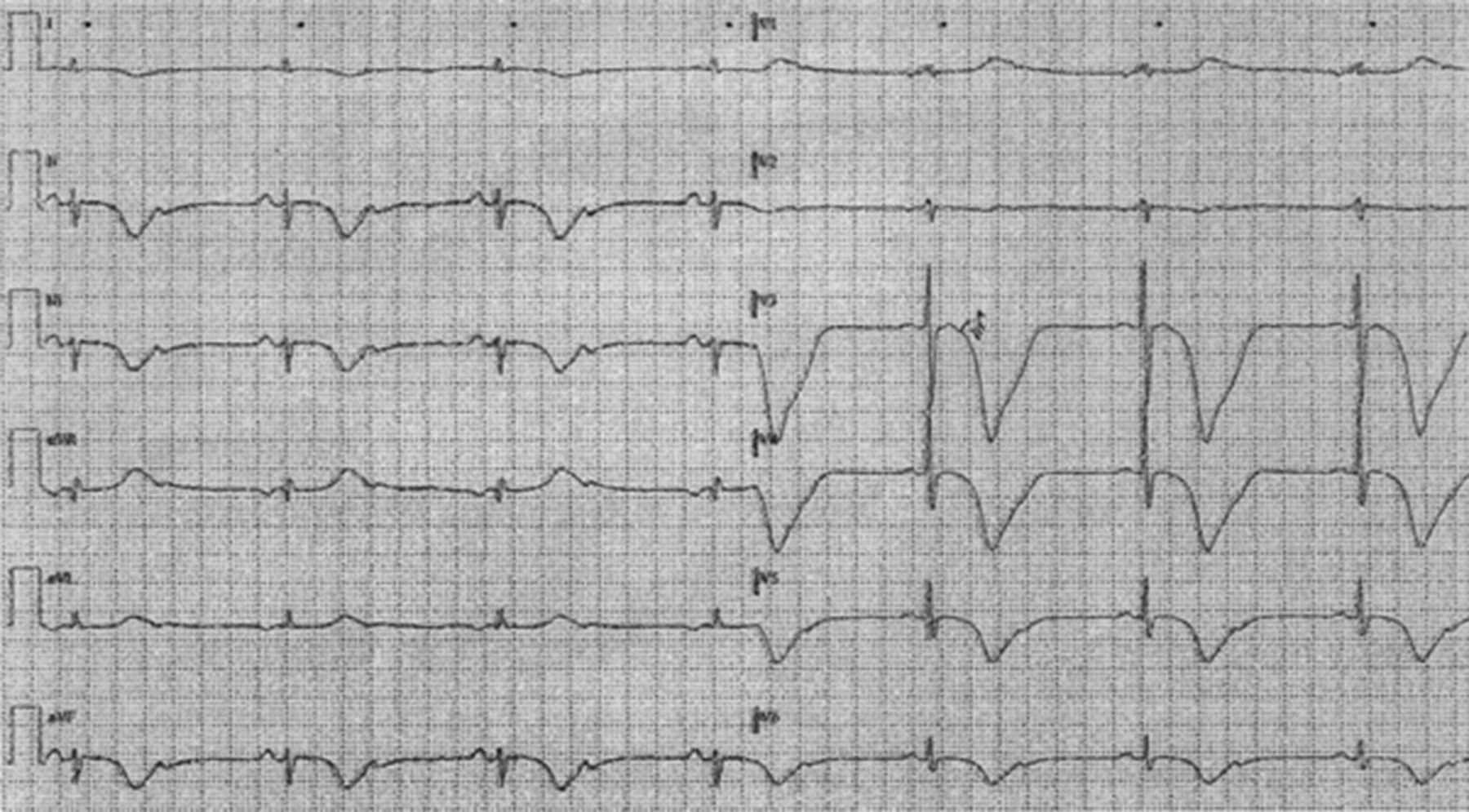
In the acute phase, the patients had a QTc interval of 503.8±61.7 (range 378–680 ms). In 64 patients, QTc interval was ≥450 ms (figure 1); the prolongation occurred within 48 h after the onset of symptoms and was associated with deep and symmetric T-wave inversion in most leads. In 10 patients, deep and symmetric T-wave inversion appeared, but QTc interval was normal. Only in one patient with the basal ballooning, variant broad upright T waves and normal QTc in subacute phase were observed. Despite significant prolongation of the QTc, no patient developed torsades de pointes (TdP), ventricular tachycardia (VT) and/or ventricular fibrillation (VF). Therefore, long QT triggering ventricular arrhythmias appear to be highly infrequent, although VT/VF have been reported at the time of presentation as well as delayed complications of this syndrome.
ECG at the second day showing widespread repolarisation abnormalities with QT interval prolongation and marked negative T wave.
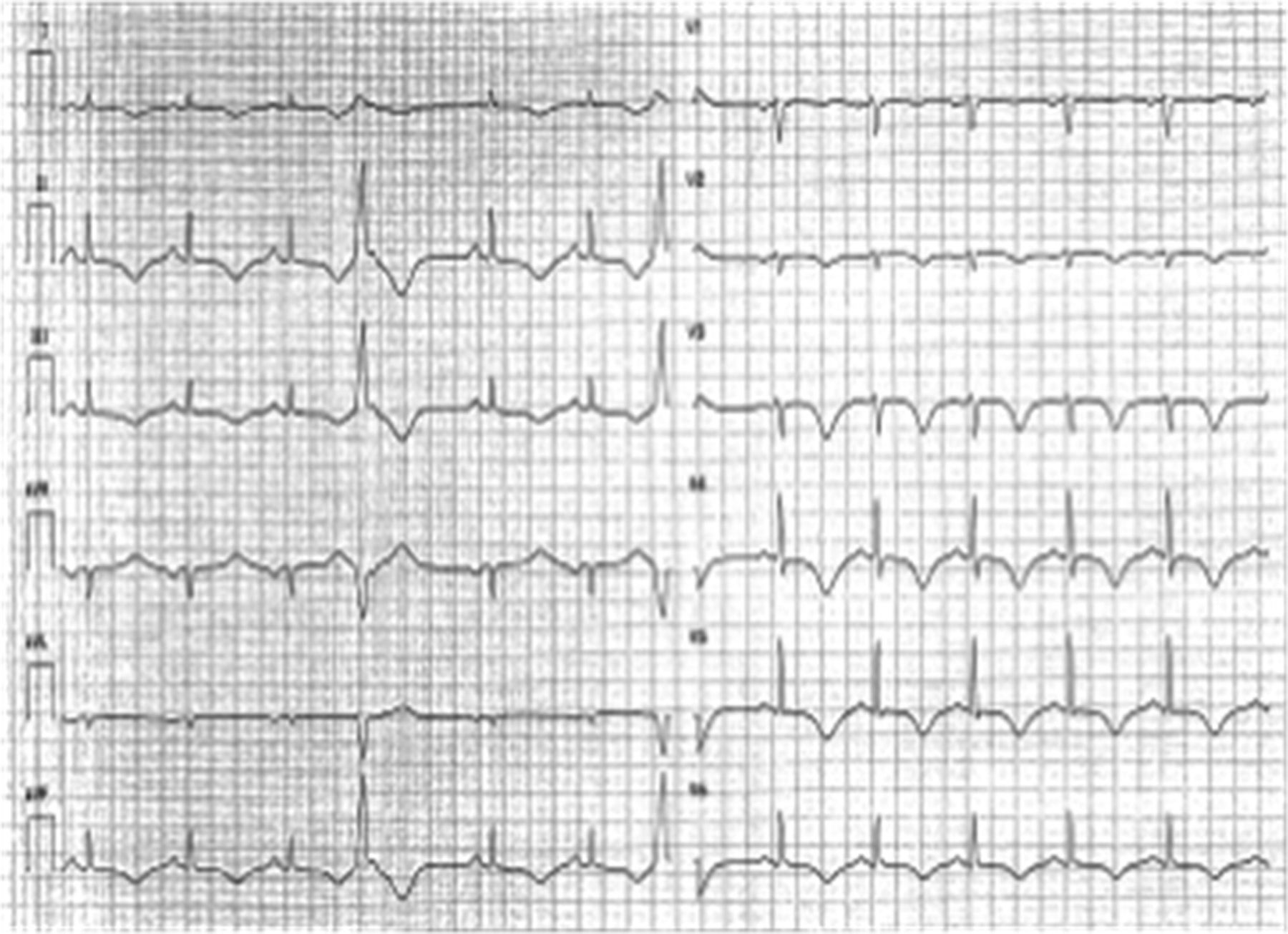
In acute phase, four patients had life-threatening arrhythmias: one patient presented with a cardiac arrest during non-cardiac surgery; three patients presented with second-degree atrioventricular block (figure 2); these patients subsequently required permanent pacemaker implantation. Eight patients had atrial fibrillation during hospitalisation (table 2).
Clinical characteristics

ECG showing atrioventricular block 2 : 1 with deep T-wave inversion and QTc interval prolongation.
Mean echocardiographic left ventricle ejection fraction, assessed in the acute phase, was 37.2%±9.05%. The prevalent regional wall motion abnormalities involved hypokinesis or akinesis of the mid and apical segments of the left ventricle; also one patient with situs viscerum inversus had this features.19 In five patients, there was preserved function of the apex and basal segments with wall motion abnormality that involved the mid-segments. In only one patient, there was a rare variant present with hypokinesis or akinesis of the mid and basal segments of the LV with preserved apical function. Also, the variant with biventricular involvement were present in one patient.20 ,21 Importantly, the wall motion abnormality typically extends beyond the distribution of any single coronary artery. Intraventricular apical thrombosis was identified in one patient (figure 3).22–24

Cardiac MR in the early phase of takotsubo-like cardiomyopathy showing apical akinesis with thrombosis (arrow).
In the acute period, only 1 of 75 patients developed dynamic obstruction to LV outflow (gradient >30 mm Hg) owing to systolic anterior motion of the mitral valve leaflets with chordal apparatus and mitral–septal contact. This outflow obstruction resolved in the subacute period.25 ,26
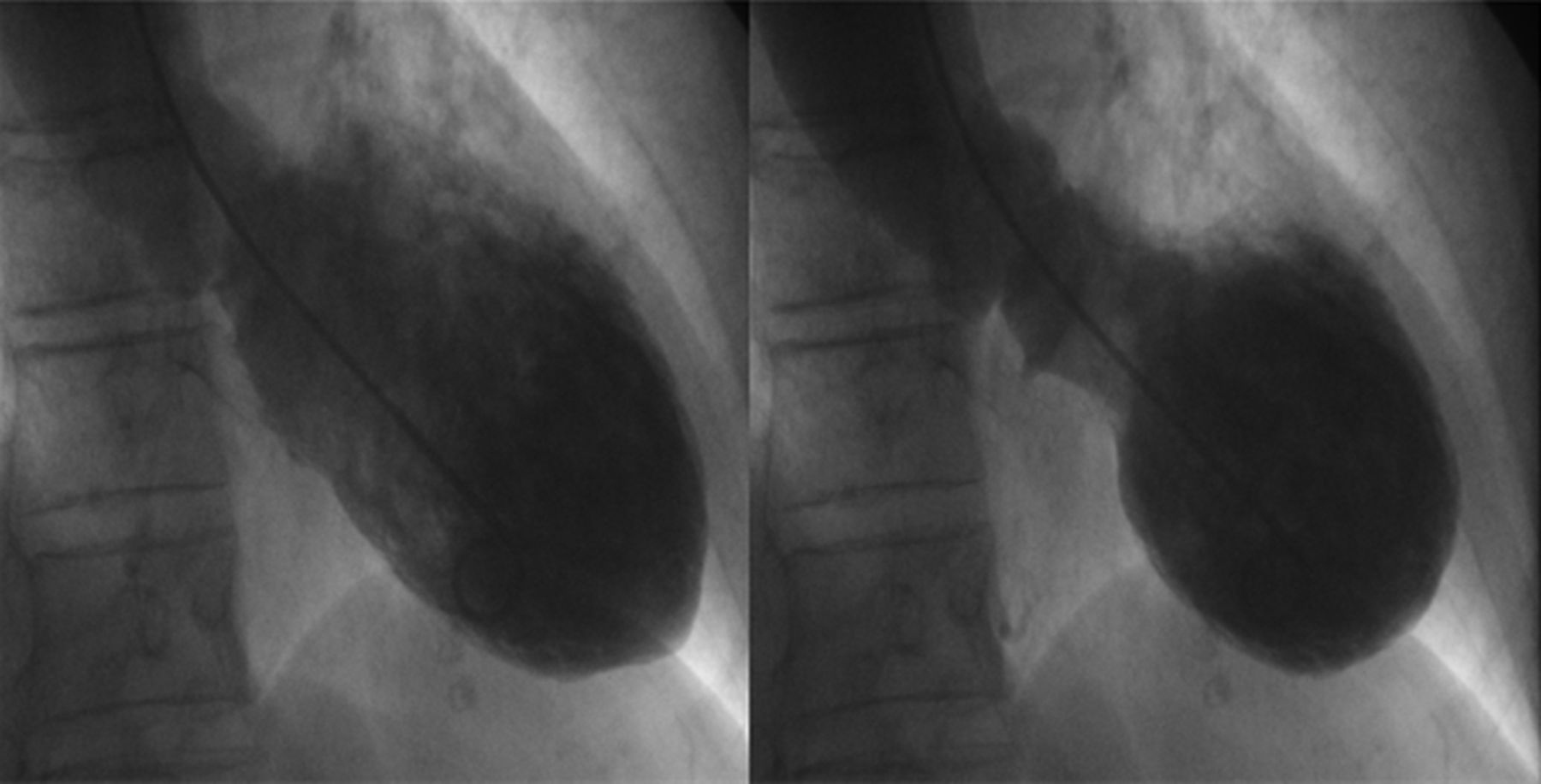
The interval between the door of the hospital and coronary angiography was 90 min in 32 patients and 36 h in 43 patients. Coronary angiography at initial evaluation indicated normal coronary arteries in 61 patients and mild stenoses (<50%) in 24 patients. Concomitant LV angiogram was performed in 42 patients (56%) (figure 4). Congestive heart failure occurred in nine patients and cardiogenic shock in 1, intra-aortic balloon pumping was required in one patient, while the dopamine was used in only two patients.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
End-diastolic and end-systolic frame of left ventriculography showing anterolateral, anteroapical and inferior apical wall dyskinesia with hypercontractility of the basal segments.
Cardiac MR was performed in only 21 patients within 10 days after their admission. Delayed gadolinium hyperenhancement was absent in all patients.27 ,28
None of the 75 patients died; all patients were promptly discharged (8.4±4.4 days), since they recovered their normal functional status without symptoms, echocardiographic left ventricle ejection fraction, on discharge, was 50.5%±7.76%. On discharge, all patients had the QTc interval ≤450 ms.
At discharge, 73 patients (97.3%) received aspirin, 71 (94.6%) ACE inhibitors/angiotensin receptor blockers, 67 (89.3%) β-blockers, 42 (56%) diuretic and 51 (68%) received statins.
Follow-up information was available for 56 patients. The frequency of returns was variable. After a mean of 6 months of follow-up, in all 56 patients, the ECG had normalised and mean echocardiographic left ventricle ejection fraction was 58%±4. At a mean follow-up time of 2.2±2 years (range 0.1–6.8 years), two patients (2.6%) died because of sudden cardiac death and pulmonary embolism, respectively, 2 years after the episode of cardiomyopathy. These patients used aspirin, ACE inhibitors and β-blockers.
In follow-up, 47 patients (83.9%) received aspirin, 50 patients (89.2%) ACE inhibitors/angiotensin receptor blockers, 42 patients (75%) β-blockers, 8 (14.2%) diuretic and 36 (64.2%) statins.
The TC recurred in one patient after 1 month from the first episode. This patient at the moment of the second episode used only aspirin and did not use β-blockers and ACE inhibitors/angiotensin receptor blockers.
Antihypertensive therapy required to be increased in seven patients. A new episode of atrial fibrillation was observed in one patient.
Discussion
We describe our observational clinical experience over a period of 6 years on 75 patients who underwent sudden, unexpected, onset of a reversible LV dysfunction. The aim of this study is to increase knowledge about this syndrome because the clinical course following events after hospital discharge is still incomplete and only few studies have followed patients after hospital discharge.
The prognosis of patients with TC, in our study, is as good in acute phase as in follow-up because none of the 75 patients died in acute phase, and death occurred, during follow-up, only in two octogenarian patients. These findings compare favourably with the reported rates of in-hospital mortality of 9–10% in non-selected case series of myocardial infarction29 and these data confirm that survival is similar to that in an age-matched and gender-matched population. Also, previous reports confirm these data.30 Elesber et al31 show an excellent 4-year prognosis for patients with TC.32 Sharkey et al33 show in follow-up a higher mortality in follow-up, but those patients died from non-cardiac causes.
For the treatment of TC, we referred to the guidelines of STEMI patients, according to good clinical practice. Further prospective studies are needed on targeted therapies. Also in chronic phase, there is no established treatment. Data from an animal model of TC suggest that its development seems to be diminished after α-blockade and β-blockade.34 Thus, sympathetic activation is believed to contribute to the pathogenesis of TC and thus it is reasonable to consider that β-blockers should be given in the acute and chronic phases and may possibly help to prevent recurrences.35 ,36 However, Elesber et al, showed that TC recurred in 10 patients over a mean follow-up of 4.4±4.6 years, and there was no difference between the patients who did and did not have recurrence in the use of aspirin, ACE, inhibitors/angiotensin receptor blockers, β-blockers, and statins. Moreover, Sharkey et al33 showed that three of the seven patients were taking β-blocking agents at the time of their first recurrent SC event. In our series, only in one patient, TC recurred and this patient at the moment of the second episode was using only aspirin and was not using β-blockers and ACE nor inhibitors/angiotensin receptor blockers. Curiously, the patient did not have an identifiable precipitating event at first episode and at recurrence.
During follow-up, emotional stressors such as an unexpected death in the family, occurred in four patients but they did not have a recurrence of TC. It is unclear why recurrences of TC do not occur when similar stressful circumstances occur again after the initial episode. In these cases, the patients used β-blockers, ACE inhibitors and aspirin.
It is interesting to note that in our series, 70.6% of patients had hypertension, whereas only 16% were diabetic. In TC, dissociation between hypertension and diabetes, although described in the literature, has not yet been well recognised and it is still unclear why the incidence of hypertension is so high and, conversely, diabetes is so low. Moreover, a high percentage of patients (29.3%) showed hypothyroidism; also the exact role of thyroid hormones in this syndrome is still unknown.
Study limitation
Our results must be considered in the light of some study limitations. First of all, the study population had a small number of individuals then the treatment of the patients was empirical and may reflect treatment biases for which we cannot account or fully adjust. Moreover, this study was observational and performed at a single centre.
Conclusion
The results of this study support the previous reports about the good prognosis, also in critically ill patients, of TC. Further assessment will be needed to determine a careful and sustained follow-up, for choosing the best care and foreseeing the recurrences of this emerging condition.
References
Footnotes
-
Contributors Each author has given substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; has drafted the article or revised it critically for important intellectual content; and has final approval of the version to be published
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.