Article Text

Abstract
Objectives An increased risk of developing knee disorders including radiographic knee osteoarthritis (OA) have been shown among workers with kneeling working demands. There may also be a dose-related association between duration of employment in occupations with kneeling work and development of radiographic knee OA and magnetic resonance imaging (MRI)-detected meniscal tears and bursitis.
Design A cross-sectional study of a historical cohort.
Setting Members of the trade unions for floor layers and graphic designers in Denmark.
Participants 92 male floor layers and 49 graphic designers aged 36–70 years were randomly selected among participants from a clinical and radiographic study of 156 floor layers and 152 graphic designers.
Outcome measures Radiographic tibiofemoral (TF) and patellofemoral (PF) knee-OA and MRI-detected meniscal tears and bursitis. Results were adjusted for age, earlier knee traumas, sports activities and body mass index in logistic regression models. Association between TF OA and years in the floor-laying trade was graphically examined by a restricted cubic spline with four knots.
Results Increase in number of years with exposure to kneeling work is associated with radiographic TF knee OA with ORs 0.7, 95% CI 0.07 to 4.42; OR 1.89, 95% CI 0.29 to 12.3; OR 4.82, 95% CI 1.38 to 17 for <20 years, 20–30 years and >30 years of kneeling work, respectively. MRI-verified medial meniscal tears was increased among subjects with kneeling work with OR 1.96, 95% CI 0.79 to 4.88 to OR 4.73, 95% CI 1.16 to 19.4 but was not associated with duration of employment. Periarticular bursitis was increased in subjects with <20 years of kneeling working activity. Lateral meniscal tears and PF knee OA were not associated with duration of kneeling working activity or with kneeling work in general.
Conclusions The findings suggest a dose–response relationship for radiographic TF knee OA in floor layers with a significant amount of kneeling work and an increase of MRI-verified medial meniscal tears among workers with kneeling work.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
An increased risk of developing knee disorders including radiographic knee osteoarthritis (OA) have been shown among workers with kneeling working demands. Workers with kneeling working positions have an increased risk of developing knee complaints in a much higher degree than can be explained by osteoarthritis.
It is unknown if there is a dose-related association between duration of employment in occupations with kneeling work and development of radiographic knee OA including both tibiofemoral and patellofemoral knee OA.
It is unknown if MRI-detected meniscal tears and bursitis around the knees can explain some of the knee complaints in subjects with kneeling work.
Key messages
The study shows a dose-response relationship between the duration of employment in work with kneeling working positions and tibiofemoral knee OA but not of patellofemoral knee OA.
There is an increased risk of developing MRI-detected medial meniscal tears and periarticular bursitis among floor layers compared with referents, but it is not associated to long duration of employment.
The study suggests that other knee disorders than osteoarthritis may explain that floor layers have knee complaints.
Strengths and limitations of the study
Study strength includes investigation with both radiographic and MRI, the description of a variety of knee disorders and the long duration of exposure among study group.
Limitation is the small number of participants due to economic reasons by conducting MRI.
Introduction
Demonstration of exposure–response and exposure–effect relations is considered important in causal inference, and the risk of developing various knee disorders may depend on both the degree of daily exposure and years of exposure to kneeling and squatting work positions.
We have in previous studies described an increased risk of developing tibiofemoral (TF) osteoarthritis (OA) meniscal tears and bursitis among floor layers with high knee loads compared with referents without knee straining work.1–4 Floor layers install linoleum, carpet and vinyl floorings. The work tasks include removal of old flooring, grinding, filling, installation of underlay, measuring and cutting materials, gluing, welding and installation of skirting board. The floor layers in this study did not usually use knee kickers, they perform all kinds of work tasks and none solely installed carpets. Graphic designers did layout of text and advertisements and made up pages before printing of newspapers, weekly papers, books and other publications. They used visual display units, mostly while sitting. Their work did not include physically demanding or knee straining working positions. In an earlier study, we measured the amount of kneeling work positions used by floor layers and graphic designers, using video recordings of short time periods without pauses and with continuous video recordings. The cumulative duration of time spent in kneeling work positions in 1 day was 65% of the workday (SD 25%) for the discontinuous measurements5 6 and 41% (SD 7.5%) for the continuous measurements for floor layers.3 Graphic designers have no kneeling working demands.
Only few occupations are exposed to the same high level of knee demands as floor layers. All Danish floor layers have the same job functions. They are skilled and continue in the profession for many years. Hence, we can apply seniority in the profession as a proxy for the total amount of knee strain.
We have shown a trend towards an increased risk of TF OA increasing with duration of employment as a floor layer,3 but no association for meniscal tears.4
The purpose of this study was to analyse whether there is a dose–response relationship for the development of radiologically detected TF and patellofemoral (PF) OA, and magnetic resonance imaging (MRI) demonstrated meniscal lesions and various forms of bursitis measured by seniority in the profession as floor layers compared with a group of referents without knee straining work demands.
Materials and methods
Study sample
A source population of 286 Danish floor layers and 370 graphic designers was established in 1994 based on membership list from trade unions. Male members aged 36–70 years in 2004, who were living in the geographical area of Copenhagen (capital city) or Aarhus (second largest city), Denmark, were included in the study. Male workers, who were members of the trade union 10 years earlier, were also included. Graphic designers, all from Copenhagen, were included as a group of non-exposed. Their work tasks involved no knee demands. Danish floor layers and graphic designers are comparable regarding the level of education and socio-economic status. Questionnaires were mailed to the source population in years 2004–2005. The response rate was 89% and 78% among floor layers and graphic designers, respectively. The questionnaire included information on age, height, weight and years in the profession, knee complaints, knee traumas and sports activity. Questionnaire respondents were invited to participate in a clinical and radiographic investigation. Informed consent to participate was given by 156 floor layers and 152 graphic designers. Consent to perform a full radiographic examination (knees and pelvis) was given by 134 floor layers (Copenhagen=88; Aarhus=46) and 120 graphic designers (Copenhagen).3 Among those, a random sample of 92 (Copenhagen, n=45; Aarhus, n=47) floor layers and 49 graphic designers (Copenhagen) had a MRI of both knees (n=282). Examinations were conducted at two MR Centres over a 1-year period (2005–2006).4 Only the participants who have been included in both the MRI study and the radiological examination were included in the analysis of this paper. Permission was obtained from the Central Danish Region Committee on Biomedical Research Ethics.
MRI
MRI at centre I was performed by a 1.5-Tesla scanner (Symphony Vision; Siemens Medical Systems, Erlangen, Germany) in 47 patients and at centre II by a 1.5-Tesla scanner (Infineon; Philips, Best, The Netherlands) in 94 patients. The MRI sequences were identical for both the right and left knee. The following MRI sequences were obtained at centre I: sagittal proton density fat-saturated turbo spin-echo (TR/TE, 3300/15 ms) and sagittal and coronal T2-weighted (4000/86 ms) fat-saturated turbo spin-echo, coronal T1-weighted (608/20 ms) spin-echo sequences and axial proton density fat-saturated turbo spin echo (3450/15 ms). The section thickness was 4 mm with an intersection gap of 0.4 mm; field of view was 200×200 mm and matrix 512 in all sequences. At centre II, the MRI sequences included sagittal proton density fat-saturated turbo spin-echo (TR/TE, 2500/18 ms) and sagittal and coronal T2-weighted (4000/85 ms) fat-saturated turbo spin-echo and coronal T1-weighted (400/13 ms) spin-echo and axial proton density fat-saturated turbo spin echo (2880/17 ms). The section thickness was 4 mm with an intersection gap of 0.4 mm; field of view was 150×150 mm and matrix 512 in all sequences.
A musculoskeletal radiologist with substantial MRI experience evaluated each of the 282 MR examinations. The observer was blinded to any medical history of knee disorders among participants. Due to differences in the appearance of MRI form the two centres, blinding of occupational affiliation was incomplete regarding participants from centre I, who were all floor layers. Blinding of occupational affiliation was complete concerning all participants from centre II. The medial and lateral meniscus of each knee was evaluated separately for abnormalities. Abnormalities in the MR signal intensities predicting degenerative tears were divided in grades 1–3.4 The presence of bursitis was assessed in both knees of each participant. Bursitis was registered in the following bursae: subgastrocnemius, semimembranosus–gastrocnemius, anserine, lateral (LCL) and medial (MCL) collateral ligament, iliotibial, prepatellar, superficial infrapatellar, deep infrapatellar bursae, and extracapsular synovial cysts Rytter et al.7
Radiographs
Radiological examinations of both knees were obtained in the standing weight-bearing position with the knee in 20–30 degree flexion in three views: posterior–anterior (PA), lateral and axial of the PF joint space. Radiographs were read and scored on workstations with 2K screens by one experienced musculoskeletal radiologist unaware of any medical history of knee disorders among all participants and blinded to occupational affiliation concerning the participants from Copenhagen. The radiographic scoring comprised assessment of the medial and lateral joint spaces of both the TF and PF compartments using a modified Ahlbäck scale (grades 0–6) of joint space narrowing (JSN) and subchondral bone attrition. The following grades of JSN were defined: grade 0 = normal; grade 1 = minimal but definite narrowing (25% JSN); grade 2 = moderate narrowing (50% JSN); grade 3 = severe narrowing (75% JSN); grade 4 = obliteration of the joint space, ‘bone on bone but no attrition’; grade 5=<5 mm attrition of subchondral bone and grade 6=≥5 mm bone attrition.3 Knee OA was defined as JSN ≥25% in at least one knee and patterns of involvement categorised into medial or lateral TF OA and PF OA.
Data analysis and statistics
We have in earlier studies shown that there were only small variations in the degree of knee straining work activities among the different work tasks in floor layers.5 6 Duration of employment for floor layers has therefore been used as a proxy for the exposure to knee straining work positions in the analyses of the study and categorised into three groups (≤20, 21–30, >30 years). Results for each of the three groups were compared with the group of graphic designers in total with no exposure to kneeling work activities. The association between the duration of employment in the trade and the development of TF and PF OA (≥25% JSN), meniscal tears (grade 3) and bursitis was analysed among floor layers relative to graphic designers. The adjusted OR with 95% CI was computed, and independent variables incorporated in the model of adjusted results were age, body mass index (BMI), knee straining sports and earlier knee traumas. Sports activity (yes/no) was considered as potential knee straining if it was one of the following: football, handball, badminton, tennis, volleyball, ice hockey, weight lifting and skiing. Earlier knee traumas (rupture of ligaments, meniscal tears operations, fractures including the knee joint) were categorised into two groups (yes/no).
Graphics splines are curves with simplicity of construction and a capacity to approximate complex shapes through curve fitting and interactive curve design. The restricted cubic splines provide a general and robust approach for adapting linear methods to model non-linear relationships between a response variable and one or more continuous covariates. The dose–response relationship between years in the trade and risk of TF OA was graphically examined by using the restricted cubic spline with four knots.8 9
Correlation between TF and PF OA, bursitis and meniscal tears was evaluated by using κ statistics.
The software package EpiData was used to code data, and statistical analysis was conducted with SPSS statistics, V.17.0.
Results
Characteristics of the study sample are given in table 1. Participants were all men and aged 42–70 years at the time of the examination (mean age 55.6, SD 6.8 years). There was a marked difference in the age distribution and the duration of employment between the two study groups. Graphic designers were generally older and had a higher seniority than floor layers. Regarding height, weight and BMI, the two groups were comparable.
Characteristics of the study sample
Knee osteoarthritis
The prevalence of TF OA was increased (but not significant) in floor layers compared with graphic designers; OR 2.46, 95% CI 0.83 to 7.28 adjusted for BMI, sports activities, age and earlier knee traumas as shown in table 2. On the contrary, PF OA was more frequent in graphic designers compared with floor layers, OR 0.44, 95% CI 0.14 to 1.37.
Risk of radiographic tibio- and patellofemoral knee osteoarthritis (OA) and magnetic resonance imaging-detected meniscal tears and bursitis
A dose–response relationship measured by years in the trade (seniority) was shown for TF OA in floor layers with ORs increasing from OR 0.70 (ns) (≤20 years of exposure); OR 1.89 (ns) (21–30 years of exposure) to OR 4.82, 95% CI 1.38 to 17.0 (>30 years of exposure) when compared with graphic designers without exposure to kneeling work demands (table 3). There was no dose–response relationship for PF OA.
Risk of radiographic tibio- and patellofemoral knee osteoarthritis (OA), and magnetic resonance imaging-detected meniscal tears and bursitis by years in the trade
To further examine the dose–response relationship between years in the trade and TF OA, we included years as floor layer as a continuous variable. The results showed a positive association between years in the floor layer and TF OA (table 4).
Association between years as a floor layer and development of TF OA, PF OA, meniscal tears and bursitis
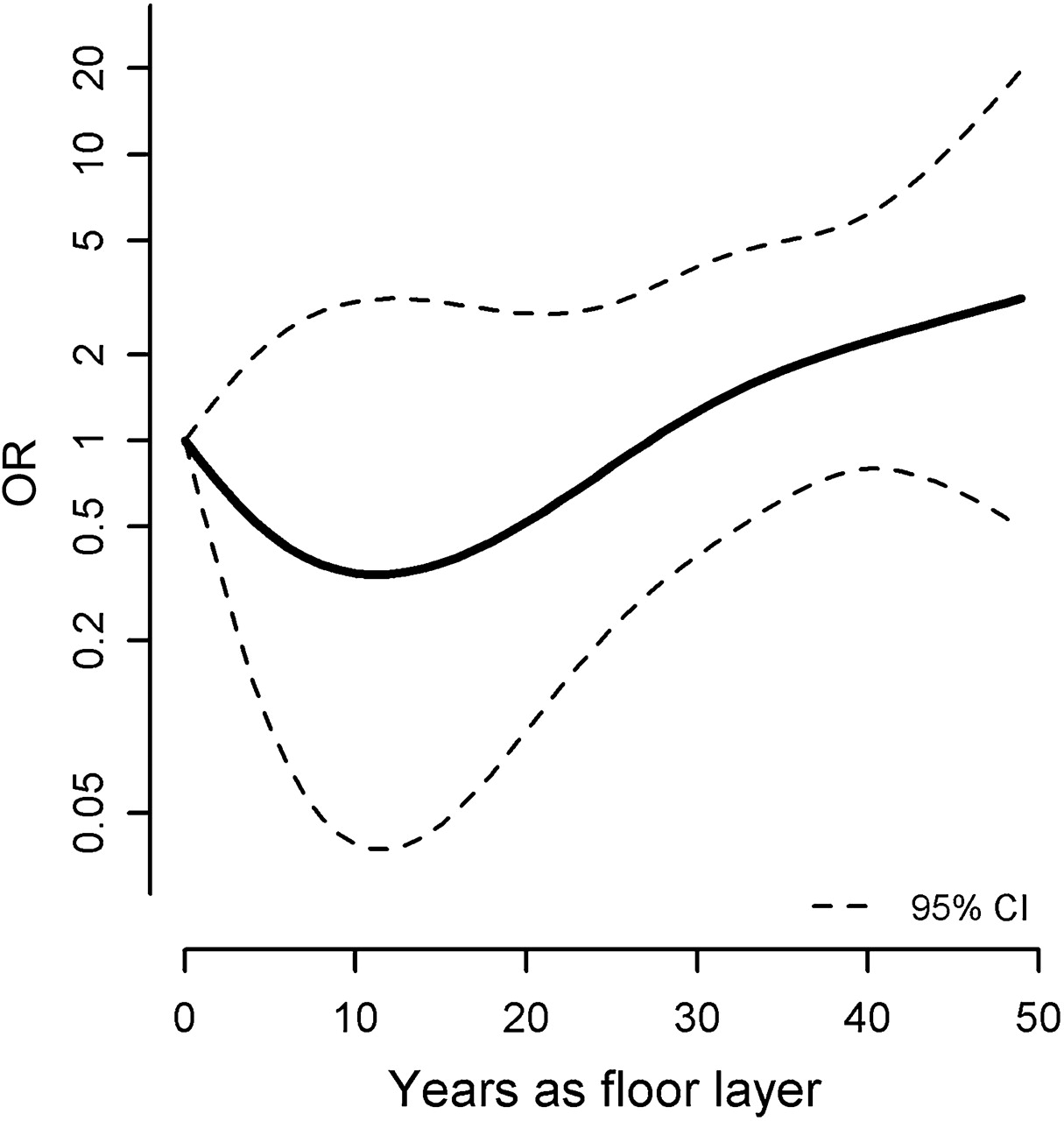
The same pattern was seen when including years of trade as a restricted cubic spline in an age-adjusted logistic regression model (figure 1).
{kind=link}
The dose–response relationship between years in the trade and risk of tibiofemoral osteoarthritis, TF OA, graphically examined by a restricted cubic spline with four knots.8
Meniscal tears
A significant higher prevalence of medial meniscal tears occurred among floor layers compared with graphic designers, as shown in table 2. The risk of meniscal tears did not increase with duration of employment in floor layers compared with the graphic designers (table 3). The adjusted ORs for meniscal tears were 4.73, 4.59 and 1.96 for duration of employment ≤20 years, 21–30 years and >30 years, respectively. There was no significant difference in the prevalence of lateral meniscal tears between the two study groups, and no dose–response relationship between seniority as a floor layers. Additionally, no correlation was found between medial meniscal tears and TF OA in floor layers (κ 0.04). Table 4 shows a significant association between years as a floor layer and the medial meniscal tears but not for lateral meniscal tears.
Bursitis
Nine graphic designers 9/49 (18%) were classified as having prepatellar, superficial or deep infrapatellar bursitis compared with 15/92 (16%) floor layers. The prevalence of prepatellar bursitis was higher in graphic designers (10.2%) compared with floor layers (1.1%). The prevalence of deep infrapatellar bursitis was on the contrary higher in floor layers (10.9%) compared with graphic designers (4.1%), OR 3.53, 95% CI 0.64 to 19.6. A higher prevalence of bursitis in the subgastrocnemius, semimembranosus–gastrocnemius and other bursae (extracapsular synovial cysts, anserine, biceps, LCL and MCL, iliotibial) was observed in floor layers with OR 2.04, 95% CI 0.89 to 4.69.
The ORs for deep infrapatellar bursitis were OR 3.20, 95% CI 0.31 to 32.9 for seniority ≤20 years; OR 7.30, 95% CI 0.62 to 85.7 for seniority 21–30 years and OR 2.30, 95% CI 0.31 to 17.7 for seniority >30 years when compared with the whole group of graphic designers without knee straining work activities.
Fluid collections in other bursae (eg, subgastrocnemius, semimembranosus–gastrocnemius) were increased significantly only for floor layers with ≤20 years of seniority (OR 12.2, 95% CI 1.31 to 113) (table 3).
Table 4 shows a significant association between years as a floor layer and periarticular bursitis.
No correlation between TF OA, deep infrapatellar bursitis and other bursitis was shown (κ 0.08 and 0.12, respectively).
Discussion
The results showed a significant association between years as a floor layer and development of TF OA, medial meniscal tears and periarticular bursitis compared with referents.
The OR for TF OA increased with the duration of employment in the trade. There were only significant differences between the non-exposed reference group and floor layers with more than 30 years of exposure, but there was a tendency towards a dose–response relationship shown by ORs >1 for the medium and high exposure groups when compared with the reference group. These results indicate a dose–response relationship. The small number of workers who were investigated (n=141), and especially few referents among those with low seniority, may influence results and explain the missing significance between all the exposure groups. Only few previous studies have investigated the dose–response relationship between knee OA and the quantity of kneeling work activities. Enderlein and Kasch found a higher frequency of knee OA in participants with a higher extent of hyperkeratosis in front of the patella (used as a measure for the extent of kneeling working position).10 Sandmark et al11 showed OR 2.1 and 1.4, respectively, among workers with high and medium exposure to kneeling work demands compared with low or no exposure. In a study, which included some of the floor layers from the same cohort as in this paper, but 10 years earlier, the ORs for the association between knee OA and exposure to kneeling work activities were 2.9 (low/moderate exposure), 4.2 (high exposure) and 4.9 (very high exposure).1 In summary, indication of a dose–response relationship for osteoarthritis in this study is supported by findings in the previous studies.
The risk of medial meniscal tears was increased in floor layers compared with graphic designers, but there were no difference depending on duration of employment. If meniscal tears are caused by many years of kneeling work, a dose–response effect due to accumulated exposures to kneeling work tasks may be expected. However, if meniscal tears are caused by trauma because of inappropriate posture when getting from kneeling work positions to the standing position many times a day, meniscal tears may not necessarily depend on the duration of the kneeling work.
In this study, the average period of employment was 29.6 years for floor layers. Twenty-two per cent have been employed <20 years, but few of them have been employed <15 years. It is possible that damage to the meniscus occurs before. In conclusion, we did not found a dose–response effect between years of kneeling work and development of meniscal tears. However, the prevalence of medial meniscal tears was significantly increased in floor layers compared with the graphic designers. In general, only few studies have examined the relationship between meniscal tears and occupational kneeling. In a nested case–control investigation by Baker et al,12 the occupational activities of 67 men (4.8%) reporting meniscectomy were compared with 335 controls. After adjustment for sports participation, meniscectomy was associated with kneeling (OR 2.5, 95% CI 1.3 to 4.8) and squatting (OR 2.5, 95% CI 1.2 to 4.9) more than 1 h in an average working day. In a case–control study, Baker et al13 investigated 243 men aged 20–59 years who had a meniscal tear confirmed by arthroscopy and compared them to community controls matched by age and sex. Results showed a significant association between kneeling (OR 2.2, 95% CI 1.3 to 3.6) and squatting (OR 1.8, 95% CI 1.1 to 3.0) >1 h/day and meniscal tears. Greinemann et al14 conducted a case–control study in 500 miners compared with 500 controls without knee demanding work postures, all men in the age of 50 years. In total, 57 miners (11.4%) had a knee surgery for meniscal tears compared with 14 (2.8%) among controls (OR 4.5, 95% CI 2.5 to 7.8). Sharrard and Liddell15 investigated the frequency of meniscectomies among miners and other patients and compared it with the frequency of appendectomies in the same period. Meniscectomy had been performed in 605 miners and 352 men from other occupations. Comparing the frequency of meniscectomy to appendectomy, they found an increased incidence of meniscectomy among miners (OR 3.3, 95% CI 2.7 to 4.0). These results may indicate a possible association between occupational kneeling and development of meniscal tears.
Results in this study showed a higher prevalence of bursitis, in total, among floor layers compared with the reference group. A low prevalence of prepatellar and superficial infrapatellar bursitis in floor layers compared with the reference group was found, and there was even a tendency of a higher prevalence among graphic designers. This finding do not correspond to earlier results of Myllimäki et al,16 who in an ultrasound study found fluid accumulation in the superficial infrapatellar bursa among 5.3% floor layers compared with none in a reference group of painters. Results also showed a low prevalence of prepatellar bursitis among floor layers compared with the reference group. Only one floor layer and five from the reference group had fluid accumulation in the prepatellar bursae. Hill et al17 have showed that prepatellar and superficial infrapatellar bursitis are common among individuals with radiographic knee OA and described fluid in bursae as a physiological phenomenon, which is consistent with findings in other studies.18
We found a higher prevalence of bursitis in the deep infrapatellar, subgastrocnemius, semimembranosus–gastrocnemius bursae and other bursae (as anserine) in floor layers compared with graphic designers. Hill et al found a 4% prevalence of bursitis in other bursae as semimembranosus, anserine and iliotibial in subjects with knee OA compared with none in subjects without knee OA. It suggests that bursitis can occur among subjects with radiographic knee OA, but the association between knee OA and bursitis was not shown in this study where κ testing showed no correlations. A difference between the study group and the reference group in the prevalence of bursitis also does not support the assumption. Identification of bursitis in many bursae, including the posterior part of the knee joint, indicates that bursitis may not only be caused by direct pressure on the knee when kneeling.
We do not know if there is a causal association between external knee pressure and development of knee disorders. However, it seems plausible that a combination of extreme flexion in the knee joint, micro traumas caused by frequent kneeling and a high external knee pressure may cause knee disorders such as knee OA and medial meniscal tears, while some of the knee disorders including bursitis may be explained by external pressure or other intra-articular factors.
The strength of this study is that the floor layers have worked many years in the occupation and have had a substantial amount of kneeling work and that the study included radiographic, MRI and self-reported data.
One of the limitations of the study is the low participation rate that may lead to a risk of underestimation of a real risk. Participants in the radiological and MRI study represented a smaller proportion of those who answered the questionnaire, and there was a predominance of graphic designers with self-reported knee complaints and knee traumas in the study compared with the questionnaire participants of graphic designers (15% compared with 38%). However, such a selection bias would typically also result in an underestimation of a real risk.
Graphic designers are in the study in general older than floor layers. This may have an impact on the number with knee OA, as particularly increases with age. We therefore adjusted for age in the analysis.
In the analysis concerning years of employment in the trade, the graphic designers were defined as having been employed zero years within the floor laying trade. The distribution of the number of years in employment of graphic designers is therefore irrelevant in this context.
Results from the current study may also have been diluted by a healthy worker selection. In the study that consisted of a historical cohort of workers, it was, however, possible to include workers who had expired. The impact of a secondary healthy worker selection may thereby be minimised, although not eliminated. Yet, the effect of a primary healthy worker selection cannot be ruled out, for example, selection of people with good health status into the workforce at the time of hire.
Overall, it is considered that the limitations of the study mainly go against an underestimation of the real risk.
In conclusion, the results of this study indicate a positive dose–response relationship between duration of employment as a floor layer and the development of TF OA and possibly deep infrapatellar bursitis. The risk of developing bursitis in other locations around the knee joint was especially increased for floor layers with seniority ≤20 years. A dose–response relationship for meniscal tears and PT OA was not found, and there were no correlations between meniscal tears, bursitis and TF OA.
Acknowledgments
The authors wish to thank Professor MD Niels Egund from the department of radiology at Aarhus University Hospital for his invaluable effort during the radiological assessments in the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online material
Footnotes
To cite: Jensen LK, Rytter S, Marott JL, et al. Relationship between years in the trade and the development of radiographic knee osteoarthritis and MRI-detected meniscal tears and bursitis in floor layers. A cross-sectional study of a historical cohort. BMJ Open 2012;2:e001109. doi:10.1136/bmjopen-2012-001109
Contributors LK, corresponding author, has the primary responsibility for design, analysis and preparation of the manuscript. SR and JPB have been deeply involved in the study design. SR has collected data under the supervision of LK and JPB. All authors have received the original data and have been deeply involved in the analysis of data, discussion of the manuscript, drafting and revising it critically. Each author has read and approved the final manuscript writing.
Funding This work was supported by the Danish Working Environment Research Fund, the Danish Rheumatism Association, the County of Viborg, the Danish Medical Research Council, M.A. Holms Memory Grants and the Society for the Preservation of Skive Hospital.
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by Central Danish Region Committee on biomedical Research Ethics.
Provenance and peer review Not commissioned; externally peer reviewed.