Article Text

Abstract
Objectives Small cell lung cancer (SCLC) is a lethal human malignancy, and previous studies support the contribution of microRNA to cancer progression. The prognostic value of miR-219-5p in patients with SCLC remains unclear. This study aimed to evaluate the predictive value of miR-219-5p with respect to mortality in patients with SCLC and to incorporate miR-219-5p level into a prediction model and nomogram for mortality.
Design Retrospective observational cohort study.
Setting and participants Our main cohort included data from 133 patients with SCLC between 1 March 2010 and 1 June 2015 from the Suzhou Xiangcheng People’s Hospital. Data from 86 patients with non-SCLC at Sichuan Cancer Hospital and the First Affiliated Hospital of Soochow University were used for external validation.
Outcome measures Tissue samples were taken during admission and stored, and miR-219-5p levels were measured at a later date. A Cox proportional hazard model was used for survival analyses and for analysing risk factors to create a nomogram for mortality prediction. The accuracy of the model was evaluated by C-index and calibration curve.
Results Mortality in patients with a high level of miR-219-5p (≥1.50) (n=67) was 74.6%, while mortality in the low-level group (n=66) was 100.0%. Based on univariate analysis, we included significant factors (p<0.05) in a multivariate regression model: patients with high level of miR-219-5p (HR 0.39, 95% CI 0.26–0.59, p<0.001), immunotherapy (HR 0.44, 95% CI 0.23–0.84, p<0.001) and prognostic nutritional index score >47.9 (HR=0.45, 95% CI 0.24–0.83, p=0.01) remained statistically significant factors for improved overall survival. The nomogram had good accuracy in estimating the risk, with a bootstrap-corrected C-index of 0.691. External validation indicated an area under the curve of 0.749 (0.709–0.788).
Conclusions The miR-219-5p level was associated with a reduced risk of mortality in patients with SCLC. A nomogram incorporating MiR-219-5p level and clinical factors demonstrated good accuracy in estimating the risk of overall mortality. Prospective validation of the prognostic nomogram is needed.
- risk management
- oncology
- gene therapy
- molecular aspects
- oncogenes
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The study uses databases of all patients with small cell lung cancer (SCLC) in two defined geographical regions of China.
The study included the creation of a nomogram for predicting survival probabilities in individual patients.
However, the model is not comprehensive since the database does not include all prognostic factors for SCLC.
Additionally, the available data on treatment status are not adequately detailed to distinguish the impact of various treatment plans.
The model needs to be prospectively assessed to determine its reliability.
Introduction
Lung cancer is the leading cause of cancer deaths worldwide, with millions of new cases diagnosed each year.1 Small cell lung cancer (SCLC) is a kind of neuroendocrine malignant tumour with poor prognosis, accounting for about 15% of patients with lung cancer.2 SCLC is generally divided into limited disease (LD-SCLC) and extensive disease (ED-SCLC). A combination of platinum and etoposide regimen is the first-line therapeutic strategy for SCLC, and most patients are easy to receive initial chemotherapy.3 However, the 5-year survival rates of LD-SCLC and ED-SCLC are only 15% and 3%, respectively.4 Therefore, improvement in early diagnosis and prognostic prediction of SCLC is vital.
MicroRNAs (miRNAs) are endogenous non-coding RNAs (~22 nt), which regulate mRNA activity by hybridisation with 3’-untranslated region of specific genes.5 Many studies have shown that miRNAs could have a role in a variety of cell biological processes, including cell growth, differentiation and apoptosis.6 7 In addition, researches have demonstrated that miRNAs are frequently dysregulated in cancers,8 9 and some miRNAs can serve as diagnostic and prognostic biomarkers for cancers.10 Recently, several miRNAs have been proven to have a role in the occurrence and development of SCLC, but few of them are likely to be a biomarker or therapeutic target for SCLC.
Recently, miR-219-5p has been found to be abnormally expressed and play a significant role in different cancers. Ma found that the expression of miR-219-5p was significantly decreased in oesophageal squamous cell carcinoma tissues compared with normal tissues.11 A study by Gong et al revealed a tumour suppressive role of miR-219-5p by targeting glypican-3 in hepatocellular carcinoma (HCC).12 On the contrary, Yang et al indicated that miR-219-5p could promote cell growth and metastasis of HCC and serve as a prognostic marker for patients with HCC.13 A research investigated by Wei et al suggested that miR-219-5p could inhibit proliferation, migration and invasion of epithelial ovarian cancer through downregulation of the Wnt signalling pathway, and it could serve as a diagnostic biomarker and therapeutic target for epithelial ovarian cancer.14 However, the biological functions of miR‐219-5p and its potential prognostic role as a biomarker in SCLC are still unknown.
In this study, we aimed to examine the variation in the expression levels of miR-219-5p in patients with SCLC, to evaluate the predictive value of miR-219-5p with respect to mortality in patients with SCLC, and to incorporate miR-219-5p level into a prediction model and nomogram for mortality.
Methods
Study design and patients
The study uses databases of all patients with SCLC in two defined geographical regions of China. Our main cohort included data obtained from 133 patients with SCLC between March 2010 and June 2015, in the Suzhou Xiangcheng People’s Hospital. Tissue samples were taken during admission and stored, and the miR-219-5p levels were measured at a later date. Those participants who lacked information on complement components data, withdrew from treatment or lacked follow-up information were excluded. Clinical information of patients, including gender, age, body mass index, neutrophil count, lymphocyte count, serum carcinoembryonic antigen (CEA) level, C reactive protein (CRP) level, albumin level, haemoglobin level, stage of SCLC, platelet count, prognostic nutritional index (PNI) score, Karnofsky Performance Status (KPS) score, neutrophil–lymphocyte ratio, pathological type, immunotherapy, radiation therapy, use of platinum, use of vascular endothelial growth factor inhibitor, target therapy, use of tyrosine kinase inhibitor (TKI), smoking, acute coronary syndrome (ACS), diabetes, heart failure and hyperlipaemia, were recorded. Diagnosis of SCLC was confirmed by histopathological examination. The median length of follow-up was 23.6 months. Median was used as the cut-off value. The definition and details of all the variables above were provided in online supplemental material part I. Data from 86 patients with non-SCLC (NSCLC) at Sichuan Cancer Hospital and the First Affiliated Hospital of Soochow University were used for external validation.
Supplemental material
Assays for detection of miR-219-5p levels
The quantitative reverse transcription-PCR (qRT-PCR) was conducted for the detection of miR-219-5p expression levels.
Total RNA from tissues was isolated and extracted using miRcute Extraction and Separation of miRNAs kit (Tiangen Biotech Co, Beijing, China), and then reversely transcribed into cDNA by PrimeScript Ⅱ 1st strand cDNA synthesis kit (Takara Biotechnology Co, Dalian, China) according to the manufacturer’s protocol. SYBR PrimeScript miRNA RT-PCR kit (Takara Biotechnology Co) was used for qRT-PCR. The thermocycling conditions were as follows: one cycle at 95°C for 3 min (initial denaturation), 40 cycles at 95°C for 15 s and 60°C for 30 s. U6 small nuclear RNA (U6) served as the respective internal control. The relative expression of miR-219-5p was quantified by the 2-ΔΔCt methods and normalised to the U6. The following primers were used: miR-219-5p forward, 5’-ACACTCCAGCTGGGTGATTGTCCAAACGCAAT-3’ and reverse, 5’-CTCAACTGGTGTCGTGGA-3’; U6 forward, 5’-GCTTCGGCAGCACATATACTAAAAT-3’ and reverse, 5’-CGCTTCACGAATTTGCGTGTCAT-3’. The experiments were repeated at least three times.
Statistical analysis
Sample size assessment was performed using NCSS-PASS software V.11.0 (https://www.ncss.com/software/pass/). Power was set as 0.99, and α was set as 0.5. The mortality data in both the groups with high-level miR-219-5p and low-level miR-219-5p in our previous data (2008–2009) (0.750 and 0.950) were entered into the PASS. The actual HR was set as 0.50. Then, the sample size was calculated using PASS, and the minimum sample size was 94 (control=51, experiment=43). Our sample size was 133 (66 and 67, respectively, for each group), which was suitable. The report of sample size assessment was displayed in online supplemental material part II. The missing data (<5.0%) were estimated by random forest algorithm using the mice package in RStudio (R V.3.6.1). Categorical variables were presented as percentages and compared via the κ² test. Continuous variables with skewed and normal distributions were presented as median with IQRs and mean±SD. The Mann-Whitney U test and the unpaired t-test were applied for comparison between groups. Cumulative mortality was shown by the Kaplan-Meier curve and analysed by the log-rank test. Univariate and multivariate survival analyses for overall survival (OS) were conducted using the Cox regression model. The forest plots were used to visualise the significance of covariates to the prognosis. The restricted cubic spline analyses were performed with Harrell’s Regression Modelling Strategies (rms) package.
We screened multifactor analysis for statistically significant indicators for inclusion in the prediction model. To build the nomogram, we found the position of each variable on the corresponding axis, drew a line to the points axis for the number of points, added the points from all the variables and drew a line from the total points axis to determine the OS probabilities at the lower line of the nomogram. The contribution of each covariate was quantified and visualised in a prognostic nomogram with internal validation via 1000-time bootstrapping. The consistency of the resulting model was assessed by the calibration assay. Decision curve analyses were performed to evaluate net clinical benefits of the model compared with conventional prognostic scores. The scatter plots were applied for visualisation of the consistency of each model. A 1000-time bootstrapping was employed as indicated. The association between miR-219-5p class and survival endpoints was evaluated by Kaplan-Meier curves and log-rank test. Statistical analysis was performed using the RStudio (R V.3.6.1) with the following packages: ‘ggplot2’, ‘rms’, ‘PredictABLE’, ‘risk regression’ and ‘survminer’.
Patient and public involvement
None.
Results
Baseline characteristics
A total of 133 patients with SCLC who were diagnosed between March 2010 and June 2015 were included in the main cohort. A flow chart of the screening process was shown in figure 1. The median age of these patients was 64 years old (58–70 years), and 106 (80.0%) were male. Median serum CEA and CRP level was 3.43 ng/mL and 7.83 µmol/L, respectively. For the stage of SCLC, 51 (38.0%) patients were diagnosed with LD-SCLC, while 82 (61.0%) patients were diagnosed with ED-SCLC. Twenty-five (19.0%) patients accepted the immunotherapy, while 54 (41.0%) patients got the radiation therapy. In addition, platinum was used for 131 (98.0%) patients, and TKI was used for 15 (12.0%) patients. The KPS score of these patients was examined, and the results revealed that 107 (81.0%) patients got 80 or higher points. The distribution of basic diseases was also assessed in our data. Diabetes was found in 17 (13.0%) patients, and hyperlipaemia in 13 (10.0%) patients. Cardiovascular diseases such as heart failure and ACS were found in three (2.0%) and four (3.0%) patients, respectively. Thirteen (10.0%) patients suffered from hypertension. In addition, 82 (62.0%) patients had a habit of smoking. The baseline characteristics of these patients were listed in table 1.

Study screening flow chart. SCLC, small cell lung cancer; SLE, systemic lupus erythematosus.
Study participant characteristics at enrolment
Among all the 133 patients, overall mortality was 87.2%. The mortality in the group with high-level miR-219-5p (n=67) was 74.6%, while the mortality in the low-level group (n=66) was 100.0%. Moreover, in the group with high-level miR-219-5p, there were 35 (52.0%) patients with ED-SCLC, while in the low-level group, there were 47 (71.0%) (table 1).
miR-219-5p expression level and clinical risk factors
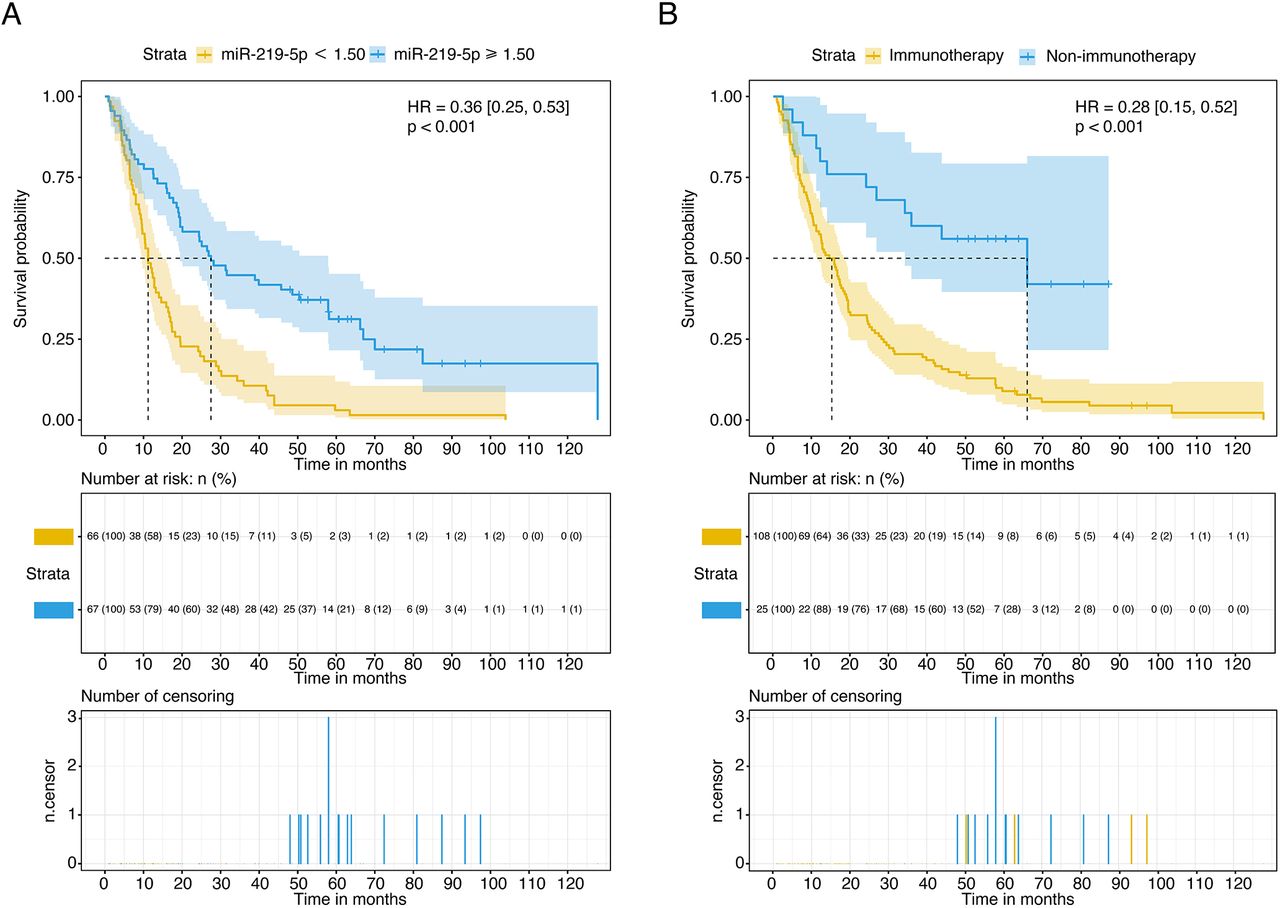
According to the univariate analysis, having high levels of miR-219-5p (≥1.50) was a strong protective predictor of mortality (HR 0.36, 95% CI 0.25–0.53, p<0.001) (table 2). The Kaplan-Meier curve showed that patients in the group with high levels of miR-219-5p had a decreased cumulative rate of death compared with those in the group with low levels of miR-219-5p (log-rank p<0.001) (figure 2A). Meanwhile, patients who accepted immunotherapy also showed a low morality compared with those patients not accepting immunotherapy, as shown in the survival curve (HR 0.28, 95% CI 0.15–0.52, p<0.001) (figure 2B).

Overall survival (OS) of patients with SCLC with different levels of miR-219-5p and different treatments. (A) OS of patients with SCLC with high or low level of miR-219-5p. (B) OS of patients with SCLC with different treatments (immunotherapy vs non-immunotherapy). SCLC, small cell lung cancer.
Results of univariate Cox regression analysis for overall mortality
In addition, gender, age, serum CRP level, albumin level, lymphocyte count, PNI score, immunotherapy, heart failure and KPS score were also correlated with overall mortality (table 2). When adjusted by age and gender, patients in the group with high-level miR-219-5p also displayed a low cumulative rate of death compared with those in the low-level group.
Independent prognostic factors for OS
After the multivariate adjustment, having a high level of miR-219-5p (HR 0.39, 95% CI 0.26–0.59, p<0.001) was also associated with a low increase in the risk of death (figure 3). Meanwhile, gender, PNI score, immunotherapy and heart failure were also the independent risk factors for OS.

Multivariate Cox regression analysis of 5-year overall survival. CRP, C reactive protein; KPS, Karnofsky Performance Status; NLR, neutrophil–lymphocyte ratio; PNI, prognostic nutritional index.
Development and validation of an OS prediction nomogram
The independently related risk factors derived from the multivariate analysis were used to create an OS estimation nomogram (figure 4A). The prognostic model was internally validated according to the bootstrap validation method. With an unadjusted C-index of 0.691 and a bootstrap-corrected C-index of 0.691, the nomogram displayed excellent accuracy in estimating the risk of OS. In the validation cohort, the nomogram showed a C-index of 0.691 for the estimation of OS. A suitable calibration curve for risk estimation was also displayed (R2=0.455, likelihood-ratio Χ2=80.55) (figure 4B). We collected 86 patients with NSCLC from Sichuan Cancer Hospital in the external validation step. The receiver operating characteristic curve showed an area under the curve (AUC) of 0.783 (0.743–0.822) for predicting 5-year OS, compared with an AUC of 0.749 (0.709–0.788) for the external validation data (figure 5). We calculated the total score using the nomogram for patients in the training and validation sets, respectively, and divided them into four groups (40–60, 61–80, 81–100, 101–120), and performed Kaplan-Meier analysis and plotted survival curves, which were found to have good separation and were statistically significant (online supplemental figure 1A,B).
Supplemental material
Supplemental material

Nomogram for overall survival (OS) risk estimation and its predictive performance. (A) Nomogram to estimate the OS risk of patients with SCLC. (B) Validity of the predictive performance of the nomogram in estimating the OS risk. LR, likelihood-ratio; SCLC, small cell lung cancer.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
External validation of the prognostic model. AUC, area under the curve.
Discussion
In this study, we detected the expression of miR-219-5p in a large cohort of patients with SCLC at a single institution, between March 2010 and June 2015. The results suggested that reduced expression of miR-219-5p was significantly correlated with unfavourable clinical features. Moreover, patients in the group with high-level miR-219-5p expression displayed better OS compared with those in the group with low-level miR-219-5p expression. The multivariate analysis demonstrated miR-219-5p as an independent prognostic factor for OS. In addition, to propose, and retrospectively verify an independent cohort of patients, these independent risk factors were applied to establish a nomogram for OS estimation. The nomogram revealed good accuracy in estimating the risk of OS.
Carcinogenesis involves multiple biological processes, which are related to many key genes.15 16 The characteristics of cancer occurrence represent properties that a cell acquires a certain ability to become and maintain itself as a cancer cell.17 The key genes guide the cellular signalling pathways related to occurrence and progression of cancers.18 19 Using miRNA expression to predict the clinical diagnosis and prognosis of cancer has more advantages than mRNAs, as miRNAs are proven to be the vital post-transcriptional regulators of gene expression.20 21 In comparison with mRNAs, these vital gene regulators are highly conserved among species.22
It has been reported that miRNAs were related to the initiation and progression of various cancers, and many miRNAs have been identified as a promising biomarker for prognostic prediction of cancer.10 23 Recently, some miRNAs have been proven to be a novel prognostic biomarker for SCLC.24 25 A study by Yu et al indicated that miR-92a-2 was significantly higher in a group of patients with SCLC compared with a healthy control, and detection of miR-92a-2 levels could be a potential biomarker for patients with SCLC.26 As a promising biomarker, miR-219-5p has been identified as a prognostic factor for different cancers. Long et al found that miR-219-5p expression level was distinctly decreased in melanoma tissues and cell lines, and the modulation of miR-219-5p expression could be a prognostic biomarker and treatment strategy in melanoma.27 A study from Huang et al suggested a role of miR-219-5p for prognostic prediction and therapeutic strategy in colorectal cancer.28 However, there are no studies exploring the role of miR-219-5p as a biomarker in patients with SCLC. To the best of our knowledge, this study was the first attempt ever made to comprehensively evaluate the role of prognostic prediction based on miR-219-5p expression in patients with SCLC. In the current study, we initially examined the expression levels of miR-219-5p in patients with SCLC. We, for the first time, demonstrated a correlation of the altered miR-219-5p expression with available clinical parameters. We found that miR-219-5p was significantly associated with lymphocyte count, PNI score and stage of SCLC. The univariate analysis indicated that increased miR-219-5p expression was a protective predictor for mortality. The Kaplan-Meier curve displayed that patients with elevated miR-219-5p expression levels or accepted immunotherapy had low cumulative incidence of death compared with those with reduced miR-219-5p expression or unaccepted immunotherapy, respectively. In addition, gender, age, serum CRP level, albumin level, lymphocyte count, PNI score, immunotherapy, heart failure, KPS score and miR-219-5p level were associated with overall mortality. The multivariate analysis showed that miR-219-5p, gender, PNI score, immunotherapy and heart failure could predict OS as the independent risk factors.
Nomograms are applied for visualisation of statistical models, graphical evaluation of variable significance and examination of predicted values.29 30 They have been widely used to predict cancer risks and therapeutic outcomes.31 32 Most recently, several studies have successfully established a prognostic nomogram that combined an miRNA with clinical-related variables for OS estimation in different cancers.33–35 Although a nomogram is becoming increasingly popular, no studies have built prognostic models using a combination of miR-219-5p and clinical risk factors in patients with SCLC. In this study, based on the combination of miR-219-5p and independent clinicopathological variables, we created a nomogram model that could provide an individual prognostic prediction for OS estimation in patients with SCLC. The results indicated excellent accuracy in estimating the risk of OS. There was a suitable calibration curve for risk estimation, indicating a well-performed nomogram, and good agreements between observation and prediction. To further verify the accuracy and efficiency of the model, an external data collection containing 86 patients from Sichuan Cancer Hospital was conducted. The results indicated that the prognostic model could accurately predict the prognosis of patients with SCLC. Hence, this was the first prognostic nomogram for patients with SCLC that considered clinical parameters in addition to miR-219-5p. This nomogram could provide comprehensive information for patients, as well as a better guidance for clinical therapy. Based on the model, the potential high-risk patients with low survival rate could be more accurately selected for a specific therapeutic strategy.
Strengths and limitations
We screened valid variables by Cox regression to construct a survival prediction model for SCLC and collected data for external validation in a logical manner. However, there are some limitations in this article. First, experimental research explaining the biological processes of miR-219-5p is needed. Thus, the molecular mechanism of miR-219-5p should be investigated in further research. Second, the prognostic nomogram needs to be further assessed in a prospective and large-scale multicentre study before it can be applied to clinical practice. Finally, our data lacked some of the risk factors associated with SCLC for inclusion, such as the determination of some of the high-risk genes and the patient’s previous chemotherapy and specific targeted therapies, which will require further analysis in our future studies.
Conclusions
In conclusion, we found that the miR-219-5p expression levels were significantly correlated with clinical parameters of patients with SCLC. Furthermore, miR-219-5p was proven to be an independent factor for prognostic prediction in patients with SCLC. Moreover, a nomogram based on multivariate analysis and including miR-219-5p expression levels showed excellent accuracy in estimating the risk of OS. However, a prospective validation of the prognostic nomogram will be needed in the future.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
For both the main cohort and the validation cohort, informed consent was obtained from all patients or their immediate family members for the collection and storage of samples and their use for future scientific research. All procedures were in line with the guidelines of the ethics committee of Suzhou Xiangcheng People’s Hospital (20140193), Sichuan Cancer Hospital and the First Affiliated Hospital of Soochow University. The study was performed in accordance with the Declaration of Helsinki.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
XW, JZ and XZ contributed equally.
Deceased 2
Contributors ZX, XW and ZC designed the study. ZC, XZ, JZ and MX collected and analysed the data. XW, ZC, JZ and XZ drafted the initial manuscript. ZX, XW and ZC reviewed and edited the article. ZX served as guarantor accepted full responsibility for the work and controlled the decision to publish. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.