Article Text

Abstract
Objective The degree awarding gap indicates that racially minoritised higher education students receive lower degree classifications relative to their white peers. While the reasons for this are complex, research suggests that educator and practitioner attitudes and behaviour towards racially minoritised students are a significant contributing factor. This preregistered study evaluates the effectiveness of unconscious racial bias training (URBT) to enhance National Health Service senior practitioner’s recognition of how racial inequalities negatively impact racially minoritised students.
Design A mixed-methods study with a pretest and post-test design was conducted in the higher education and healthcare practice environment.
Methods Forty-nine NHS senior practitioners completed a 4-hour URBT workshop with activities focusing on activating stereotypes, exploring differences between unconscious and implicit bias, discussing the development of bias, and reflecting on student experiences of prejudice, harassment and discrimination. They completed pre- and post- quantitative measures that assessed the effectiveness of URBT and changes in racial competency, awareness and perceptions of unconscious racial bias. Qualitative measures explored the usefulness and perceived applications of URBT, and a 1-month follow-up assessed further how it had been applied within practice.
Results Participants reported positive evaluations of URBT, higher perceived racial competency, awareness and perceptions of racial bias (ps<0.001, dz>0.35). After 1 month, key themes from qualitative responses suggested that participants had increased self-awareness and were exploring how to set up mentoring and working groups, change recruitment and progression processes, and diversify the taught curriculum.
Conclusions URBT may be one effective strategy to enhance awareness and encourage reflections of racial bias. We discuss how reducing racial inequalities requires a multifaceted approach that affords upfront conversations about systemic racism, implements effective initiatives, policies and procedures, and engages in continuous evaluation.
- EDUCATION & TRAINING (see Medical Education & Training)
- GENERAL MEDICINE (see Internal Medicine)
- HEALTH SERVICES ADMINISTRATION & MANAGEMENT
- Health policy
- Organisational development
- Human resource management
Data availability statement
Data are available in a public, open access repository. The design and analysis plan were preregistered via the AsPredicted.org template on the Open Science Framework (https://osf.io/5w8fc). All materials, anonymised data, and analysis syntax are publicly available, as well as a statement outlining any necessary deviations to the preregistration protocol (48; https://osf.io/yfa6s/).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- EDUCATION & TRAINING (see Medical Education & Training)
- GENERAL MEDICINE (see Internal Medicine)
- HEALTH SERVICES ADMINISTRATION & MANAGEMENT
- Health policy
- Organisational development
- Human resource management
STRENGTHS AND LIMITATIONS OF THIS STUDY
In line with recommendations, unconscious racial bias training was delivered to National Health Service (NHS) senior practitioners in the practice and higher education environment and focused explicitly on increasing awareness of and concern about racial bias. NHS senior practitioners are in leadership and management positions that allow them to implement significant changes, so this targeted population represents a strength of our research.
We used a mixed-methods approach to evaluate the training, gathering both quantitative and qualitative outcome measures, as well as exploring how the training had been implemented in practice 1 month later.
Our study assessed self-report evaluations and perceptions but did not assess longer-term objective measures of behaviour change (eg, changes in student attainment, staff retention, progression and disciplinary hearings for racially minoritised individuals).
Research suggests that the effectiveness of training may decay over time so a longer or additional follow-up period would be fruitful (however, this can introduce an equitable challenge of greater response attrition).
Introduction
The NHS was established on the principles of social justice and equity. In many ways, it is the nation’s social conscience, but the treatment of our colleagues from minority groups falls short far too often. (NHS People Plan, 2020/21, pp. 23).
Racial inequalities persist within education, healthcare and workplace settings in the UK. As students, racially minoritised individuals are awarded significantly lower degree classifications than their white peers.1–3 As healthcare patients, they have poorer access to services, receive inadequate treatment, and their mortality rates are higher.4–7 As healthcare practitioners, they experience racial discrimination and harassment, report more risks to their personal safety, are less represented at senior levels, and face more obstacles in their career progression.8–11 As reported in the British Medical Journal’s special issue on ‘racism in medicine’, these statistics have remained stable over the past twenty years and require urgent action.12 13 The National Health Service (NHS) has responded to these concerns, outlining their commitment to addressing racial inequalities for staff, students and patients through the Workforce Race Equality Standard,14 NHS People Plan15 and Race and Health Observatory.16 17 Despite these reports showing some signs of progress, the NHS recognises that continuous improvement is required for them to become a fully inclusive, equitable and fair organisation.
The UK government has also announced that it demands improvements to the experiences and attainment of racially minoritised students in higher education, putting the spotlight on the sector to explore factors involved in the ‘degree awarding gap’ and make a genuine pledge to reduce racial disparities.18 19 The degree awarding gap indicates the percentage point difference between the proportion of UK-domiciled white and racially minoritised students awarded a first or 2:1 degree classification on graduation.1 Despite holding equivalent entry qualifications, racially minoritised students are approximately 13% less likely to be awarded a first or 2:1 grade compared with their white peers, which is significantly greater than that of all other student groups.1–3 This increases to 23% when looking at Black students exclusively, resulting in a ‘leaky pipeline’ with Black students 1.5 times more likely to discontinue their studies compared with any other racial group.3 Importantly, these disparities are suggested to be caused by the higher education environment itself, with racially minoritised students reporting problems relating to the academic environment, curriculum, assessment practice and academic support.20–22 They also report experiences of microaggressions—defined as subtle or offensive comments, action or inaction directed at a minority group23 24—that adversely impacts their sense of belonging, confidence, mental health and progression at university.25–28
Students studying for a healthcare degree (eg, nursing, midwifery) in the UK undertake clinical practice placements alongside their studies. However, these placements have been found to be racially hostile environments that present a daunting prospect for racially minoritised students.29 30 The Equality and Human Rights Commission19 reports that 56% of students have been racially harassed while on placement or within the university campus. Despite this, many universities are slow and sometimes unresponsive to act: a freedom of information request indicated that, out of 40 medical schools in the UK, only half collected data on students’ complaints regarding racism and racial harassment.31 Shockingly, data also indicate that out of 60 000 students across the UK who made a complaint of racial harassment to their university in 2015/2016, only 560 were officially recorded.19 Similar trends are also evident in the workplace. Data from the NHS Workforce Race Equality Standard report14 show that 15.3% of racially minoritised staff experience discrimination from their colleagues compared with only 6.4% of white staff, with this disparity present within 82.7% of NHS Trusts. Furthermore, only 40.7% of racially minoritised staff believe that their organisation provides equal opportunities for career progression or promotion compared with 88.3% of white staff, which is reflected in their representation with only 9.2% in senior management roles. Combined, racial inequalities within higher education and healthcare practice disproportionately impact the achievement, retention and progression of racially minoritised students and staff and reflect the broader issue of systemic racism within UK society.29
Although the reasons for the degree awarding gap are complex and multifactorial, research suggests that educator and practitioner attitudes and behaviour towards racially minoritised students are a significant contributing factor.32 33 Bhopal and Pitkin32 explain how the enactment of the Race Equality Charter—a measure recently introduced to address racial inequalities in higher education—actually works to enhance the reputation of the sector rather than tacking structural disadvantages faced by racially minoritised students. This can also be seen in the way the degree awarding gap is discussed, and the interventions put forward to mitigate it. Specifically, the apparent differences in academic achievement between racially minoritised and white students are often portrayed through a deficit model. This model focuses on the personal attributes and characteristics of racially minoritised students (eg, their perceived lack of skills, knowledge or experience) as explanations for attainment differences, therefore, ascribing blame to the students themselves rather than an environment which perpetuates structural and institutional racism.1 32 This is acknowledged by the NHS who state that efforts to improve racially minoritised staff representation at more senior levels have been overshadowed by an ‘over-focus on the deficit model; the notion that there are inherent weaknesses or deficits among BAME staff themselves, rather than deep-rooted issues within organisations’ (WRES Implementation Team, pp. 11).34
The persistent evidence of racial inequalities for minoritised students and staff, coupled with global events such as the murder of George Floyd, have prompted universities and the NHS to address their roles in perpetuating racism and inequality. Task forces have been set up across the UK and USA to confront racism and to decolonise the taught curriculum, and statements have been disseminated by universities to signal a commitment to antiracist actions.35–37 Although these initiatives make it seem like progress is being made, many of them are inadequate, implemented without input from racially minoritised individuals, do not lead to sustained change and can lead to high-status group members reacting defensively.32 38–41 One active step has been to recommend that educators and healthcare practitioners undergo unconscious bias training (UBT) (also referred to as ‘diversity training’19 20 42), which aims to teach people about the snapshot judgements we make about others and how this can impact our attitudes and behaviour.43 The goal of this training is to encourage people to acknowledge their biases and consider their source, while also exploring proactive steps that they can take to promote an inclusive environment that challenges racism.
A large-scale evaluation42 found that across 18 studies, UBT was effective for awareness raising and reduced unconscious bias within advanced training designs.44 45 However, this report also highlighted that there was typically no long-term impact on behaviour following UBT, as well as the potential for the training to backfire when it is implied that stereotypes and biases are unchangeable. At first glance, this report seems to conclude that there is insufficient evidence to indicate that UBT is effective for behaviour change, however, the authors propose two main reasons for the mixed findings to date: (1) research examining behaviour change is limited and (2) methods for evaluating behaviour change mostly have low validity in that they do not measure actual observed change. Another review46 states that the current evidence base is hindered by examining the effectiveness of UBT in university student populations and US-based settings, suggesting that there is a need for robust, repeated behavioural studies of UBT interventions in UK workplaces. Others have suggested that diversity initiatives, such as UBT, should be improved to focus on explicitly increasing awareness of and concern about racial bias, planting seeds that inspires continued learning, and teaching strategies that allow participants to change their behaviour.47
Informed by these recommendations, we developed and evaluated an unconscious racial bias training (URBT) workshop delivered to NHS senior practitioners in the practice and healthcare environment. The implementation of this training represents a coordinated effort between the NHS and UK higher education to enhance awareness of how racial inequalities negatively impact racially minoritised students as one strategy to reduce the degree awarding gap. The overarching research question centres on whether URBT is effective in increasing knowledge, perceptions and awareness of racial bias, and can lead to a process of reflection and change. The following hypotheses were preregistered:
H1: Evaluation of training. There will be an increase in positive evaluations of UBT from pre- to post-training suggesting that the training increased understanding of unconscious racial bias and willingness to engage and promote the training.
H2: Racial competency. There will be an increase in racial competency (ie, racial beliefs and self-efficacy) from pre- to post-training suggesting that the training encouraged practitioners to reflect on their beliefs around race and how these impact mentoring, supervision and interactions with racially minoritised students/staff.
H3: Awareness of unconscious bias. There will be an increase in awareness of unconscious racial bias from pre- to post-training suggesting that the training enhanced recognition, awareness and the impact of unconscious racial bias on racially minoritised students/staff.
H4: General perceptions of bias. There will be an increase in perceptions of personal, societal and professional bias from pre- to post-training suggesting that the training made people reflect more globally about these forms of bias and how they affect decision-making.
As well as examining immediate pre–post changes, we also assessed qualitative responses regarding the usefulness of the training and explored the degree to which participants had applied this in practice 1 month later.
Method
The design and analysis plan were preregistered via the AsPredicted.org template on the Open Science Framework (https://osf.io/5w8fc). All materials, anonymised data and analysis syntax are publicly available, as well as a statement outlining any necessary deviations to the preregistration protocol (48; https://osf.io/yfa6s/).
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Design
A quasi-experimental pretest-posttest design was combined with an explanatory mixed-methods approach.49 The quantitative component comprised immediate pre- and post questionnaire measures and a 1-month follow-up questionnaire to evaluate the effectiveness of URBT. The qualitative component included open-ended questions regarding the usefulness and applications of the training. The URBT workshop and its evaluation were co-developed in line with recent large-scale evaluations42 46 47: specifically, we ensured that the training was: (1) explicitly aimed at increasing understanding and awareness of unconscious racial bias, (2) tailored to the healthcare environment; (3) discussed the impact on racially minoritised students and staff; (4) acknowledged potential feelings of discomfort and their importance; (5) explored strategies to mitigate bias with a focus on behaviour change and (6) included a follow-up to assess the application of training in practice. Outcome measures were selected based on their previously demonstrated rigour.42
Participants
Senior nursing and midwifery practitioners from two NHS Trusts and a higher education institute were recruited via opportunity sampling to attend URBT. Our sample size justification was therefore based exclusively on resource constraints: specifically, the number of individuals who agreed to participate in the training. Sixty-one participants provided pre-training responses for our primary outcomes, but six of these were excluded due to duplicate identifiers and five for not providing matching post-training responses. This resulted in a final sample size of 49 participants (MAGE=45.31, SD=10.20) of whom 41 identified as female and White British. Thirty-three were nurses, nine were midwives, three were higher education lecturers and four from other separate (and therefore, anonymised) healthcare roles. The majority of the sample reported that they had been in their profession for 15 years or more (61.2%), followed by 11–15 years (12.2%). Of this sample, 98% reported having completed ‘Equality & Diversity’ training at some point within their career.
Sensitivity power analyses were conducted in G*Power50 to assess the minimum effect size we could reliably detect with our final sample size across a range of statistical power levels. This indicated that for repeated measure analyses of pre- to post-training outcomes, we had 80% power to detect a moderate effect size of Cohen’s dz=0.41 and 90% statistical power to detect dz=0.47 with an alpha of 0.05.
Procedure
An email was sent to the senior management team within two NHS Trusts and a higher education institute requesting that staff sign-up to an URBT workshop. Participants signed up to 1 of 16 workshops, which were delivered online via Microsoft Teams due to the restrictions imposed by the COVID-19 pandemic. The workshops were developed and led by two individuals who identify as a Black British and White British female and limited to groups of 10 participants to encourage engagement and active discussion. Participants were informed that the learning objectives of the training were: (1) ‘To know: what unconscious bias is and how it impacts the people around us’, (2) ‘To be aware: of the barriers our own unconscious bias can create for the people around us’ and (3) ‘To do: commit to a change in practice’. Each training workshop was approximately 4 hours long and included seven main activities that focused on activating stereotypes, exploring the difference between unconscious and implicit bias, defining key terms (affinity bias, halo effect, in/out-groups, stereotypes, confirmation bias and group attribution), discussing the development of bias and reflecting on experiences of prejudice, harassment and discrimination (materials: https://osf.io/yfa6s/). After each activity, the trainers engaged in reflections, group discussions and question-and-answers. At the end of the training, participants were presented with key statistics regarding racial inequality from the NHS WRES34 and completed a quiz to reinforce their learning.
Primary outcome measures
The following measures were administered both pre- and post-training.
General training evaluation
We adapted a general evaluation questionnaire used in a previous training evaluation,51 which included 10 statements such as ‘I feel comfortable participating in this training’. Responses were recorded on a 5-point Likert scale (1=strongly disagree, 5=strongly agree) and resulted in acceptable internal reliability both pre- (Cronbach’s a=0.78) and post-training (a=0.87). A total score was calculated for each time point (range 10–50), with higher scores representing more positive evaluations of the training. After the questionnaire, participants completed open-ended questions that asked: ‘What did you find the most useful and why?’ and ‘How will you apply this training in practice?’.
Racial competency
Racial competency was measured using an adapted version of the cultural beliefs and self-efficacy subscale from the Cultural Competency Questionnaire.52 The term ‘culture’ was replaced to ask specifically about race. This questionnaire included six statements such as ‘students/staff may identify with more than one racial group’ recorded on a 5-point Likert scale (1=strongly disagree, 5=strongly agree). The questionnaire resulted in low internal reliability for pre-training responses due to the item ‘I am aware of the limits of my competency when interacting with students/staff who are a different race to me’. Removal of this item improved reliability for pre- responses (a=0.61) and was therefore removed for post- responses to allow direct comparison (a=0.64). A total score was calculated for each time point (range 5–25), with higher scores representing greater perceptions of racial competency.
Awareness of unconscious bias
Participants were asked ‘Have you ever heard of the term ‘unconscious bias’?’ and if they responded ‘yes’ were asked to define it. Perceived awareness and attitudes regarding unconscious bias were then measured using the Attitudes Towards Unconscious Bias Scale.51 This questionnaire included six statements such as ‘Mentors can have biases about students/staff of which they are unaware’ recorded on a 5-point Likert scale (1=strongly disagree, 5=strongly agree). The questionnaire resulted in acceptable internal reliability both pre-training (a=0.80) and post-training (a=0.82). A total score (range 6–30) was calculated for each time point, with higher scores representing greater awareness of unconscious bias.
Perceptions of bias
Perceptions of bias were measured using an adapted version of the General Perceptions of Bias scale.53 This questionnaire included eight statements with three subscales of personal bias (‘In most situations, I am objective in my decision making’), societal bias (‘People in today’s society tend to treat people of different social groups equally’) and healthcare bias (‘In healthcare practice, racial bias is no longer a problem in hiring decisions’). Responses were measured on a 6-point Likert scale (1=strongly disagree, 6=strongly agree), allowing for consistency with the other scales, and then reversed.52 The questionnaire resulted in acceptable internal reliability both pre- (a=0.86) and post-training (a=0.75). A total score (range 8–48) was calculated for each time point with higher scores representing greater perceptions of bias (ie, more ‘disagree’ responses).
Exploratory outcome measures
The following exploratory measure was administered post-training only.
Applications of training in practice
Approximately 1 month after the training, participants were sent a follow-up questionnaire that asked them to reflect on how they had applied the training in practice and were asked to return this within 3 weeks. This was registered as an exploratory outcome measure because we expected a relatively high attrition rate with the survey being distributed via email. First participants were asked: ‘Do you believe you have been successful in applying the training within your practice?’, responding either ‘yes’ or ‘no’. In line with52, they then responded to seven statements such as ‘since the UBT workshop I have reflected on how my biases may affect student/staff mentoring’ on a 5-point Likert scale (1=strongly disagree, 5=strongly agree). This questionnaire resulted in excellent internal reliability (a=0.92). Participants then responded to three open-ended questions that asked: ‘Since learning about unconscious bias, in what way do you think that this might influence your practice?’, ‘How have you applied the training in your practice?’ and ‘Have you had any difficulties/challenges in applying this training in your practice?’.
Analytical strategy
Analyses were conducted in SPSS (V.26).54 Missing questionnaire data were inputted using the mean for that particular questionnaire item (‘mean imputation’, <5% of cases).55 Confirmatory analyses assessed changes in general evaluations of URBT, as well as racial competency, awareness and perceptions of unconscious racial bias from pre- to post-training. These were each analysed using a repeated measures analysis of variance with an alpha level of 0.05 used to determine statistical significance. In line with previous research52, we report the percentage of agreement/disagreement with each statement for the general training evaluation and the applications of training in practice measures. Reflexive thematic analysis56 57 was employed to code responses to the open-ended questions and develop key themes. In this process, coding is recognised as a subjective process that requires a reflexive researcher who strives to reflect on their assumptions and how these might shape and delimit their coding. It includes the phases of familiarisation, coding, generating initial themes, reviewing and developing themes, refining, defining and naming.
Results
Primary outcomes
Evaluation
There was a significant increase in positive evaluations of URBT from pre- (M=38.71, SD=4.37) to post-training (M=47.08, SD=3.09), F (1, 48)=210.20, p<0.001, ηp2=0.81, dz=2.08. As can be seen in table 1, the training was evaluated positively, with the majority of participants responding ‘agree’ or ‘strongly agree’ to each item. In support of hypothesis 1, this suggests that the training increased understanding of unconscious racial bias and willingness to engage and promote the training.
Percentage of agreement/disagreement with each item of the training evaluation (post-training responses only)
Key themes from open-ended responses to the evaluation questionnaire
Four main themes were identified from the open-ended question ‘what did you find the most useful and why’: (1) reflections of unconscious racial bias; (2) lived experiences of discrimination, (3) a non-judgemental, open space and (4) prompting reflections of making a positive change. Three main themes were identified from the question ‘how will you apply this training in practice?’: (1) confronting racial bias; (2) enabling conversations about race and (3) enacting real change. Example excerpts are provided in table 2.
Racial competency
There was a significant increase in perceptions of racial competency from pre- (M=19.85, SD=2.14) to post-training (M=21.81, SD=2.17), F (1, 47)=37.63, p<0.001, ηp2=0.45, dz=0.88. In support of hypothesis 2, this suggests that the training encouraged participants to reflect on their beliefs around race and how these impact mentoring, supervision and interactions with racially minoritised students and staff.
Awareness of unconscious bias
There was a significant increase in awareness of unconscious bias from pre- to post-training: more participants reported that they recognised this term (MPRE=89.13%, SD=31.47, MPOST=100.00%, SD=0.00), F (1, 45)=5.49, p=0.02, np2=0.11, dz=0.35 and reported that they were more aware of its impact on staff and students (MPRE=25.00, SD=2.63, MPOST=27.65, SD=2.59), F (1, 47) = 40.60, p<0.001, ηp2=0.46, dz=0.92. In support of hypothesis 3, this suggests that the training increased overall awareness of unconscious bias.
Perceptions of bias
There was a significant increase in perceptions of bias from pre- (M=30.92, SD=7.69) to post-training (M=35.74, SD=5.23), F (1, 47)=29.27, p<0.001, ηp2=0.38, dz=0.78. In support of Hypothesis 4, this suggests that the training increased perceptions of personal, societal and professional bias and how they affect decision-making. Figure 1 displays the pre- and post- primary outcome measures.
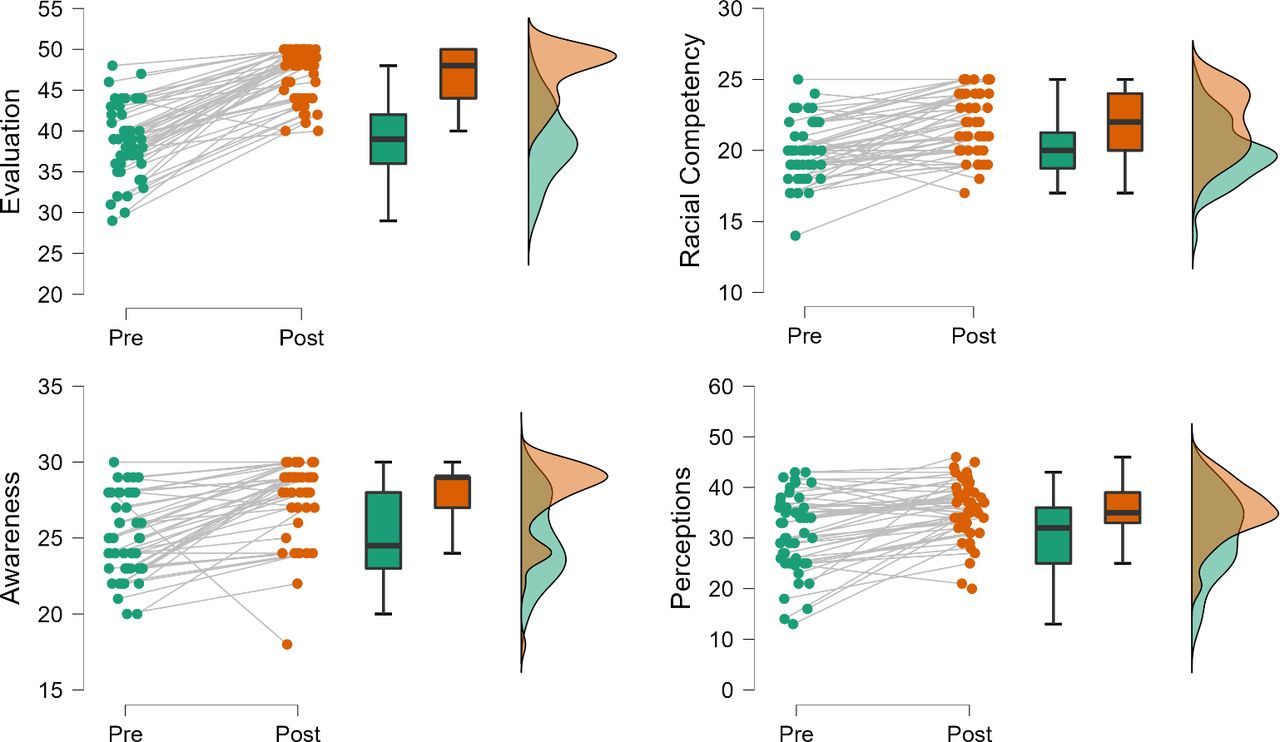
{kind=link}
A raincloud plot displaying pre- to post-training changes in training evaluations, racial competency, awareness and perceptions of unconscious racial bias. Left=individual data points from pre- to post-training, middle=IQR and CIs, right=data distribution.
Exploratory outcomes
After exclusion of duplicate or missing participant identifiers (n=9), a total of 17 participants were matched to the 1-month follow-up questionnaire. Of this sample, 76.5% responded ‘yes’ to the question ‘Do you believe you have been successful in applying the training within your practice?’. As can be seen in table 3, the majority of participants responded ‘agree’ or ‘strongly agree’ to six out of the seven questions; however, for the question ‘I have noticed a positive change in the way that students/staff respond to my mentoring’, the majority responded with ‘neither agree nor disagree’.
Four themes were identified from the open-ended questions ‘since learning about unconscious bias, in what way do you think that this may influence your practice?’ and ‘how have you applied the training in your practice?’. The themes identified were: (1) setting up mentoring and working groups, (2) changing the recruitment and progression process, (3), increased self-awareness and (4) diversifying the taught curriculum. Example excerpts are provided in table 4.
Percentage of agreement/disagreement with each item of the 1-month follow-up questionnaire
Key themes from open-ended responses to the ‘applications of training in practice’ questionnaire
Discussion
The degree awarding gap indicates that racially minoritised students receive lower degree classifications relative to their white peers, and this is coupled with experiences of racial prejudice and discrimination in higher education and the placement/practice environment. Research suggests that educator and practitioner attitudes and behaviour towards racially minoritised students are a significant contributing factor32 33 and should be a focus of racial equality initiatives. The current study evaluated the effectiveness of URBT delivered to NHS senior practitioners to enhance awareness of how racial inequalities negatively impact racially minoritised students. Findings indicate that participants reported overall positive evaluations of URBT and higher perceived racial competency, awareness of unconscious racial bias and perceptions of bias after the training. Qualitative responses suggest that participants had increased self-awareness and were exploring how to set up mentoring and working groups, change recruitment and progression processes, and diversify the taught curriculum. These findings suggest that URBT may be one effective strategy to increase knowledge, perceptions and awareness of racial bias in the higher education and healthcare practice environment and lead to a process of reflection and change.
Previous research has found mixed findings with regard to the effectiveness of UBT,42 46 and several recommendations have been put forth to improve it.46 47 Informed by these, we developed and evaluated an URBT workshop that was explicitly aimed at increasing understanding and awareness of racial bias, tailored to the healthcare setting, discussed the impact of prejudice and discrimination on racially minoritised students and staff, acknowledged feelings of discomfort and explored actions to mitigate bias. To assess (short-term) change, we also surveyed participants 1 month after the training to ask how they had implemented their learning in practice. These preliminary positive findings suggest that UBRT may be more effective when developed in line with these recommendations, and these should be considered in the development and implementation of future training interventions.
Participant’s qualitative responses provide further insight into useful aspects of the training, which can inform future training workshops. Two of the themes suggested that the training was useful because it facilitated reflections of unconscious bias and highlighted lived experiences of racial discrimination. The focus on the student narrative allowed participants to ‘consider their unconscious bias’ and ‘review how [their] values and beliefs might impact on practice’. A third theme suggested that the non-judgemental, open space was useful because it fostered ‘safe discussions around common misconceptions’ and allowed people to ‘explore issues and challenges’ and ‘talk freely about experiences’. This may have helped to overcome defensive reactions towards bias, which can occur as an unintended consequence of diversity initiatives.39 41 Finally, participants suggested that the training prompted reflections of making a positive change, such as ‘thinking about how to have conversations about race with staff in practice’ and ‘looking at the deficit model to implement change and overcome barriers with recruitment and development opportunities’. These excerpts support the notion that URBT should be action-oriented so that raised awareness of racial bias is coupled with strategies to mitigate it.47
Participants also responded positively when asked about how they would apply this training in practice, with three themes centring on confronting racial bias, enabling conversations about race, and enacting real change. However, it is important to note that these responses were gathered immediately after the training, so it is more informative to focus on responses to the 1-month follow-up questionnaire. Here, the majority of participants agreed that they had applied the knowledge learnt to their own practice, reflected on how their biases may affect student/staff mentoring, created new habits to explore unconscious biases, and been able to discuss race more confidently. They also strongly agreed that they had been aware of how their biases may impact student/staff mentoring and were able to share what they had learnt with other colleagues. Nevertheless, participants were also neutral with regard to noticing a positive change in the way that students/staff had responded to their mentoring. This may reflect the short follow-up period in which participants were asked this question, highlighting the need for continuous, long-term evaluations to ensure that URBT has its intended impact of negating racial inequalities.
At this stage, four themes were also identified which were setting up mentoring and working groups, changing the recruitment and progression process, increased self-awareness, and diversifying the taught curriculum. The first theme showed how participants were exploring how to ‘provide mentoring to our BAME staff to develop their leadership development’, ‘listening to other people’s views’ to implement change, and ‘setting up a focus group to […] support Black mothers’ and ‘engage with Black staff’. Within the second theme, participants expressed how the training had made them ‘think about recruitment processes’ and ‘challenging’ these to be more equitable. A general theme throughout these quotes was increased self-awareness of perceptions towards racially minoritised students and staff, for example, being ‘more aware of how what is said may have a cumulative effect on staff members’ and the impact of implicit behaviour such as ‘body language’ and ‘microaggressions’. The final theme indicated that the training had encouraged participants to diversify the taught curriculum, with excerpts focusing on ‘including sessions about race and bias in modules’ and ensuring that the ‘inclusion of bias [is] more explicit in lesson planning’, and the need to ‘actively explore the reasons for the attainment gap’. These themes are encouraging given that the training was targeted at staff in senior management roles who hold the power to make substantial changes in the NHS and higher education environment.
The main limitation of the current study is a common one in the literature on UBT: our outcome measures focused on the training’s usefulness, post-intervention knowledge and putative planned behaviours rather than actual behaviour change. Research has suggested that training effects can decay over time58 and longitudinal studies are therefore required to assess the sustained effectiveness of this training with more objective indicators (eg, changes in student attainment, staff retention, progression and disciplinary hearings). A recent study provides a gold-standard example of this, assessing whether a training workshop reduced racial microaggressions through simulated interracial patient encounters.59 As a positive early indicator of change, the current research has nevertheless informed the development of an anti-racism framework within one regional NHS Trust. This framework was co-produced with healthcare staff and focuses on six key principles of leadership, policy, transparency, well-being and belonging, employment, and education. It aims to provide a resource for management and individual staff members to facilitate individual accountability and monitor actions towards being an antiracist colleague and organisation. A longer-term evaluation of this framework is planned.
It is also important to note that, although the majority of qualitative responses were positive, some participant’s quotes revealed inherent racial biases within them, too. For example, when asked ‘since learning about unconscious bias, in what way do you think that this might influence your practice?’, one participant responded that one barrier was ‘when people of colour play the race card when they are being managed about their performance. People are not confident in how to challenge appropriately’. This language reveals inherent unconscious racial biases that may perpetuate racial inequalities by passing the blame onto racially minoritised students and staff themselves. When asked this same question, another participant responded that ‘I also think there is a risk that it may have a negative effect on my under[st]anding of different cultures as I am less likely to ask staff questions about differences in cultures in case this is perceived to be micro aggressions’. Although there were only a few instances of such responses, we include them here to highlight finer nuances around the effectiveness of URBT and the need for continued education to eradicate bias. Additional follow-up sessions after the training would be fruitful to explore such responses further and dismantle any misunderstandings.
Conclusions
The degree awarding gap between racially minoritised students and their white peers is well documented within UK universities and these students continue to experience racial prejudice and discrimination within the higher education and healthcare environment. The current study represents a coordinated effort between the NHS and higher education sector to evaluate the effectiveness of URBT to improve the experiences of racially minoritised students. Our findings indicate that such training may be a useful component of wider racial equality initiatives to increase knowledge, perceptions and awareness of racial bias and lead to a process of reflection and change. One-month later, qualitative themes suggest that participants had increased self-awareness of how they perceive and treat racially minoritised students and staff and were exploring how to set up mentoring and working groups, change recruitment and progression processes, and diversify the taught curriculum.
Although this study highlights the potential effectiveness of URBT, we emphasise that it is not a panacea. Instead, a multipronged approach is required that treats URBT as one element of a comprehensive and continually evaluated strategy to achieve racial equality. Effectively tackling the degree awarding gap requires a shift away from relying on a deficit model to explain differences between racially minoritised students and their white peers to greater critical awareness of the structural and institutional factors that perpetuate racism.1 32 Furthermore, open and honest conversations about racism are essential outside of URBT to ensure indefinite, positive change.27 Individuals, institutions and organisations must take an antiracist approach, demonstrating that they are actively combatting systemic inequalities and structural injustice.60 The NHS has outlined their commitment to addressing racial inequalities through the WRES report,14 NHS People Plan,15 and Race and Health Observatory.16 17 However, we argue that it is important that the degree awarding gap is also addressed within these strategies to ensure that racially minoritised students receive equitable education and placement experiences. This will allow the NHS to meet its goal of being a fully inclusive, equitable and fair employer.14
Data availability statement
Data are available in a public, open access repository. The design and analysis plan were preregistered via the AsPredicted.org template on the Open Science Framework (https://osf.io/5w8fc). All materials, anonymised data, and analysis syntax are publicly available, as well as a statement outlining any necessary deviations to the preregistration protocol (48; https://osf.io/yfa6s/).
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Research Ethics Committee at University of the West of England, REF: HAS.20.02.136. Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Twitter @drcpennington
Contributors This contributor statement was informed by the CRediT taxonomy (https://credit.niso.org/). Conceptualisation: CRP, EB and AA; Data curation: CRP; formal analysis; CRP: funding acquisition: CRP, EB, AA, MB and MPM; investigation: EB, AA; methodology: CRP; project administration: EE, AA, MB; resources: CRP, EB, AA; software: CRP, EB, AA; supervision: MB and MPM; validation: CRP and MPM; visualisation: CRP; writing—original draft: CRP; writing—review and editing: CRP, EB, AA, MB and MPM. Guarantor: CRP.
Funding The work was supported by a Health Education England (HEE) grant (reference: EHAS0025).
Disclaimer The funder had no role in the design and conduct of the study, the analyses, or their interpretation, nor the decision to prepare and submit the manuscript for publication.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note The term ‘Black, Asian and Minority Ethnic (BAME)’ is commonly used in research and society but is seen as problematic because it indiscriminately groups people from different geographical, behavioural, social, and cultural backgrounds (creating ‘othering’). For this reason, in this article we use the term ‘racially minoritised’ which represents people who are from the global majority but who have systemically been minoritised based on their race.