Article Text

Abstract
Objective To investigate the effect of the H1N1 influenza pandemic on the public's expectations for a general practice consultation and antibiotic for acute respiratory illness.
Design Mixed methods.
Participants Qualitative interviews: 17 participants with acute respiratory tract infection (RTI) visiting English pharmacies. Face-to-face survey: about 1700 adults aged 15 years and older were recruited from households in England in January 2008, 2009 and 2011.
Results The qualitative data indicated that the general public had either forgotten about the ‘swine flu’ (H1N1 influenza) pandemic or it did not concern them as it had not affected them directly or affected their management of their current RTI illness. Between 2009 and 2011, we found that there was little or no change in people's expectations for antibiotics for runny nose, colds, sore throat or cough, but people's expectations for antibiotics for flu increased (26%–32%, p=0.004). Of the 1000 respondents in 2011 with an RTI in the previous 6 months, 13% reported that they took care of themselves without contacting their general practitioners and would not have done so before the pandemic, 9% reported that they had contacted their doctor's surgery and would not have done so before the pandemic and 0.6% stated that they had asked for antibiotics and would not have done so before the pandemic. In 2011, of 123 respondents with a young child (0–4 years) having an RTI in the previous 6 months, 7.4% requested antibiotics and would not have done so before the pandemic. Unprompted, 20% of respondents thought Tamiflu© (oseltamivir) was a vaccine.
Conclusions Expectations of the general public for a consultation or antibiotics with an RTI are similar now to before the H1N1 influenza pandemic; therefore, public antibiotic campaign messages and general practice advice to patients can remain unchanged. Parents with young children and those with personal experience of the H1N1 influenza are more likely to consult and will need more reassurance. The public need more education about Tamiflu©.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
Hypothesis
The H1N1 (2009) pandemic has ‘medicalised’ acute respiratory illness presenting with flu-like symptoms, including cough, cold, sore throat and fever.
The general public may now have a greater expectation that they should seek a consultation with a health professional and have a greater expectation for antibiotics when they next have an acute respiratory illness presenting with flu-like symptoms, including cough, cold, sore throat and fever.
Aims
To determine if expectations for a consultation or an anti-infective have changed as a result of the publics' experiences of the recent (2009) H1N1 influenza pandemic and to explore the publics' understanding of anti-infectives.
Key messages
The H1N1 influenza pandemic has not changed the general public's expectations for a general practitioner's consultation or antibiotics when they have a runny nose, cough, cold or sore throat but may have increased people's expectations for antibiotics for influenza.
Most have either forgotten about the influenza outbreak or it did not concern them as it had not affected them directly.
The smaller subsets of the public with young children and those who have had suspected or confirmed H1N1 influenza themselves are now more likely to consult and request an antibiotic for an RTI and, therefore, these groups will need more guidance and reassurance.
A fifth of the public believe that Tamiflu© (oseltamivir) is a vaccine, implying that enhanced information sharing is needed in this area.
Strengths and limitations of this study
This was a large survey of the general population, repeating some of the questions asked before the 2009 H1N1 flu epidemic, using the same sampling methods.
The qualitative interviews had recruitment problems with many potential interviewees not being at home when telephoned. However, the purpose of qualitative interviews was mainly to enrich our data, and they did help explain our quantitative findings.
The questionnaire survey asked to recall their most recent RTI in the previous 6 months and what actions they took on that occasion. This will be subject to some recall bias.
Introduction
Antibiotic resistance is an increasing problem in the community that has been highlighted by the WHO, European Health Council and, most recently, a EU-US Transatlantic Task Force.1–3 An individual's previous use of antibiotics is associated with a twofold increase in the risk of a subsequent respiratory tract infection (RTI) or urinary tract infection (UTI), within 12 months, being caused by an antibiotic-resistant organism.4 England, as well as other European countries,5 has implemented public health campaigns, based mostly on general practices and pharmacies, to encourage the public to ask for and to expect antibiotic prescriptions less often. The key message of recent English campaigns has been: ‘The best way to treat most colds, coughs or sore throats is plenty of fluids and rest. For advice talk to your pharmacist or doctor’.6 A further Department of Health (DH)-funded antibiotic campaign was planned for autumn 2009.7 However, in spring 2009, cases of H1N1 influenza A in England began to rise and, to avoid any public confusion with messages about what they should do when they had an RTI, the antibiotic campaign in the autumn of 2009 and spring of 2010 did not proceed. Flu response centres were set-up with the aim of delaying onward transmission of the virus. Initially, all suspected cases of influenza and their contacts were tested for the virus and given antiviral treatment or prophylaxis with Tamiflu© (oseltamivir). By July 2009, the H1N1 influenza virus had become widespread in the community, and the primary aim became the clinical management of cases through a dedicated National Pandemic Flu Service (NPFS) website and telephone service (flu line).8 This was for people with flu-like symptoms (including high fever, aching muscles, headache, sore throat, cough and runny nose); symptoms which have a high sensitivity but low specificity for influenza. Those with suggestive symptoms were given a unique ‘flu number’ to obtain a course of Tamiflu© treatment. Of patients with flu symptoms authorised to receive Tamiflu© by NPFS, selected to be sent a swab kit and returning a specimen, 7% were positive for influenza A H1N1.9
Two waves of pandemic activity were observed, separated by the closure of schools for summer holidays.10 Community transmission was initially observed in London and the West Midlands following large school outbreaks. Cases were reported from all UK regions in the summer wave, though there was a variable level of transmission; all regions of the UK were affected in a more uniform way during the autumn wave. Most cases were reported to have a mild illness consistent with influenza. Severe disease, hospitalisations and deaths were reported in a minority of cases, particularly among those with underlying clinical disease that had a 10-fold risk of hospitalisation.10 There was an overall low case death ratio of 0.04%, particularly compared with previous pandemics.10 Pandemic H1N1 vaccine was used and was effective, though uptake only increased in the second half of the autumn wave.10
By February 2010, as numbers of influenza in the community had dramatically decreased, the NPFS was closed and care of patients consulting with flu-like or respiratory symptoms returned to the responsibility of general practitioners (GPs) or NHS Direct. From then on, GPs have decided whether to prescribe antibiotics/antivirals based on their clinical judgement and local antimicrobial guidance. In 2010, because of budget restrictions, the DH launched a low-budget antibiotic awareness campaign through the professional societies. It coincided with European Antibiotic Awareness Day and was aimed at promoting prudent antibiotic use in hospitals, while continuing to reinforce the messages to the general public and GPs. GPs received an email highlighting the day with links to materials to download or order.
The advice to the general public during the 2009 H1N1 influenza pandemic ‘to always seek health advice when they had respiratory or flu-like symptoms’, essentially so Tamiflu© could be prescribed, ran counter to National Institute of Clinical Excellence RTI advice, which recommended that GPs should follow a ‘no’ or a ‘delayed’ antibiotic prescribing strategy for patients with acute self-limiting RTI11 and may have ‘medicalised’ acute respiratory illness. As a consequence, the general public may now have lowered their threshold for consulting and increased their expectations for antimicrobial treatment for RTI or flu-like symptoms. We, therefore, aimed to determine whether the general public's expectations for a consultation or an antibiotic changed as a result of their experiences of the 2009 H1N1 influenza pandemic and to explore their understanding of Tamiflu© treatment. We considered that the findings could not only inform the key messages to the general public during future antibiotic awareness campaigns but also inform key messages for the general public during the next rise in seasonal or H1N1 influenza.
Methods
First, we used in-depth telephone interviews with patients, enrolled when visiting pharmacies, to explore their views on their own management of recent respiratory illness. Second, the results of this qualitative research informed questions in an Ipsos MORI12 survey in England in January 2011. Some of the questions regarding beliefs about and use of antibiotics were asked in related 2008 and 2009 Ipsos MORI surveys13 before the H1N1 influenza pandemic, and so it was possible to compare the results of the three surveys, two before and one after the pandemic.
Study population for qualitative interviews
To obtain a sample of adult participants with diverse ethnicity and deprivation in urban, city and rural settings, including some patients with personal experience of H1N1 influenza, we recruited members of the public in nine pharmacies based in four different areas of England, all with a high level of Tamiflu© dispensing and with above average or normal H1N1 influenza activity during the pandemic. As the interviews were conducted during the recruitment period, the pharmacies were visited several times, in rotation, until data saturation was reached. In total, the pharmacies were visited 26 times for 3–6 h at a time. In 2010, 65% of the general public reported visiting a pharmacy in the past year.13 Recruiting participants in pharmacies allowed us to obtain data from members of the public with current symptoms of cough, cold, sore throat or flu who had either recently consulted a doctor (and may be picking up a prescription for antibiotics); those who were managing the condition themselves (buying over the counter remedies) and others who were in the pharmacy for reasons unrelated to acute respiratory tract illness.
Flu activity for the weeks 29–52 in 2009 was determined using a combination of QSurveillance data14 (which is biased towards identifying high flu activity early in the pandemic) and cumulative pharmacy Tamiflu© dispensing data, obtained from a single pharmacy company that has outlets across the UK (which is biased towards identifying high flu activity later in the pandemic). QSurveillance provides rates of GP consultations for influenza-like illness (ILI) in Primary Care Trusts and is divided into four thresholds of activity of H1N1; that is baseline 0–20 per 100 000 practice population; normal seasonal 21–70; above average 71–130; exceptional activity 131+. We selected nine pharmacies, all with high Tamiflu© dispensing. Four urban pharmacies were randomly selected from high Tamiflu© dispensing pharmacies in South Birmingham (The Midlands, England), and three were randomly selected from such urban pharmacies in Enfield (North London; both areas with above average QSurveillance ILI activity). We also randomly selected one rural pharmacy with high Tamiflu© dispensing in West Hertfordshire (South East England) and one such rural pharmacy in Oxfordshire (Central England); both areas had normal QSurveillance ILI activity.
Two researchers separately visited the pharmacies several times between October and December 2010. Pharmacies displayed a poster provided by the research team that introduced the research. Members of the public in the pharmacy were opportunistically approached to complete a short pro forma that asked if they, or someone they were caring for, was currently unwell with symptoms of cough, cold, sore throat or flu-like illness that had started within the preceding 3 weeks. If they answered ‘no’, they were not eligible to take part; but they were offered information about managing coughs, colds and flu. From the pro forma, one in three persons was found to be eligible at each pharmacy on each day of recruitment. If they answered ‘yes’, the pro forma went on to ask if they would be prepared to be interviewed and, if so, to provide a telephone number and time that the researcher could contact them to undertake a telephone interview. The pro forma also asked about age, sex, ethnicity, children younger than 5 years, sources of advice during their current illness and whether they had taken Tamiflu© or collected Tamiflu© for someone in the past year. Potential participants were telephoned by one researcher to arrange a telephone interview and to discuss the study. Participants gave verbal informed consent before the telephone interview, which we aimed to complete a maximum of 14 days after the pharmacy visit, and retrospective written consent. Participants received a £10 Lloyds Pharmacy voucher as a thank you for their time. The interviews were undertaken just before the 2010 rise in ILI consultations in general practice (figure 1).
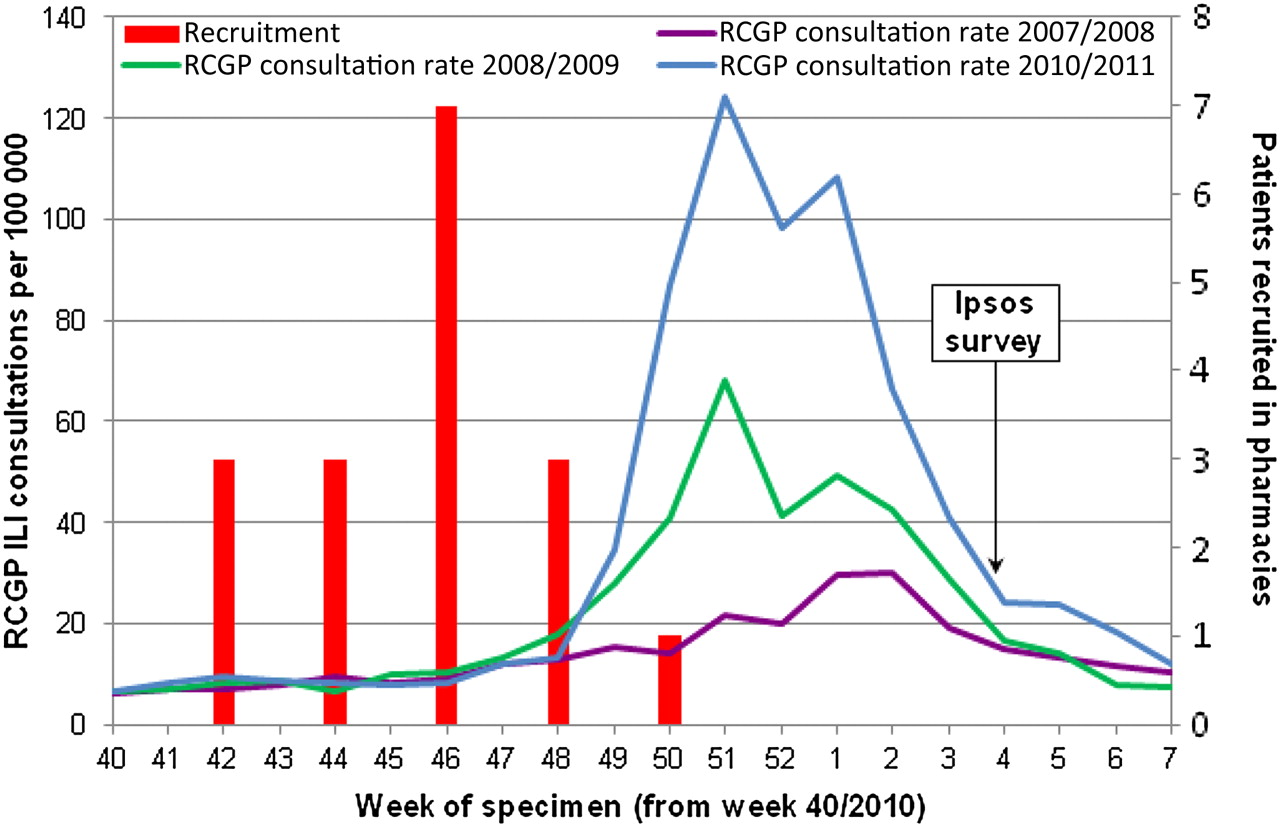
Number of patients recruited to the qualitative work and timing of Ipsos survey relative to the number of general practitioner's patient consultations for influenza-like illness (ILI) per 100 000 population in England and Wales. Consultation rates compiled by the Royal College of General Practitioners (RCGP), Research and Surveillance Centre and supplied by the Health Protection Agency.
Sampled participants for Ipsos MORI questionnaire survey
Multistage sampling was used to recruit a target of 1800 adults aged 15 years and older in England in January 2011. A market research company, Ipsos MORI,12 conducted the interviews as part of their weekly ‘Capibus’ survey that collects a wide range of information from across the country in a single week. Approximately 180 Local Area Authorities are randomly selected in the first stage of sampling. Some of these are in Wales and Scotland and do not feature in this study. In the second stage of sampling, one Output Area (OA) is randomly selected from each Local Area Authorities. An OA is a small area made up of between 60 and 100 addresses. Interviewers are given quotas of people to interview for each OA according to age and gender. Interviewers go door-to-door and invite the person who answers (as long as they are 15 years and older) if they would be willing to take part in the survey. If that person refuses, interviewers can invite another member of the household to participate. Visits are spread out over the week so households are visited in the daytime, evenings and both Saturdays and Sundays to ensure inclusion of people who work weekdays. If there is no response from the household, then interviewers do not revisit. Interviewers generally get about one complete interview for every three or four doors on which they knock.
Ethics
The Ipsos MORI surveys and interviews were undertaken outside the NHS setting and therefore did not need NHS ethical approval. The study was approved by the ethics review board at Coventry University. Consent for the Ipsos MORI questionnaires was by verbal agreement to participate with completion of the questionnaire considered as indicating consent; respondents were not given any financial incentive. Respondents were able to refuse to participate in the interview or questionnaire at any stage in the process. All data were processed in accordance with the Data Protection Act 1998.
Schedule for qualitative interviews
The semistructured interview schedule was developed collaboratively by the authors, a member of the public on the steering group and with input from the DH communications team and the paediatric representative of the DH Education Subgroup on Antimicrobial Resistance and Healthcare Associated Infections (ARHAI) (online appendix 1).
The schedule was based on Leventhal's Common Sense Model15 and previous research exploring beliefs about antibiotic use, influenza and consultation behaviour in primary care. The Common Sense Model proposes that, when faced with a threat to their health, the coping strategies adopted by the individual depends on their ‘common sense’ beliefs about that threat and possible coping strategies and, in particular, whether possible coping strategies make sense in terms of their beliefs about the threat.15 The interviews therefore aimed to elicit beliefs about the health threat (ie, respiratory or flu-like symptoms) and the possible behavioural responses such as seeking a prescription for antibiotics or self-management. The schedule was piloted with five members of the public to explore ease of comprehension. Topics explored included the current illness episode, and what healthcare advice they had sought, if any, and why and about their perceptions of the sorts of medications that might help cough, cold, sore throat or other flu-like symptoms. When participants had explained their current illness decisions fully, they were then asked whether the swine flu outbreak the previous year had affected the decisions they had made about their current illness, how the swine flu outbreak was handled by the DH and whether the public campaign message ‘Antibiotics don't help when you have coughs or colds’ should still be used following the recent swine flu outbreak. The terms ‘Swine flu’ and ‘swine flu outbreak’ were used in the interviews and questionnaire as H1N1 influenza was not common parlance in the winter of 2010/2011.
Qualitative data collection and analysis
The interviewer (PJ) encouraged respondents to speak candidly about the management of their recent RTI illness. All interviews were recorded and transcribed verbatim. Data were subjected to thematic analysis. Transcripts were coded into themes by one member of the research team (PJ). Themes were discussed and agreed upon by the steering group, including three members of the research team who read a sample of the transcripts (LA, DF and KN).
An iterative process was used (where interviews and analyses occur in parallel) allowing additional exploration of new themes as the process progressed. We considered after 17 interviews (including five people with experience of H1N1 influenza) had been conducted that no novel material was being elicited.
Questionnaire for Ipsos MORI survey
Some questions about expectations for antibiotics for runny nose, cough, cold, sore throat and flu, use of and knowledge of antibiotic activity in the Ipsos MORI surveys in 2008 and 2009 were left unchanged so that responses could be compared before and after the H1N1 influenza pandemic.13 Other questions were new to the 2011 survey; some of these were based on the qualitative interview findings, including some hypothetical questions about whether respondents thought their behaviour in relation to a recent RTI would have been different before the H1N1 influenza pandemic. To reduce acquiescence bias, general questions were asked first followed by questions about their recent RTI, which were asked in a separate part of the same Ipsos MORI survey; the questions about understanding of Tamiflu© (oseltamivir) were asked in a separate survey the following week. The 2011 survey was carried out just after the fall in ILI in January 2011 determined by QSurveillance data14 (figure 1; online appendix 2).
Questionnaire data analysis
Weights provided by Ipsos MORI and based on the National Readership Survey were used to correct for known selection biases. Weights are defined by gender and, within gender, by age, social grade, region and working status. Initial data processing was carried out by Ipsos MORI, with further data management, and all analyses performed by TN using Stata V.11.2 (Stata Corporation). All results make use of the weights and allow for the clustering of the sample. Significance tests for differences in percentages were a variation of the Pearson χ2 test.
Results
Interview results
Fifty eligible persons agreed to a telephone interview when asked at the pharmacy. Of these, three participants had given wrong numbers, two declined to participate when contacted, 10 never answered the phone (private number or number showing), nine did not answer the telephone at the time when an interview had been arranged and nine could not commit to a time for an interview despite several phone calls. In total, 17 people were interviewed between 3 and 8 days of the pharmacy visit (median 6 days). Eight had only consulted their pharmacy with their current RTI, while three had consulted their GP only; five went to both, consulting their pharmacy first and subsequently their GP, and one made several visits to both pharmacy and GP. Ten were women; 16 were white and one was South Asian; five either had confirmed or suspected H1N1 influenza themselves or lived with another member of their household who had confirmed or suspected H1N1 influenza.
None of the participants reported that the swine flu had affected their management of the current illness. Participants reported that they had either forgotten about the influenza outbreak or, as it had not affected them directly, it did not concern them (box 1). Several commented that, as the swine flu outbreak had not been as serious as the government had expected, they did not need to worry. Some described the DH as initially panicky or overcautious, but most participants thought the government had handled the outbreak and media coverage well. Most reported that they had heard of Tamiflu© either in the news or on TV, and a few had experience of friends or family taking it. Several thought that it was a vaccination and, initially, one participant thought that it was a strain of flu. When asked about the sort of medications that would help with fever, cough, cold, sore throat or flu-like symptoms and about the benefits of antibiotics, some participants struggled to answer, not knowing whether antibiotics would work or not. When participants were asked if the campaign message ‘antibiotics don't help when you have coughs and colds’ should continue to be used in public antibiotic campaigns, the majority of participants thought that the message should continue to be used, as they agreed with the message and it was appropriate unless you had severe symptoms or pain. Four participants were not sure whether it should be used, and two participants thought that the message should not be used; one because it was up to the doctor to decide if you needed antibiotics and another thought antibiotics did help when you had a cough or cold.
Quotes from interviews with members of the public visiting pharmacies with acute respiratory tract infection (RTI) in October–December 2010
Participants' behaviour in current RTI unaffected by the swine flu (H1N1 influenza)
P33: I‘ve sort of forgotten all about it now really, none of it has really stuck.
P26: I know a few people that potentially have had swine flu, but no it's never really phased me to be honest.
P10: I know, at the time, I felt very aware of any cold or flu symptoms. It was something that was very present in my mind, at the time, but, since, it's gone away, and now I’d probably have put it to the back of my mind.
The H1N1 pandemic was not as big as predicted, and therefore, it would not influence what they did.
P39: I thought it was all blown up out of proportion, I think it was just a bit of panic by the government—with anything they always panic and they create a lot more worry to people than is necessary.
P34: No not really because I don't think the swine flu outbreak was as bad as everyone panicked or thought it was going to be, everyone thought that everyone was going to die and everyone was going to be really really ill. I just I don't assume that things are swine flu I think that they're flu or a cold.
Handling of swine flu (H1N1 influenza) by the DH.
P35: I think they must have done a good job. Nothing that bad happened, did it, I don't think.
P8: Well at first it was panicky and it settled down towards the end, like very good for everybody really yeah, they got on top of it, of course if it became to be a big epidemic it would be very dangerous for everybody.
Understanding of Tamiflu© (oseltamivir)
P7: my niece was, had to take some because we thought she had swine flu.
P10: It's the H1N1, um, it's a inoculation, isn't it, for H1N1.
P38: Tamiflu it's just been on the telly there a few minutes ago, there was lots about the swine flu symptoms coming back and the kids want to get them all vaccinated.
Understanding of benefit of antibiotics for different RTIs.
P13: Well, I've heard that antibiotics do help if you've got a cold but they just tell you they don't, for some reason, because maybe they're not very good for you. I've also heard that they're completely useless in a cold. So, I don't really know what to believe, so, I always just go by the guidelines of if I've got an infection, I'll take them and if not, I won't.
Most participants agreed the message that antibiotics do not work on coughs and colds should continue to be used:
P34: Yes, because the swine flu was different, my view is as well if you have got a cough and a cold there is no point in just going to the GP with a cough or a cold because there's nothing they can give you, if it's something more severe like a chest infection then they can give you the antibiotics. But I think that message still stands because swine flu was different, completely different.
P26: Yes I suppose campaigns when you're trying to get a message across to people helps quite a lot ……. I think some people go to the doctors for anything, and I don't think the doctors really give out antibiotics for coughs and colds. So just trying to stop the amount of people that go to the doctors for coughs and colds or…
P22: I think so, yes…and it's not for colds, is it, antibiotics?
Campaign message ‘antibiotics do not work on coughs and colds’ should not be used:
P36: No not really no. No I don't because I find, I believe, that antibiotics do help especially when you've got one (a cough) like I have this week. Coz you know as I said I know I don't get the pain in my chest—therefore they're working.
P33: No, no, I don't think it should be (nor) use the message. Because I think when you go to the doctors and you go with the symptoms I think it's probably up to the doctor to decide whether or not they prescribe antibiotics.
Ipsos survey results
All respondents
There were a similar number of respondents aged 15 years or older interviewed each year in weeks 3, 4 or 5 in England (2008, N=1706; 2009, N=1707; 2011, N=1767). In 2011, there were 209 respondents with children aged 0–4 years (table 1).
Public's expectation for antibiotics before and after H1N1 influenza pandemic: based on comparable questions to adults 15 years and older asked in 2008, 2009 and 2011
Between 2008 and 2011, there was progressive improvement in the percentage of respondents providing a scientifically acceptable answer to the question about activity of antibiotics against coughs and colds (the percentage understanding that antibiotics do not work on most coughs and colds was 60% in 2008, 63% in 2009 and 69% in 2011) (table 1). There was little or no change in people's expectations for antibiotics for runny nose, colds, sore throat or cough between 2008 and 2011, but expectations that their GP or nurse would prescribe them an antibiotic if they had flu increased significantly from 24% in 2008 to 26% in 2009 to 32% in 2011 (the increase between 2009 and 2011 was significant, p=0.004). Between 2008 and 2011, there was little or no change in people asking for antibiotics for any reason either for themselves or for someone else in the past year (28% in 2008, 29% in 2009 and 26% in 2011). The change between 2009 and 2011 was non-significant (p=0.20).
Between 2008 and 2011, there was little or no change in people being prescribed any kind of antibiotic for themselves in the past year in the UK (32% in 2008, 36% in 2009 and 32% in 2011). The change between 2009 and 2011 was borderline significant (p=0.06).
In 2011, 8.9% of respondents reported that they or someone in their household had had suspected or confirmed swine flu (4.3% themselves, 4.7% someone else) and 11% reported that they had been prescribed Tamiflu© in the previous 2 years. People's understanding of Tamiflu© was poor (table 2). Although 71% stated that they had heard of Tamiflu©, without prompting only 34% thought that it helped for influenza or swine flu or was used as an antiviral agent; however, 20% reported that it was a vaccine and 8% a flu-like illness. Prompted by a show card and asked to indicate which of the following statements were true, 33% reported that it was a vaccine and 46% that it helped when you had flu or was used as an antiviral agent (table 2).
Proportion saying the following about Tamiflu© (oseltamivir), unprompted and with a showcard with these statements written on it
Respondents with recent RTI
In the 2011 Ipsos survey, 58% of respondents reported having a sore throat (25%), cold (37%), cough (26%) or flu symptoms (14%) in the previous 6 months; 9% reported that the swine flu outbreak or the media coverage of it had affected their actions a lot when they had their recent illness, 23% that it affected their actions a little and 66% that it had not affected their actions at all. The biggest behaviour change (‘what they did for their most recent RTI and would not have done before the swine flu outbreak’) was washing their hands more often (16%). The other actions that respondents reported were different to what they would have done before the H1N1 pandemic were taking care of themselves without contacting the doctor's surgery (13%) and contacting or visiting their doctor's surgery (9%). Only 0.6% stated that this time they had asked for antibiotics at the doctor's surgery when they would not have done so before the H1N1 pandemic and 1.4% asked for Tamiflu© when they would not have done so before the pandemic.
In contrast, the H1N1 pandemic seems to have made parents of a young child more likely to contact or visit their doctor's surgery when their child has an RTI. Of 123 respondents with a child (0–4 years) who had a sore throat, cold, cough or flu symptoms in the last 6 months, the behaviours that they said occurred as a result of their child's most recent illness and would not have occurred before the H1N1 pandemic included: contacting or visiting their doctor's surgery (14%), taking care of them without contacting the GP (3.4%), asking for antibiotics (7.4%), asking for Tamiflu (5%) and keeping their child at home (6.7%) (table 3).
How actions of respondents with regard to their or their child's sore throat, cold, cough or flu symptoms in the last 6 months were affected by the H1N1 pandemic
Respondents with a recent RTI were more likely to have contacted their GP if they had experienced H1N1 influenza themselves (35% if they previously had suspected or confirmed H1N1 influenza vs 19% if they had not, p=0.004) (figure 2A). Respondents with a recent RTI were also more likely to have contacted their GP if they had been prescribed Tamiflu© themselves (29% if they had previously been prescribed Tamiflu© vs 18% if they had not, p=0.01) (figure 2B).

{kind=link}
{kind=link}
(A) Whether respondent contacted or visited their local practice for their most recent respiratory tract infection (RTI) by personal experience of swine flu. Group sizes are 51 (‘Yes myself’), 53 (‘Yes someone else in the household’) and 873 (‘No’). (B) Whether respondent contacted or visited their local practice for their most recent RTI, by whether prescribed Tamiflu© in the past 2 years. Group sizes are 116 (‘Yes’) and 863 (‘No’). (C) Respondents' expectations for antibiotics for their most recent RTI by their personal experience of swine flu. Group sizes are 51 (‘Yes myself’), 53 (‘Yes someone else in the household’) and 873 (‘No’). Figures show percentage and 95% CI.
Respondents with a recent RTI were also more likely to expect antibiotics from their GP for their recent illness if they had experienced H1N1 influenza themselves (20% if they previously had suspected or confirmed H1N1 influenza themselves vs 10% if they did not, p=0.05) (figure 2C).
Discussion
Principal findings
Our results indicate that the pandemic flu line and the media coverage surrounding the H1N1 influenza pandemic probably had little or no affect on people's expectation for an antibiotic or a consultation with their GP surgery for runny nose, cold, cough and sore throat. In contrast, we found that the public were now significantly more likely to expect antibiotics for flu-like symptoms, and some of this increase is probably due to the pandemic. The small subgroup of respondents who had experienced H1N1 influenza themselves (4.3%) were more likely to consult their surgery with their most recent RTI (35% vs 19%).
Parents managed their young children's RTIs different from their own. Of respondents with a young child (aged 0–4 years) having a recent RTI, 3.4% reported that they took care of their child without contacting the GP surgery when they would not have done so before the H1N1 influenza pandemic, but 14% reported that they consulted the doctor's surgery when they would not have done so before the H1N1 influenza pandemic.
Many of the general public did not know what Tamiflu© was. Only one-third thought that Tamiflu© helped for influenza or was used as an antiviral agent, 29% had not heard of Tamiflu©, 20% thought that it was a vaccine and 8% a flu-like illness.
Strengths and limitations
This was a large survey of the general population, repeating some of the questions asked before the 2009 H1N1 flu epidemic. The surveys used the same sampling methods. Respondents were recruited from throughout England by a leading market research company. The qualitative interview component informed the survey questions, enriched the data and suggested explanations for some of the quantitative findings. Recruitment for the qualitative interviews was based in areas of England with a high level of Tamiflu© dispensing. The qualitative interviews had recruitment problems with many potential interviewees not being at home when telephoned. However, research of this nature relies on consenting participants, raising the possibility of a biased sample. However, the purpose of qualitative interviews was mainly to enrich and explain our larger quantitative findings. The questionnaire survey asked respondents to recall their most recent RTI in the previous 6 months and what actions they took on that occasion. This will be subject to some recall bias. Just over 4% of our respondents reported that they had personally had suspected or confirmed swine flu. Almost 800 000 (CI 375 to 1 644 000) cases of ILI due to H1N1 were estimated to have occurred in England in 2009,16 this equates to 1.5% (CI 0.7% to 3.2%) of the population. Our percentage includes respondents with suspected influenza, and therefore, it is not surprising that it is higher; furthermore, Evans et al do not include patients who did not consult a health professional with ILI and they observed that consultations were much lower in the second phase of the pandemic. They were also asked if the ‘swine flu outbreak’ had affected what they did on that occasion and what actions they took which they would not have done before the outbreak. This is a hypothetical question that may have been difficult to answer. However, the reported lack of change in behaviour to what they would have done before the swine flu outbreak (a question asked only in 2011) is consistent with the lack of change in the public's expectation for antibiotics for respiratory symptoms we found in 2008, 2009 and 2011. The Tamiflu questions were asked in a separate week to reduce response bias, which may have occurred to previous questions in the survey about their experience of flu and use of Tamiflu for it. This prevented any response bias but meant that we were unable to relate the public's knowledge about Tamiflu to any of the other responses.
Comparison with other published work
Teasdale and Yardley17 discussed the government advice for managing the H1N1 influenza pandemic with members of the public in focus groups during the pandemic in late 2009. They found that the participants did not feel that they could distinguish normal cough and cold symptoms from flu-like symptoms. One year later, our interview respondents did not report this as a problem and did not think that their RTI symptoms were due to influenza. In the study by Teasdale and Yardley,17 participants felt underqualified to self-diagnose and self-care at home and reported that they would need to seek advice to determine if they needed treatment. In our questionnaire survey, 12% stayed at home, 13% self-cared for their recent episode of RTI without contacting their GP and 9% reported that they had contacted their doctor's surgery when they would not have done so before the H1N1 influenza pandemic. The greater ability of our participants to distinguish normal cough and cold symptoms from flu-like symptoms compared with those in the study by Teasdale and Yardley, probably reflect that Teasdale and Yardley enrolled participants at the height of the pandemic when there was still considerable uncertainty about the likely severity of the pandemic.17 Our interview participants reported that they felt the pandemic had not been as severe as was initially anticipated.
We found that adults with a child reported a much higher level of GP consulting with regard to their child's most recent RTI than did all respondents with regard to their most recent RTI. Butler et al18 found that parents were much more likely to report accepting self-management advice for themselves because they ‘know how they are feeling’ but were less able to assess illness severity in their children.
Interviews with parents of children admitted to hospital with complicated RTI revealed missed opportunities for early treatment that resulted from several parental factors, including parents' inability to assess illness severity and belief that they would not receive antibiotics if they did consult.19 Parental beliefs, fears and expectations play an important part in both consulting behaviour and expectations for antibiotics. Prescribing data shows that primary care antibacterial prescribing for children in the UK rose by 4% per year between 2000 and 2007.20 Our findings suggest that we do need to address these expectations and fears through effective information sharing with parents. Clinicians discussing an interactive booklet with parents on RTIs in children within primary care consultations reduced intention to consult and reduced antibiotic prescribing, without reducing satisfaction with care.21
Interpretation of the results
The lack of change in the public's consultation behaviour may be explained by our qualitative findings that people thought that the H1N1 influenza pandemic was not as serious as expected or, as it had not affected them directly, it did not concern them and they did not perceive a connection between their usual coughs, colds and sore throat and the H1N1 pandemic influenza. Rubin et al found that about 80% of a random sample of members of the public across the UK telephoned during the pandemic were satisfied with the amount of information available from the government about the influenza pandemic and that people's worries about catching H1N1 pandemic influenza decreased during the winter of 2010.22 We found that those who had suspected or confirmed H1N1 influenza themselves were more likely than others to contact their GP surgery. Our findings support the Leventhal model of health-related behaviour,15 which suggests that personal experience is associated with a higher perceived risk, which in turn is associated with help-seeking behaviour (eg, consulting their GP surgery when they have an RTI). Moore et al23 found that patients who had been prescribed an antibiotic for cough in the previous 2 years were over twice as likely to consult for a similar illness and that a delayed antibiotic prescription strategy reduced re-consultation by 78% in this group. Previous attendance with cough and other RTI also predicted re-consultation, so consulting behaviour as well as personal experience of illness influence help-seeking behaviour.
The two largest changes in reported behaviour with their most recent RTI, which they said they would not have done before the pandemic flu, were washing their hands more often and staying at home. This is consistent with the advice of the influenza pandemic media campaign. A survey in a service station lavatory in England also showed that the media had an impact on hand-washing with rates increasing during the time in which H1N1 influenza featured prominently in blogs and in the news.24
The increased expectation for antibiotics to treat flu-like symptoms may be explained by the lack of understanding of the difference between antiviral agents (active against viral infections) and antibiotics (active against bacterial infections). Only 46% of respondents in our 2011 survey correctly identified Tamiflu© as treatment for influenza or an antiviral, although, encouragingly, only 7% thought that it was an antibiotic. A third thought Tamiflu© was a vaccine; such misunderstandings may be relevant to poor uptake of H1N1 vaccine. In the event of another influenza outbreak (which may be of a different strain but will inevitably be called swine flu again by the media and public), a targeted public health campaign might be needed to correct the view that taking Tamiflu© is protective against future influenza.
Implications for policy makers
This year's European Antibiotic Awareness Day public campaign messages in England do not need to be changed as a result of the H1N1 influenza pandemic. Parents need more guidance about which symptoms should trigger a consultation for their young children and a plan made about rapid reassessment should they feel it necessary. Patient leaflets for use during a discussion during the consultation need to be readily accessible; short cuts to suitable materials are available on the DH website.25 The lack of understanding that Tamiflu© is an antiviral agent specifically for the treatment of acute influenza should be addressed in both vaccination information and during influenza epidemics. These findings should also inform antimicrobial stewardship programmes, such as toolkits for community medicine managers and primary care.26
Implications for clinicians in primary care
Expectations for a consultation or antibiotics when getting an RTI are similar now to what they were before the H1N1 influenza pandemic. Therefore, primary care clinicians' advice to patients does not need to be adapted in the light of the pandemic. Those patients who had suspected or confirmed H1N1 influenza and parents with young children may, however, need more intensive explanation and reassurance. Some patients may confuse previous consumption of Tamiflu© with influenza vaccination and not understand the difference between antiviral and antibiotic agents.
Acknowledgments
We thank Katie Newby, Louise Wallace and Nicholas Russell at Coventry University for their advice and help with the qualitative work; Graham Tanner the patient representative; Andrew Gibb at Lloyds head office and the community pharmacists who allowed patient recruitment; the patients who took part in the interviews; the staff at Ipsos MORI, the public who answered the household questionnaire; Mike Sharland, Sally Wellsteed, Christine Robert and other staff at the DH who gave advice about questionnaire format; and Gillian Smith, Neeta Singh and Alex Elliot from the Real-time Syndromic Surveillance Team who provided us with the QSurveillance data.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data Supplement - Manuscript file of format pdf
Footnotes
The Lloyds pharmacy group commented on interviewee information leaflets and pharmacy poster, provided data on Tamiflu© dispensing and commented on the suitability of selected pharmacies, in terms of layout and staffing, for the study, but otherwise had no influence on the study design or interviewee selection.
To cite: McNulty C, Joshi P, Butler CC, et al. Have the public's expectations for antibiotics for acute uncomplicated respiratory tract infections changed since the H1N1 influenza pandemic? A qualitative interview and quantitative questionnaire study. BMJ Open 2012;2:e000674. doi:10.1136/bmjopen-2011-000674
Contributors CM designed the study. CCB, TN, AH and DF contributed to the refinement of the study. PJ and LA undertook the qualitative interviews and analysis. All authors contributed to the design of the qualitative and quantitative questionnaires. TN undertook the analysis of the quantitative questionnaire. CM wrote the paper. All authors contributed to drafting and have seen and approved the final version of the manuscript.
Funding This study was funded by the Health Protection Agency.
Competing interests CM leads the development and writes evidence-based antibiotic guidance for primary care and also chairs the ARHAI Public Education Subgroup. Any payment for speaking at conferences goes to a research trust fund.
Ethics approval The household survey and interviews were undertaken outside the NHS setting and, therefore, did not need NHS ethical approval.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data can be obtained from the authors on request.