Article Text

Abstract
Introduction The mental health of children and young people in the UK has been declining and has continued to worsen throughout the pandemic, leading to an increase in mental health-related emergencies. In response, the Best for You programme was developed as a new service designed to integrate mental healthcare for children and young people between acute hospital and community services. The programme is comprised of four new services: a rapid assessment young people’s centre with dual-trained staff, a co-located day service offering family-based care,a digital hub, designed to integrate with the fourth element of the model, namely community support and mental health services. This evaluation protocol aims to assess the development, implementation and outcomes of the Best for You programme and develops a scalable model that could be implemented in other parts of the National Health Service (NHS).
Methods and analysis This mixed-methods realist evaluation aims to delineate the components of the system to assess their interdependent relationships within a wider context. Data collection will include interviews, participant observations, focus groups and the collection of local quantitative healthcare data. The research will be conducted across four phases. Phase 1—captures the development of the underlying programme theory. Phase 2—a process evaluation testing the programme theory. Phase 3— an outcome and economic evaluation. Phase 4—consolidation of learning from phases 1–3 to identify barriers, facilitators and wider contextual factors that have shaped implementation drawing on the Consolidated Framework for Implementation Research.
Ethics and dissemination Ethical approval for the evaluation was received from the NHS local ethics committee. Embedded within the evaluation is a formative review to feedback and share learning with stakeholders to scale-up the programme. Findings from this study will be disseminated in peer-reviewed journals as well as presentations to be useful to service user organisations and networks.
- MENTAL HEALTH
- Health policy
- Organisation of health services
- Paediatric A&E and ambulatory care
- Child & adolescent psychiatry
- Eating disorders
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- MENTAL HEALTH
- Health policy
- Organisation of health services
- Paediatric A&E and ambulatory care
- Child & adolescent psychiatry
- Eating disorders
STRENGTHS AND LIMITATIONS OF THIS STUDY
Protocol co-produced with clinical, managerial, academic, third sector and public stakeholders.
Uses a robust realist framework to develop initial programme theory and test its operability for evidence-building.
Connecting communities of practice to facilitate dissemination of learning, explore potential for scale-up and identify fixed and flexible implementation factors.
Plans to engage children and young people and their families in designing data collection methods.
Single-site study prevents direct prospective comparison of outcome data.
Introduction
The mental health of children and young people (CYP) in the UK has been declining and continued to worsen during the pandemic.1 Even before COVID-19, one in eight people under the age of 18 suffered from a clinically significant mental illness, equating to 112 000 individuals in London alone and representing a threefold increase in mental health-related (MHR) emergency department (ED) attendances.2 Consequently, the number of CYP admitted to paediatric wards primarily with a mental health condition has risen.3 Emergency hospitalisations for eating disorders or drug/alcohol intoxication significantly increased during the COVID-19 pandemic.4 The growing number of CYP seeking help from the ED has resulted in suboptimal, fragmented care as there are rarely the resources required to appropriately assess and treat this group of patients. This has led to poorer experiences and outcomes including long waiting times for referral to specialist psychiatric care, resulting in 13% returning to ED within a month.5 This is worrying, given the increasing mortality risk of MHR emergencies, such as eating disorders.6
Policymakers have acknowledged this problem and highlighted the need for greater integration of mental and physical healthcare for CYP within general acute paediatric settings.7 The NHS Long Term Plan prioritised CYP’s mental health, requesting significant improvements to the provision and access of care and early intervention for those with MHR emergencies.8 Evidence indicates that innovations for integrated acute care, such as embedding multidisciplinary assessment, early intervention and specialist psychiatric care significantly reduced the number, duration and repetition of emergency hospitalisations.9 Specifically, multidisciplinary teams (MDTs), psychoeducation and psychiatric telephone follow-up in ED reduced admissions up to 40%.10 Establishing a multidisciplinary unit for MHR emergencies reduced both the need for acute admission by 20% and the ED length of stay.11 Providing family-based therapy through partial hospitalisation reduced 1-year return admissions by 40%, which was the most clinically effective therapeutic modality.10 12 13 Thus, models of integrated acute care improve care coordination to treat both the physical symptom and the underlying mental disorder to prevent future emergencies and help a young person stay well.
The Best for You programme was developed in 2020/21 as a new service designed to integrate the mental healthcare for CYP within an acute hospital. The programme comprises four main components to better meet the needs of CYP and their families experiencing an MHR emergency: a rapid assessment young people’s centre based within an acute hospital staffed by dual trained (mental and physical health) clinicians that will receive direct admissions from the ED, with the aim of assessing and stabilising patients before referring to onward care; a day service that will cater for CYP requiring both psychiatric and medical care, such as eating disorders, to ensure an integrated approach between acute and community care for patients needing longer intensive step-down care; a digital hub that provides advice and support to CYP through apps and other digital interventions designed and evaluated to support and treat mental disorders in CYP; and a community partnership programme to support CYP and their families in non-clinical settings. These services are further supported by a range of programmes and activities including an MDT and a novel staffing approach, and an education and training programme. Each component of Best for You was developed through a review of existing services conducted by all programme stakeholders, which led to the development of financial and clinical proposals. The proposals included analysis of current staffing and service capacity, and a review of best practices to identify service reconfigurations targeted at improving the comprehensiveness of services to better meet the needs of CYP and their families.
Collectively, Best for You can be understood as a complex intervention, as outlined by Craig et al,14 due to several features.14 These include several interacting components, the need for organisational and procedural changes across multiple components of the system of care, the need for changes in behaviour by those delivering or receiving the interventions; the breadth of groups and organisations targeted by different elements of the programme and a diversity of outcomes that the programme intends to achieve. Despite this complexity, the overall aim of the programme is simply to better meet the needs of CYP and their families experiencing an MHR emergency by integrating specialist psychiatric care within an acute hospital.
While evidence exists for each component of the Best for You programme from comparable international examples, the proposed evaluation aims to assess the development, implementation and effectiveness of the different components both individually and collectively.9 This mixed-methods evaluation draws on both the complex systems literature and realist evaluation methods and theories to understand how complex, multi-layered service improvements can be evaluated.14–17 This approach recognises the complexities of interventions which achieve their outcomes via social, medical, organisational and interpersonal mechanisms that by their very nature may be non-linear, emergent and unpredictable and also that these effects may manifest differently for different cohorts of patients and their families. Complex interventions rely on a level of flexibility and adaptability to ensure responsiveness to the wider system of components, which may in turn, reduce the level of certainty of the intended outcomes.18 The evaluation is further centred around understanding and documenting the iterative nature of programme theory and service implementation. The initial programme theory (IPT) documents and explains how the proposed interventions intend to achieve their outcomes through the causal mechanisms within its wider context, which is an explicit purpose of realist evaluations.19 The use of a realist approach to evaluation is especially useful when the intervention under study is large, multifaceted and complex and will elicit the underpinning context, mechanism and outcomes (CMO) configuration.18 This seeks to explain what mechanisms are used to what effect, and alongside which contextual challenges and enablers. This is relevant due to the multiple components of Best for You that seek to improve multiple outcomes within an existing service.
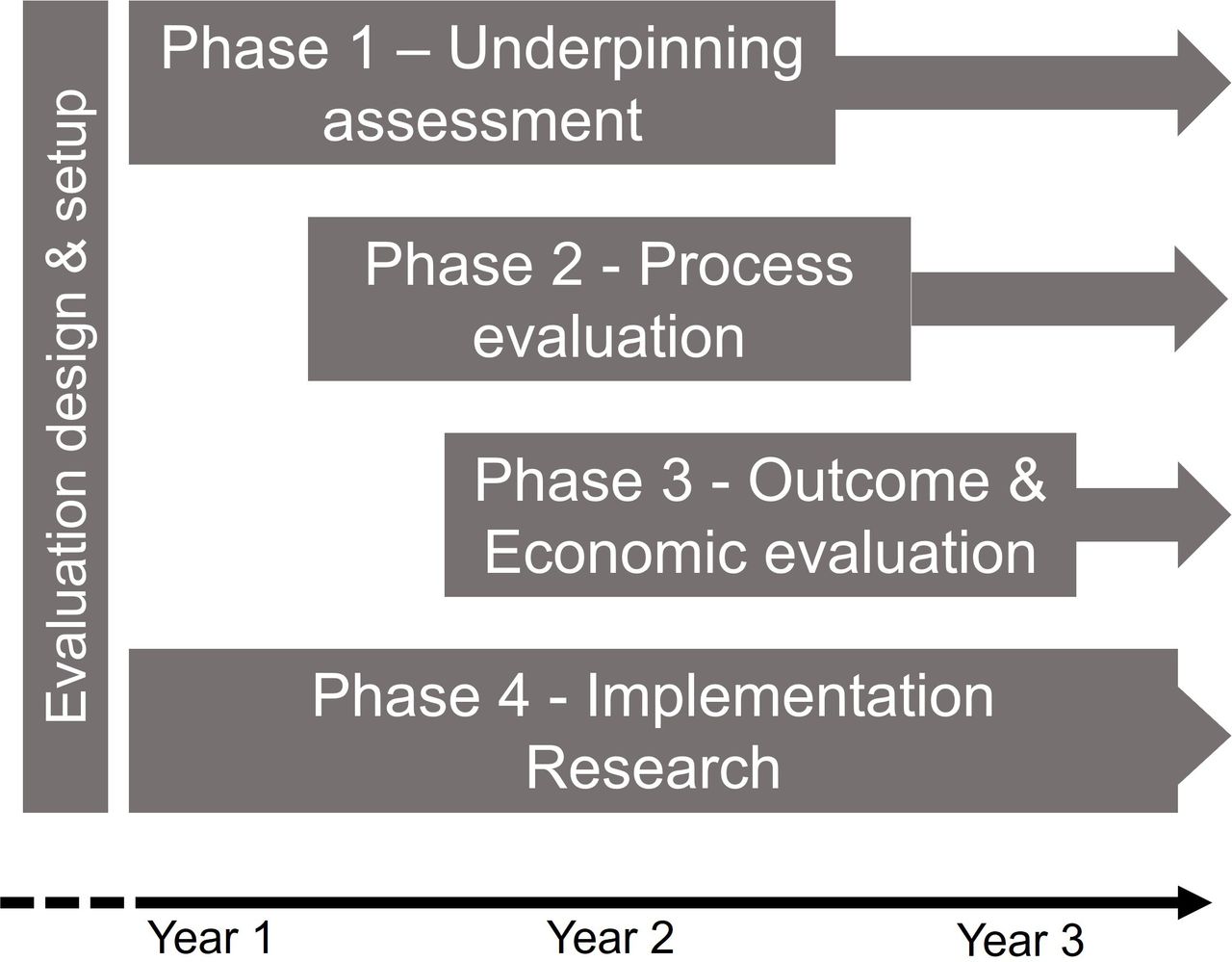
The evaluation design includes four overlapping phases (figure 1). The primary objective of phase 1 is to identify the nature and scope of the problem, where it is located, whom it affects and how. Through the development of the IPT, individual interventions/strategies that comprise the programme will be iteratively revised in the light of evidence from data collected during implementation. Phase 2 will compare how the service delivery corresponds to the vision of the programme team and to the IPT and identify if there are areas of underimplementation through a process evaluation. Phase 3 will assess the effect of the programme on patient level and service level outcomes through an economic and outcome evaluation. Finally, phase 4, which runs throughout the duration of the programme, will identify the barriers and facilitators related to the interventions and context that influence the implementation and attainment of the outcomes.

Phase 1: develop an understanding of the current problem from multiple perspectives drawing on participatory methods such as stakeholder analysis and process mapping; phase 2: assess the implementation of the programme and delivery of services to patients using qualitative and quantitative approaches; phase 3: analysis of programme outcome data to quantify impact and costs and critically analyse effectiveness /cost-effectiveness to ascertain value for money; phase 4: identify barriers and facilitators encountered in implementation and the role of wider contextual factors in shaping implementation using analytical frameworks.
Methods
Study design
The complexity of the evaluation reflects the complexity of the organisational, clinical and research context in which the evaluation will be conducted. Multiple organisations, including NHS Trusts, are responsible for the planning, co-ordination and delivery of services, some of which overlap between the different programme components, requiring an adaptable but comprehensive evaluation drawing on multiple research frameworks.
This mixed-methods realist evaluation draws on a complex systems approach set within an implementation science framework. The first step was to co-produce the IPT with the Best for You programme team. The development of the IPT was undertaken in consultation with the Best for You programme team and through a review of the programme documents.19 Co-producing the IPT provided an opportunity for the programme team to clarify and refine their thinking around the components of the programme and allowed the research team to capture and articulate the shared aim and key elements of the programme (figure 2), while building relationships with the programme team. The IPT outlines the interventions that comprise Best for You and how each is expected affect patient outcomes, through what mechanism, and their contextual circumstances. This diagrammatic representation of the IPT guides our approach to the overall evaluation of the programme, with the data collection split among the different service delivery interventions, following their implementation via different subteams. This will allow the research team to note any variations during the programme implementation, discuss the reasons for this with the team and assess their understanding of the impact of the variations on the programme. These insights will be particularly relevant in shaping the planned formative reviews, which will also facilitate discussion and provide opportunities to collect data from the programme team.

{kind=link}
{kind=link}
Best for You Initial Programme Theory: diagrammatic representation of the overall initial programme theory (IPT) for the Best for You programme that links the overall aim of the programme to the six main programme interventions by outlining the main contributing factors and causal mechanisms. CYP, children and young people; CAMHS, child and adolescent mental health services; ED, emergency department; MDT, multidisciplinary team.
As an observational study, there are recognised limitations to the types of evaluations that are appropriate for the different programme components. As such, the study includes several distinct parallel evaluations: a process evaluation, outcome evaluation and economic evaluation nested within the Consolidated Framework for Implementation Research (CFIR). CFIR provides the overarching framework for the research methodology that will inform the data collection and analysis.20 The CFIR domains and subdomains form the basis of the topic guide for interviews and the observational framework for the participant observation.
Description of the Best for You programme (interventions)
The Best for You programme is composed of four main interventions:
Young People’s Centre: A bespoke 8–10 bed unit based within an acute hospital that will provide a dedicated space for the treatment and rapid assessment of CYP between the ages of 13 and 17 years who are admitted to hospital via the ED due to an MHR emergency. A typical patient admitted to the unit for 72 hours would receive a thorough multidisciplinary assessment by dual-trained (mental and physical health) clinicians.
A day service: A multipurpose environment designed to provide a social and therapeutic area to support a small number of CYP during the day. Therapeutic services focused on eating disorders and other related problems that require both medical and therapeutic care will support CYP and their families to become more independent and offer group and family sessions and holistic therapy classes. Out of hours, the space will be utilised as a drop-in that will integrate with the provision of a community partner programmes staffed by skilled volunteers and social prescribers. This will provide a space for low-level intensity care and signposting to appropriate community services.
A digital hub: An online web portal that curates a range of evidence-based apps that aim to support CYP with their mental health. These range from ‘crisis’ support, for example, ‘Shout’, to online psychological interventions, for example, ‘Kooth’. Access to the Digital Hub, which was launched in 2021, is promoted through various events and platforms including user-generated platforms, for example, Tik Tok and YouTube or via ‘Digital Prescribers’ who will be trained and deployed to introduce digital aids to CYP and their families. The intention is to provide a single portal for validated clinical support and information for CYP and their families, with links to local organisations offering nearby support. This workstream integrates into associated community outreach projects to ensure maximum reach and adoption of new digital aids and will support the integration of the Young Peoples Centre and day service into current mental health services that are offered to CYP.
A community partnership programme: A network of local mental health partners, which currently include Chelsea Football Club, the Royal Borough of Kensington and Chelsea (RBKC) and several specialist voluntary organisations. It will also build on current community programmes to hold classes for CYP in their communities and guide them and their families to the appropriate organisations that can offer help outside of traditional NHS settings.
Throughout the four core interventions, an MDT and novel staffing approach will aim to support the redesign of the current model of care for CYP in MHR emergency bringing together paediatric, specialist mental health staff at the point of admission to deliver a targeted and tailored intervention as quickly as possible. The project will work with patients and families to help design a staffing and engagement model for the proposed rapid assessment young people’s centre and day service, including the recruitment of specialist volunteers, youth workers, young peer-to-peer advisors and social prescribing link workers who can offer non-clinical advice and guidance to families and carers. Finally, the education and training programme will allow staff across NWL and the UK to access placements and training opportunities in the new integrated model of care provided by the partner organisations. This could include rotations, short-term secondments, training fellowships and clinical innovation and research placements within the programme team. The team are exploring the opportunity to introduce a new specialist nursing role as part of the staffing infrastructure of the Young Peoples Centre. This work will be extremely important in providing the evidence to encourage scale-up the Best for You model in other parts of the UK.
Data collection
Data will be collected through multiple methods including documents, participant observation, semi-structured interviews, focus group discussions, stakeholder mapping, process mapping, questionnaires and routine clinical and administrative data from the healthcare providers involved. These methods allow for the continuous collection of data through the development and implementation of the programme that will enable the research team to identify the challenges and barriers, along with strategies that were used to overcome these, at different stages of the programme. Furthermore, these methods will allow the research team to capture the views and opinions of staff, volunteers, patients, service users and parents/carers about the new service. Participatory methods, such as stakeholder and process mapping, will be used to engage the programme team and front-line healthcare professionals and where possible, patients and their families, to understand their perspectives of care use and delivery. Parents or carers will receive either the Brief Parental Self Efficacy Scale (BPSES) or Parents vs Anorexia’ scale (PVA) questionnaires at both the start of the intervention and at the end.21 22 Before–after treatment effects for patients will be assessed through routinely collected questionnaires to assess clinically relevant mental disorder. Finally, the collection of quantitative data, which will include hospital administrative data such as admissions/readmissions and length of stay, will allow the research team to assess the effectiveness of the programme and identify changes in activity that may be crucial in developing the evidence to support scale-up of the programme in other locations. Data analysis using quantitative and qualitative sources will support the refinement of the programme theory and demonstrate where evidence is generated to support possible causal links between the interventions and the outcomes through plausible mechanisms.
Data collection is limited to one site (comprising three trusts and several third sector organisations). The use of various conceptual and analytical frameworks along with the triangulation of the data will help to ensure that the analysis is robust and makes findings generalisable to ensure their use to those who engage in adopting and adapting the model to additional settings outside of the initial implementation site. Furthermore, the research team will engage in reflexive discussions about the data prior to more formal analysis.
Sampling
A theoretical sampling matrix has been developed with three axes of diversity to account for a range of views that might be expressed by different participants. This will be used to guide recruitment of different stakeholder groups for interviews and focus group discussions. The sampling matrix demonstrates the range of key informants that will be engaged to ensure a variety of perspectives and views (table 1). The first axis relates to the location of the organisation in relation to the programme, that is, those directly involved in the development and implementation of the Best for You programme and external stakeholders within other organisations that currently provide services for CYP with an MHR emergency in northwest London. The second accounts for the different locations of informants in the pathway, that is, whether they provide services or receive services in the acute setting or the community. Again, the rationale is that those in the acute services may have different views and opinions compared with those in community services. The third axis relates to the different roles/positions informants have within the organisations or programme. Those at a senior level within the organisations but not directly involved in the programme, those responsible for the implementation of the programme, those involved in delivering services as part of the programme and those receiving services or their families and carers.
Theoretical sampling framework outlining the three axes of diversity (programme/setting/ role) that generate 12 different participant groups
Recruitment
Service users, patients and their parents/carers will be recruited via posters displayed at the clinical sites. Once they contact the research team, they will be provided with a summary of the purpose of the evaluation and a participant information sheet. A follow-up call will be scheduled to allow the potential participant to review the material and address any questions raised. If the participant agrees to participate, either an interview or focus group will be scheduled according to their preferences. Those under 16 years will be required to have parental or guardian consent and will be offered to have a parent or guardian present during the interview or focus group discussion. Participation will be voluntary and service users not wishing to take part in the evaluation will still receive the healthcare on offer to them.
The recruitment process will be continuously monitored to ensure recruitment across all participant groups.
Service providers including clinicians and managers will be recruited from the study sites via direct email from members of the research team. An information sheet will be provided on invitation to participate. Recruitment will occur systematically, until sampling quotas have been achieved.
The number of participants that will be included in the qualitative data collection with regard to the interviews and focus group discussions are: 60 staff or volunteers that make up groups 1–6 and 9–12; 40 patients/service users and 40 parents/carers that together make up groups 7 and 8. Approximately 100 responses to the questionnaire would be expected from parents/carers.
Quantitative data includes hospital data, routinely recorded by NHS Trusts and input to an integrated database comprising pre-consented patient data from primary, secondary and tertiary care across northwest London, known as Whole Systems Integrated Care (WSIC) database. WSIC is hosted and governed by Imperial College Health Partners, who provide deidentified data access for research through a secure server titled Discover Now. We will select the patient cohort who present at the ED with MHR emergencies and are admitted for emergency treatment; approximately 250 CYP per year.
Data analysis
Data analysis will be conducted in four phases. Data analysed within phase 1 will specifically focus on the participant observation (of the programme team), focus group discussions and process mapping. The analysis will aim to generate a narrative of the programme development identifying key milestones and capturing the development of the underlying programme theory and the assumptions about the mechanisms of action of the interventions. This phase will also aim to elucidate the ‘problem’ as understood from an organisational perspective and clarify the rationale and motivations for the approach taken.
Data analysed in phase 2 will include quantitative data generated by the clinical services as well as qualitative interview data. Analysis of these data will test the programme theory and assess delivery of the service as intended by the programme team. In phase 2, descriptive statistical analyses will be used to characterise the cohort of people who use the services within the programme, to examine clinical and sociodemographic characteristics as potential individual mechanisms of impact. The qualitative interview data will be analysed using template analysis—a type of thematic analysis, which is guided by an a priori set of themes under a pre-existing template. The template will use the Context Mechanisms Outcome (CMO) framework developed iteratively in phase 1, to test the IPT. Within this phase, we will triangulate analysis of qualitative data from our observations, documentation, focus groups and interviews, as well as quantitative hospital data. This will allow us to describe the specific context of the clinical interventions, assess the outcomes achieved and propose the mechanisms by which these occurred.
Phase 3 will include an outcome and economic evaluation to assess the effect of the programme on patient-level and service-level outcomes using hospital service data. Descriptive analyses will report on service provision both pre-delivery and post-delivery of each programme component. This will report on the number care packages delivered at each component (ie, young people’s centre, day service, digital hub), number of patient transfers between programme components, length of stay (average and proportion within the maximum target threshold) and service expenditure.
Statistical analyses will evaluate the effect of the programme components on the outcomes of interest, using an interrupted time series analysis as the programme components are delivered in sequence. This will consist of at least three time points both pre-delivery and post-delivery of each component. The outcomes are service performance data including ED visits, emergency admissions in the young people’s centre, emergency paediatric admissions, readmissions within a year and annual expenditure. Individual attributes will be considered as covariates, including clinical service history, diagnosis, deprivation index (by postcode), age and gender. This will explain differences in programme effectiveness and service provision in the cohort. Propensity score matching will be performed to improve comparability of pre–post intervention effects if the patient-level data permit. Analysis of before–after treatment questionnaires for the day service participants will be analysed using repeated measures analysis of variance tests.
Phase 4, which runs throughout the duration of the study, will integrate the analysis from the other three phases. The CFIR framework will serve as an analytical framework to identify barriers, facilitators and the wider contextual factors that shape the implementation of the programme.20 The analysis will draw on data collected in phases 1–3 and will consider:
Intervention characteristics—such as the evidence strength and quality, the extent to which the service is adaptable, the quality of the design of the programme and the relational integration between the different aspects of the service which was designed to deliver holistic care;
The outer setting—which includes factors such as patient needs and resources, external policies and incentives;
The inner setting—which includes factors such as the implementation climate, factors influencing change, how ready the pre-existing services and service providers were to change, and the context of the changes made;
Characteristics of individuals—taking in factors such as knowledge and beliefs about the intervention, how legitimate the change was perceived to be, how well integrated in the service staff felt, and their roles were in the overall reconfiguration of the service;
The processes involved in the programme delivery—including factors such as planning, engagement of stakeholders, the execution of the new service delivery plan, evidence of reflection and evaluating during the programme delivery, the skillset of those charged with delivering the service and the opportunities that were available to appraise progress and influence service change.
The findings from this analysis will also inform the basis of the proposed model for scale-up, outlining the different components of the interventions and the potential challenges and barriers to their implementation along with potential strategies for mitigating these challenges.
Patient and public involvement
The research team includes two public partners with varied and relevant backgrounds and experiences. JS is a former specialist teacher of vulnerable pupils and was seconded to Child and Adolescent Mental Health Services (CAMHS). She is a public partner on several national research projects to do with hearing loss, has experience of improving hearing care for care home residents and writes a column for a hearing loss magazine. MK has 30 years’ experience as a Healthcare and Well-being trainer and therapist, specialising in Stress Management and over 20 years as a GP Surgery PPG Representative. She is an Associate Member of the Young Harrow Foundation, an MHFA Youth Mental Health First Aider and a Dementia Care Friend. She has lived experience of multimorbidity and anxiety and depression and is a carer for elderly, extremely vulnerable parents with complex health needs.
Public partners have contributed to refining the research questions and reviewed the lay research summary, consent forms, participant information sheets and designed the recruitment posters. As co-investigators in the study, they will continue to be involved in developing the research and will actively contribute to the data collection and analysis.
Future involvement of a wider range of people with lived experience, including CYP and their carers, will be co-ordinated by the research team, the NHS Trusts and charity involved in the programme. Planned activities include the co-production of interview and FG topic guides with CYP. Preliminary findings from the study will be shared with PPI groups to inform the interpretation and analysis of data and help to identify areas where further investigation may be needed. The development of relationships with key PPI groups expects to generate new opportunities to engage a wider range of service users, families and carers engaged with Best for You interventions, to co-design future research if the programme is scaled-up, as planned. Furthermore, the involvement of CYP and their families in the co-design of the Best for You programme has been explicit in all aspects of the service development through a consultation process. The evaluation will assess patient and public involvement, whom have been consulted on co-designing the new service, as an intrinsic part of the implementation research.
Ethics and dissemination
Ethics
Ethical approval for the evaluation was received from the North West—Greater Manchester Central Research Ethics Committee (REC reference number: 22/NW/0116). Research and Development approval has been gained from three different participating NHS Trusts: an acute Trust and two mental health provider Trusts. The study will be conducted adhering to relevant ethical and legal institutional and organisational guidelines and policies that cover issues of research governance such as informed consent, confidentiality and the storage of personal data.
Each set of observations, interviews and/or questionnaires may include participant-identifiable data. This will be stored on a secure password-protected drive, with access restricted to researchers within the research team who do not have close working relationships (defined as direct line management, sharing work responsibilities) with any of the participants. Personal data (consent forms and non-anonymised data) will be stored in a locked cabinet and destroyed 10 years after completion of the study. Research data (non-identifiable) including transcripts and audio recordings will be destroyed 10 years after completion of the study.
Dissemination
This protocol outlines an evaluation that will assess the planning and implementation of the Best for You model and dissemination of the learning from it. The planning and implementation of the service model will be studied in a single inner London borough. In addition, stakeholders from other NHS organisations interested in adopting or adapting the model will be engaged by the research team to share learning and consider the suitability of the model for scaling up outside of the inner London setting and context. Learning events will be timed to share learning throughout the course of the new service implementation. The focus of the events will be on the three phases of the research: (1) planning and programme theory development; (2) lessons learnt from the implementation process, context and outcomes; (3) adopting and adapting the model to additional geophysical and organisational contexts. This approach builds on evidence for successful collaborative networking and knowledge mobilisation.23 T. The learning events will be organised to enable attendees from the inner London borough and from other NHS organisations to share their experience of testing service models in different contexts. This local experience-based knowledge will be utilised to support implementation and encourage collaborative working and ‘communities of practice’.24–26 Within these communities of practice, people will ‘share their experiences and knowledge … to foster new approaches to problem-solving and improvement, help drive strategy, transfer best practice, develop professional skills …’19
Findings from this study will also be disseminated in peer-reviewed journals and presented to relevant stakeholders and conferences, including in formats likely to be useful to service user organisations and networks.
Evaluation steering group
This research has been shaped through a dedicated steering group comprised of clinical academics from a range of disciplines—child psychiatry, paediatrics and primary care and researchers with backgrounds in evaluation, economics, public health, mental health, digital health innovation, implementation and improvement science. Public partners have previous working experience in children’s and adult mental health services as well as improvement work. The steering group have contributed to the development of the study design and continue to play a role in monitoring the study and ensuring that milestones are reached, ensuring the research is conducted according to the ethical and legal responsibilities that have been set out. Draft and final versions of the evaluation protocol were shared with the programme team, who agreed the approach and its content. It is intended that a participatory approach to evaluation will develop as working partnerships are further utilised between service providers and the research teams progress.
Conclusions
There is an urgent need to develop new models of care to address the fragmented and uncoordinated care for CYP experiencing MHR emergencies. Best for You is a novel multi-component model that has been co-designed with clinicians, managers, CYP and their parents and carers to deliver care that aims to integrate specialist mental healthcare within an acute paediatric setting. Through a mixed-methods evaluation that draws on a complex system approach, this research aims to identify and assess the various components that make-up this new model of care within the wider context of the healthcare system. Through this process, a proposed service model will be generated and learning about the barriers and facilitators to implementation that can support scale-up will be shared with policy makers, clinicians and health service commissioners.
Ethics statements
Patient consent for publication
Footnotes
Contributors MO, SB and SGH contributed equally to this paper. MO, SB and SGH led the design of the study with input and guidance from MK, JS, DSH, BH, NA, LL and DN. SGH, MO and SB produced the draft manuscript and MK, JS, DSH, BH, NA, LL and DN contributed to the manuscript. All authors read and approved the final manuscript. DN is the guarantor for this research.
Funding The National Institute for Health and Care Research Applied Research Collaboration Northwest London and the CW+ charity funded the evaluation.
Disclaimer This articlepresents independent research commissioned by the National Institute for Healthand Care Research (NIHR) under the Applied Health Research (ARC) programme forNorthwest London. The views expressed in this publication are those of theauthor(s) and not necessarily those of the NHS, the NIHR or theDepartment of Health and Social Care.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.