Article Text

Abstract
Objectives Patients with peptic ulceration continue to present to surgeons with complications of bleeding or perforation and to die under surgical care. This study sought to examine whether improved consultant input, timely interventions and perioperative care could reduce mortality from peptic ulcer.
Design Prospective collection of peer-review mortality data using Scottish Audit of Surgical Mortality methodologies (http://www.SASM.org) and analysed using SPSS.
Setting Secondary care; all hospitals in Scotland, UK, admitting surgical patients over 13 years (1994–2006).
Participants 42 736 patients admitted (38 782 operative and 3954 non-operative) with peptic ulcer disease; 1952 patients died (1338 operative and 614 non-operative deaths) with a diagnosis of peptic ulcer.
Primary and secondary outcome measures Adverse events; consultant presence at operation, operations performed within 2 h and high dependency/intensive therapy unit (HDU/ITU) use.
Results Annual mortality fell from 251 in 1994 to 83 in 2006, proportionately greater than the reduction in hospital admissions with peptic ulcer. Adverse events declined over time and were rare for non-operative patients. Consultant surgeon presence at operation rose from 40.0% in 1994 to 73.4% in 2006, operations performed within 2 h of admission from 10.3% in 1994 to 28.1% in 2006 and HDU/ITU use from 52.7% in 1994 to 84.4% in 2006. Consultant involvement (p=0.005) and HDU/ITU care (p=0.026) were significantly associated with a reduction in operative deaths.
Conclusion Patients with complications of peptic ulceration admitted under surgical care should be offered consultant surgeon input, timely surgery and HDU/ITU care.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
Patients with peptic ulceration continue to present to surgeons with complications of bleeding or perforation and to die under surgical care.
Key messages
Mortality from peptic ulcer has declined both in the population generally but much more in surgical hospital patients.
Patients with complications of peptic ulceration admitted under surgical care should be offered: consultant surgeon input, timely surgery and HDU/ITU care.
Strengths and limitations of this study
Continuous prospective peer-reviewed audit data of mortality over 13 years.
Population data.
Absence of data on those who survived; the changing nature of the medical communities' understanding and treatment of peptic ulceration; selection bias effects in data omission or miscoding and the potential of specific changes in patient management.
Introduction
While elective surgery for peptic ulcer was once a mainstay of surgical practice, the advent of histamine type 2 (H2) receptor antagonists, proton pump inhibitors and Helicobacter pylori eradication has resulted in surgical therapy for peptic ulceration being confined to complications, such as perforation and bleeding.1 The frequency of such complications, particularly perforation, has increased especially in the elderly female population and may be related to the use of prescription medication.1–3 However, the incidence of peptic ulcer disease in the general population is difficult to assess: individuals may be asymptomatic until emergency presentation with a complication requiring surgical intervention; self medication with antacids, H2 antagonists and proton pump inhibitors is difficult to quantify. The uptake of prescription medications is also a non-specific indicator as the most widely used medications, proton pump inhibitors, also have non-ulcer indications. In addition, improved prevention of peptic ulcers through eradication of H pylori and more judicious use of non-steroidal anti-inflammatory drugs (including companion medications) may be changing the epidemiology of peptic ulcer disease.
Quoted mortality from complications of peptic ulceration range between 4% and 30%,4–7 while morbidity has been reported for 25%–89% of those requiring surgical intervention.4 Delay to treatment, increased age, the presence of shock on admission, associated illnesses and chronic health recorded as American Society of Anaethesiologists status have been cited as significant factors associated with fatal outcomes.5–7 A delay in treatment of more than 24 h has shown to increase mortality up to eightfold and complications by three times.4
We considered that fewer deaths with peptic ulcer disease and a reduction in adverse events in clinical management over time should be expected with increasing consultant input, timely intervention and improved perioperative care. We examined the trend over time of Scottish Audit of Surgical Mortality (SASM) operative deaths per SMR01 operative patient, for patients diagnosed with peptic ulcer disease. We then looked at this relationship with operative deaths with adverse events, consultant surgeon involvement, use of high dependency/intensive therapy unit (HDU/ITU) and operation within 2 h.
Methods
The SASM (www.sasm.org.uk) aims to peer-review all patients who die under surgical care. Over a period of 13 years (1994–2006), deaths from peptic ulcer under surgical care were prospectively peer-reviewed using established methodologies previously detailed (8–10, http://www.sasm.org.uk). Subsequent changes in coding (for 2007 and 2008) and further modifications to SASM in 2009 and the interruption of SASM in 2010 pending transfer to an electronic web-based format do not allow direct comparison of data after 2006. In keeping with previous practice, ethical permission was not required for the use of audit data.8
Briefly, data were collected via completed proformas from the surgeon responsible for the patient's care during his/her final admission. On the surgical proforma, questions relate to consultant presence in the operating room taken from ‘grade of surgeon operating’ and ‘grade of surgeon assisting’; timing of operation from ‘operation within 2 h’ and if the patient ‘received HDU/ITU care or treatment’. These proformas were assessed by a surgical assessor (and anaesthetic assessor if any anaesthetic had been given). Based on this anonymous peer review, an evaluation is made of the care provided, highlighting any adverse events and fed back to the consultant surgeon and anaesthetist. Adverse events were defined as ‘care should have been better and contributed to or caused the patient's death’. Where further details are required or where concerns about patient management are raised by the first-line assessor, the case notes are retrieved and sent to a second assessor with experience in that particular area. After completion of assessment, each surgeon and anaesthetist receives individual feedback. Some 10% of cases undergo a full case note review.8–10 Widely circulated annual reports ensure that an overview of the data is promulgated to the surgical and anaesthetic community.
Patient admissions to hospital (recorded on Scottish Morbidity Record—SMR01episodes) with a diagnosis of gastric ulcer (ICD9 531 up to April 1996; ICD10K25 from April 1996 to the present day), duodenal ulceration (ICD9 532; ICD10K26), peptic ulcer, site unspecified (ICD9 533; ICD10K27) or gastrojejunal ulcer (ICD9 534; ICD10K28) were identified. These hospital admissions were patients admitted to the same surgical specialties as covered by the SASM audit (all surgical specialties apart from cardiac surgery, cardiothoracic surgery and obstetrics).
Similar Read Codes were used for the SASM analyses: gastric ulcer (J11), duodenal ulceration (J12), peptic ulcer, site unspecified (J13) or gastrojejunal ulcer (J14).
Statistical analysis
SASM data were managed within a custom MS Access data base. All data (SASM and SMR01) were analysed using SPSS version 19 (SPSS Inc). Linear regression was used to assess the significance of differences in categorical data. Based on the literature review, consultant input, use of HDU/ITU facilities, the timing of surgery and an analysis of adverse events were examined. p Values <0.05 were considered significant.
Results
There were 1952 patients who died (1338 operative and 614 non-operative deaths) over the 13 year period (1994–2006) where the diagnosis was peptic ulcer disease. Of these 1952 deaths, 1029 (52.7%) patients were women and the median age decreased from 77 to 76 years over time (range 27–102 years). There was a decline in the annual number of deaths from 251 deaths in 1994 to 83 in 2006 both for those who died following an operation and for those who did not undergo surgery. There was no notable change over time in American Society of Anaesthesiologists grade of the patients who died.
Contemporary with this fall in mortality under surgical care, 42 736 patients were admitted to hospital in surgical specialties covered by the SASM audit with a diagnosis of peptic ulcer from 1994 to 2006. The annual number of patients admitted declined from 3872 in 1994 to 2481 in 2006, 64.1% of the 1994 admissions (table 1).
Number of patients who died and admissions to surgical wards for patients with peptic ulceration 1994–2006
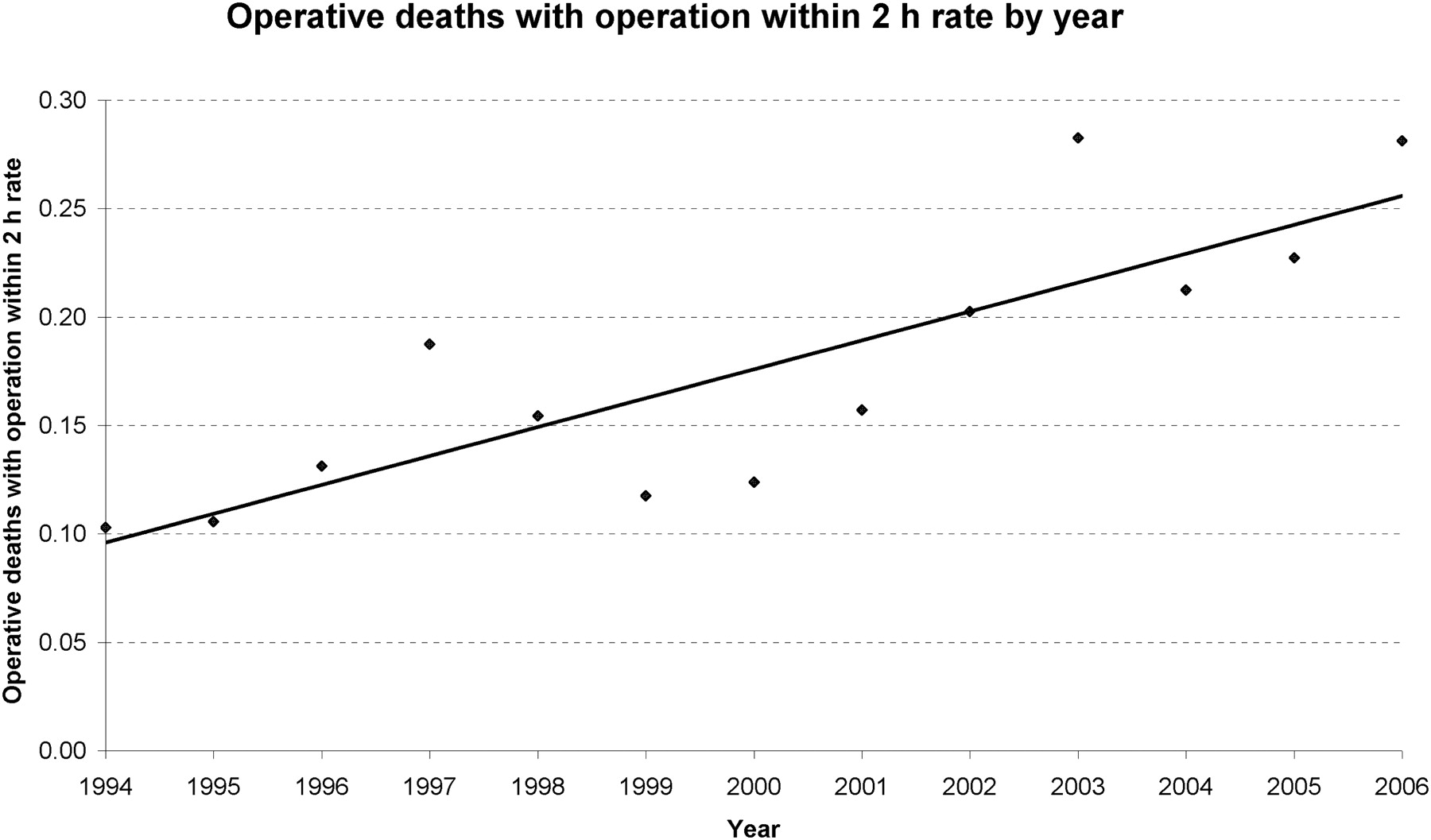
There was a significant increase in consultant input (operating or assisting in theatre) from 40.0% of operations in 1994 to 73.4% of operations in 2006. In 7.7% of the operative cases in 1995, a consultant assisted in theatre (11 cases) compared to 28.1% (18 cases) in 2006; however, 43.0% (66) of the patients were operated on by a consultant surgeon in 1994 compared to 50.0% (31 patients) in 2006. Furthermore, the proportion of operations performed within 2 h of admission increased from 10.3% in 1994 to 28.1% in 2006 (table 2). There was an increase in utilisation of HDU/ITU services in operative patients who subsequently died from 52.7% (87/165) in 1994 to 84.4% (54/64) in 2006 (table 1). Linear regression analysis confirmed a fall in operative deaths following surgery, increased consultant involvement (p=0.005) (figure 1), increased use of HDU/ITU (p=0.026) (figure 2), increased operation within 2 h (p=0.088) (figure 3). Increased consultant involvement and increased use of HDU/ITU for operative deaths were significant factors in the fall in operative death rate (number of SASM operative deaths with a diagnosis of peptic ulcer disease per SMR01 operative patient with a diagnosis of peptic ulcer disease).
Rates of operative death per year by consultant involvement, HDU/ITU care or time to operation

Consultant involvement in operations 1994–2006.

Utilisation of high dependency/intensive therapy unit (HDU/ITU) services 1994–2006 in patients who died under surgical care.

{kind=link}
{kind=link}
{kind=link}
Operative deaths of patients who had an operation within 2 h 1994–2006.
At least one adverse event contributing to or causing death was identified on peer review for 226/1338 (16.9%) of those patients who underwent surgery and in 27/614 (4.4%) of the non-operative patients who died. For each SASM case with an adverse event, at least one adverse event code has been identified. There can be more than one adverse event code for each case; therefore, the number of adverse event codes is greater than the number of cases with an adverse event.
The most common adverse events for operative deaths were delays: delay in transfer to surgeons by physicians (23/384 adverse events identified; 6.0%), delay to surgery (4.4%) and delay in transfer to the surgical unit (2.9%); however, surgeon too junior (4.9%) and inadequate resuscitation (3.4%) also featured (table 3). The most frequent causes of death were perforated or bleeding duodenal ulcers, septicaemia, peritonitis, bronchopneumonia, a cardiac event or multiple organ failure.
Adverse events associated with operative deaths (one patient may have more than one adverse event)
For non-operative deaths, adverse events such as delay in transfer to a surgeon by a physician, delay to surgery, diagnosis missed by medical unit or the view that an operation should have been done were noted.
Discussion
This study identified 1952 patients who died under surgical care over 13 years with the principle diagnosis of a ‘benign’ condition, peptic ulceration. There was a substantial fall by 2006, to a third of the 1994 figures, in deaths from peptic ulcer and adverse events under surgical care. This paralleled, but was proportionately much greater than, the 36% fall in admissions to hospital with peptic ulceration. Associated with, but not necessarily causal for, this disproportionate reduction in surgical mortality, there was a significant increase in consultant input in the operating theatre, prompt operating and enhanced perioperative care through HDU/ITU. This provides circumstantial evidence that improvements in the provision of healthcare may influence outcome and suggests further investigation of these domains of care in those who survive hospital admission.
Adverse events were identified in 226 (16.9%) of deaths where an operation was performed but only contributed in 27 (4.4%) patients who died without surgery; adverse events have certainly decreased over time. Where such events were identified, this study confirms that the majority of adverse events were problems of process (predominantly delays)8–10 rather than technical difficulties. Although the SASM process highlighted time to surgery as an adverse event, three times as many patients had their operations within 2 h by the end of the audit period. Delay to treatment remains important for complications and mortality from peptic ulcer, increasing the complication rate up to threefold and increasing mortality by up to eightfold.5
Such adverse events reflecting process should be amenable to protocol development based on guidelines or case analysis.11 Failure to use HDU/ITU was recognised as a frequent adverse event in the first 4 years of SASM and highlighted to the individual surgeon, hospital trust and public by the SASM annual reports. Following significant media attention, the subsequent enhanced provision of HDU/ITU facilities in hospitals in Scotland was associated with a decline in failure to use HDU/ITU as an adverse event,9 confirmed in the current study and supported by guideline development.11 Thus, adoption of evidence-based initiatives to improve the process of care may have a considerable impact on clinical practice.
Further reductions in adverse events related to process and the seniority of staff may be achieved by enhancing team integration among hospital staff12 together with the use of risk stratification and a suitable risk-group-based management.13 There remains potential for improvements in the process of care,8–10 with consultant staff performing early triage of emergency surgical and medical admissions potentially reducing delays in transfer to appropriate care and to surgery (table 3).
This analysis shows the benefits of continuous and complete audit data over a sustained time frame using individual feedback, annual reporting (http://www.SASM.org) and, more recently, individual annual reports for surgeons, for anaesthetists and for hospital Trusts to observe significant changes in practice. SASM demonstrates the benefits of a large, prospective, population-based, validated, high-quality data set. Evidence using similar methodology in Western Australia suggests that surgical mortality audit does have a direct impact: 73% of surgeons changed their practice in at least one way, 24% noted changes in hospital practice and 11% changes in colleague's practice.14
However, the potential weaknesses of this study include the absence of data on those who survived; the changing nature of the medical communities' understanding and treatment of peptic ulceration; selection bias effects in data omission or miscoding and the potential of specific changes in patient management.
Whether this mortality audit reflects improvements in care of those who do not die following hospitalisation with peptic ulceration remains uncertain. However, the fall in the number of deaths under surgical care has been disproportionately larger than the fall in hospital admissions with peptic ulcer. There is potential for confounding via cohort effects, including changes in patient's behaviours, in the disease itself, changes in therapy and changes in the SASM process. However, increased consultant input, more prompt operating and enhanced use of HDU/ITU have been identified alongside a reduction in adverse events for those who died.
Acknowledgments
The authors thank Gillian McPhillips and Garry Hecht for their contributions to the paper.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data Supplement - Manuscript file of format pdf
Footnotes
Presentation: Oral presentation to the Association of Surgeons of Great Britain and Ireland, Glasgow, May 2009.
To cite: Aga H, Readhead D, MacColl G, et al. Fall in peptic ulcer mortality associated with increased consultant input, prompt surgery and use of high dependency care identified through peer-review audit. BMJ Open 2012;2:e000271. doi:10.1136/bmjopen-2011-000271
Contributors This research was conducted by HA designed by AT and analyses performed by DR and GM; all authors contributed to the analysis, writing and final review of the manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests The authors declare that they have no conflict of interest; specifically no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years, no other relationships or activities that could appear to have influenced the submitted work.
Ethics approval Ethics approval was not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Mortality and audit data analysed for this publication can be shared for further analyses; interested parties should contact the corresponding author.