Article Text

Abstract
Objectives To explore factors associated with care burden and the self-described positive aspects of caring for a person living with amyotrophic lateral sclerosis (ALS) over time.
Design Exploratory longitudinal mixed-methods study.
Setting A national multidisciplinary tertiary clinic in Dublin, Ireland.
Participants Participants were informal caregivers of people living with ALS (plwALS) attending the national ALS/motor neuron disease Clinic Dublin. This study focuses on informal caregivers who completed five consecutive interviews (n = 17) as part of a larger multisite study, over the course of 2.5 years. Participants were over the age of 18. Formal paid caregivers were not included.
Outcome measures Data were collected on demographic and well-being measures and an open-ended question asked about positive aspects of caregiving. Relevant statistical analysis was carried out on quantitative data and qualitative data were analysed thematically.
Results The caregivers in this study were predominantly female and spouse/partners of the plwALS. Hours of care provided and self-assessed burden increased substantially over time, psychological distress reached clinical significance and quality of life remained relatively stable. Positive aspects identified were thematised as meaning in life and personal satisfaction and varied in relative frequency across phases of the caregiving trajectory.
Conclusions The co-occurrence of negative and positive factors influences the experiences of informal caregivers in ALS. It is important to explore and acknowledge positive aspects, how they develop and are sustained in order to inform supportive services. The cyclical adaptation identified in this study provides evidence for time sensitive targeted supports.
- motor neurone disease
- qualitative research
- neurology
- psychiatry
- mental health
Data availability statement
Data are available on reasonable request. The data presented in this study are available on reasonable individual request from Mark Heverin Research Manager in the Academic Unit of Neurology in Trinity College Dublin.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
While evidencing negative factors, this study has detailed positive factors identified by the caregivers themselves.
The mixed-methods study design provides standard outcome measures and self-identified positive factors to better understand the caregiver experience.
The study followed the same people over the course of 2.5 years, which represents the majority of an average disease trajectory.
Seventeen caregivers completed five consecutive interviews; the findings cannot be generalised to all caregivers of people with amyotrophic lateral sclerosis.
This study did not include details of the cognitive and behavioural impairments, disease status of the care recipient and the influence of these on the caregiver experience.
Introduction
Amyotrophic lateral sclerosis (ALS), also known as motor neuron disease (MND), is a progressive neurodegenerative disease, which causes paralysis of limb, respiratory and bulbar muscles, cognitive and behavioural decline (e.g., impaired executive functioning and behavioural changes) and may be accompanied by frontotemporal dementia.1 No cure has yet been found for this condition, treatment is in a palliative capacity and for the majority of people living with ALS (PlwALS), death occurs within 3 years of symptom onset.2 3 Due to the debilitating nature of the disease, there is an increasing need for care, a major role in the care process is provided by informal caregivers.4 The management of ALS often takes place in the home and focuses on maximising quality of life for PlwALS.5 Informal caregivers have a central role in the care of PlwALS particularly because their involvement allows the PlwALS to stay in their own home.4 6 The majority of informal caregivers in ALS are family members.7 Caring for a PlwALS has been shown to impact the caregiver’s quality of life and is a significant source of burden and psychological distress increasing over time.8–10 Phases in ALS caregiving have been reported—early coping and adjustment, maintenance and transition to the terminal stage through to bereavement.11–15 Phases are demarcated by key transitions experienced when the illness progression manifestly challenges.13
High levels of burden have been found in informal caregivers of PlwALS.6 10 16 Patient-specific factors such as disease severity, apathy, disinhibition and executive dysfunction17 have been shown to contribute to levels of burden.18 Having a lack of sufficient information and training has also been reported to contribute to burden.19–21 Most caregivers will experience psychological and physical distress in response to the strain caused by having a family member receive a diagnosis of an incurable disease, such as ALS.22 Caregiver characteristics such as resilience, coping style, problem-solving skills, use of social supports and other psychological-emotional factors impact burden.16 18 20 23–25
Caregiver burden and difficulties may be moderated and balanced by positive aspects of the caregiving situation,7 Positive experiences coexist with distress, and individual psychological factors may shield the individual against higher levels of burden.26–29 Personal satisfaction has been identified as being a protective factor in caregiving, including having enough time to care for oneself and having a life outside of caregiving.29 Meaning in life has also been identified as a protective factor for the caregiving experience.30 One study found that finding meaning in the caregiver role protected against depression and strain due to the role of caregiving.31 Finding positive meaning32 33 and having a sense of hope34 may increase quality of life and decrease perceived caregiver burden in informal MND caregivers.
Psychological appraisals, such as optimism, perceived autonomy, sense of purpose, resilience and perceived levels of social inclusion, have been shown to positively impact caregiver wellbeing.35 Psychological flexibility, mindfulness and meditation have also been shown to contribute to a more positive caregiver experience.14 15 36 37 As such, we believe it is important to identify positive factors derived from caregiving, which may protect against elevated levels of burden and distress in this cohort, and ultimately better inform caregiver supports and interventions.
There are a lack of longitudinal mixed-methods analyses in the research literature regarding positive and negative aspects of caregiving in ALS. The aim of this study was to explore factors associated with care burden and the self-described positive aspects of caring for a PlwALS. The mixed-methods longitudinal study design provides a unique opportunity to follow a group of informal caregivers over the course of approximately 2 years and a substantial proportion of the ALS disease trajectory.
Methods
Study design
Irish caregiver data were collected as part of a European multicentre study (ALSCarE) from 2015 to 2019.38 Prospective participants were identified by the PlwALS as their primary informal caregiver. Primary informal caregivers are defined as those who previously or currently provide the majority of support and assistance to a PlwALS at any disease stage, without financial compensation.39 Up to five in-person one-to-one in-home semistructured interviews were undertaken by either a male or a female research assistant psychologist attached to the National ALS/MND Centre in Dublin. This longitudinal qualitative dominant mixed-methods study explored the characteristics of caregivers who completed all five interviews.
Participants
Participants were aged over 18 years of age; a primary informal caregiver of a PlwALS attending the National ALS/MND Centre in Beaumont Hospital Dublin; and who completed five consecutive interviews over 2.5 years. Written informed consent was obtained from all participants.
Seventy-three caregivers completed at least one interview (seventy at baseline) and 17 caregivers completed five consecutive interviews over the course of 12–28 months (figure 1). The latter cohort is the focus of this analysis. Data from all caregivers at baseline are presented for comparative purposes as relevant.

Flowchart outlining the number of participants at each interview time point and the approximate time between interviews. a = mean months between interviews.
Procedures
Demographic data were collected and standardised measures assessed established well-being characteristics over time, for example, levels of burden (Zarit Burden Inventory, ZBI), psychological distress (Hospital Anxiety and Depression Scale, HADS) and quality of life (Quality of Life in Life Threatening Illness-Family Carer Version 2, QOLLTI-F) (see online supplemental appendix A).
Supplemental material
In an open question during each interview, participants were asked: ‘For you, what are the good things about caregiving?’. Unstructured text responses were recorded on paper by the interviewer, and later uploaded into a Microsoft Excel database. Quantitative and qualitative data were collected at baseline and on a possible four further occasions, thus five interviews completed the interview series.
Data analysis
Quantitative analysis
Demographic and assessment data were analysed using statistical tests, for example, t-tests and Mann-Whitney U tests as relevant to compare means and χ2 tests of association as relevant, using IBM SPSS V.26.40
Qualitative analysis
Qualitative data were analysed using the codebook approach, part of a tripartite typology of thematic analysis.41 The authors familiarised themselves with the text responses through reading and rereading across the dataset. A coding frame was developed from initial in vivo coding, which was refined and amended as the coding progressed. Coding was carried out until data saturation was reached. Three coders worked independently and met to discuss similarities and differences, before reaching consensus. Themes were derived from the data.
Patient and public involvement
None.
Results
Characteristics of the 73 caregivers who participated in interviews (at least one) are described in online supplemental appendix B.
At the first interview, hours of care provided per week was the only measure that was statistically significantly different (p = .007) between those who took part in at least one and those caregivers who completed all five interviews consecutively. Hours of care provided was not significantly different at any other time point.
Characteristics of caregivers who completed five consecutive interviews (n = 17)
These caregivers were predominantly female (76.5%), spouse or partner (S/P) of the PlwALS (82.4%) and living with the PlwALS (94.1%). There were three daughters among the cohort. The mean age was 57 years, ranging from 32 to 82 years. Hours of care provided per week increased from a median of 1 to 89.5 hours from interview 1 to interview 5.
The mean burden score increased from 12 to 22 (ZBI) across the interview series. The clinical cut-off score for ‘high burden’ is ≥24,42 and 27% of caregivers reached this score at some stage over the course of the five interviews.
The mean level of psychological distress score (HADS-T) increased. The clinical cut-off score for ‘probable psychological distress’ is ≥12.43 Among the cohort, 35% of caregivers reached this level of psychological distress at some stage over the course of the interviews.
The quality-of-life mean score (QOLLTI-F) remained stable over time (7.3–7.36 from first to last interview). Well-being characteristics are presented in figure 2 and online supplemental appendix C.

Outcome measures (well-being characteristics) over time (n = 17).
The PlwALS for whom care was provided were mainly spinal onset disease, at various stages of disease progression (according to Kings staging44 45 and in terms of cognitive functioning, (Edinburgh Cognitive and Behavioural ALS Screen, ECAS)46 and behavioural status (Beaumont Behavioural Inventory, BBI),47 the majority were cognitively and behaviourally intact at the time of their first interview (shown in online supplemental appendix B). Longitudinal ECAS or BBI data were not available.
Positive aspects
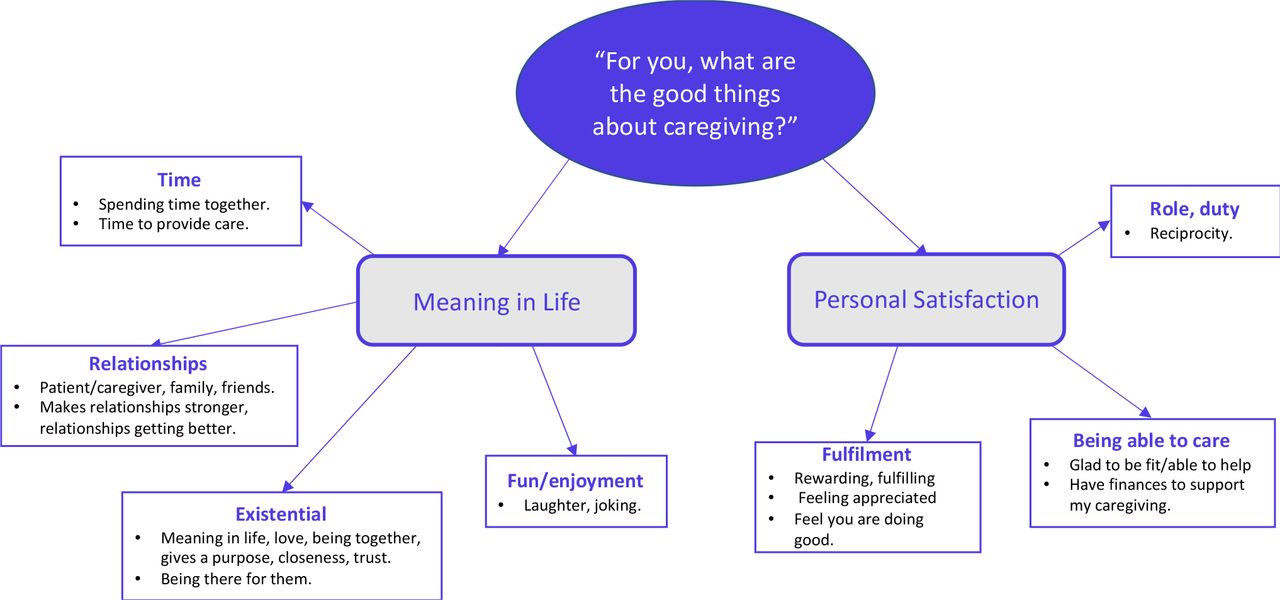
‘For you, what are the good things about caregiving?’ Respondents were asked to describe what for them were some of the positive things about caregiving. Coding and thematic analysis of the qualitative data were carried out independently by three researchers (two female psychologists and a female health services researcher) attached to the National clinical centre. Two main themes with associated subthemes were generated from the responses: theme 1, meaning in life and theme 2, personal satisfaction (figure 3).

Thematic map: positive aspects of caregiving.
The themes were quantified in terms of the frequency of occurrence in the dataset and are presented in figure 4A with associated subthemes (see figure 4B in online supplemental appendix D).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Frequency of themes over time (n = 17).
Describing positive aspects associated with being a caregiver, over two-thirds of responses were coded to meaning in life at baseline. Positive factors related to the theme of personal satisfaction represented 59% of all responses at the third interview.
In the following section, these two themes are explored in greater detail, with illustrative quotes provided. There are verbatim pseudonymised quotes indicating the interview time point and relationship to the person with ALS.
Theme 1: Meaning in Life
The theme of meaning in life comprised subthemes of ‘time’, ‘relationships’, ‘existential’ and ‘fun/enjoyment’. This captures the depth and complexity of reflection and (re) connection while providing care for a loved one with a terminal illness. Meaning in life is derived from their relationships and as a lens through which caregivers discuss a shift in focus and values.
The concept of ‘time’ was described in terms of spending time together, reprioritising time/creating time to be together and having time to provide care as positive aspects. Perhaps contemplating the nature of time, and how it takes on added value in a progressive and life-limiting condition.
"Spending more time with her" (daughter, T2)
"the time we can spend together. It allows us time to talk about practical stuff" (female spouse/partner, T3)
"Spend a lot of time together, talk more" (female spouse/partner, T3)
The quality and nature of relationships contributed to meaning in life. The relational connections between the caregiver and the PlwALS, family and friends grew stronger and for many became of better quality. The cognitive and emotional impacts of observing the challenging experiences of another may alter interpersonal relationships.
"Brings us closer, we're more involved, watching, keeping an eye on her and we do everything together" (daughter, T2)
"It’s a journey we didn't expect to travel on but now there, find what’s good in our relationship" (female spouse/partner, T4)
"It brought the family together and a new appreciation for each other" (female spouse/partner, T1)
‘Existential’ factors pointed to a re-evaluation of what matters and what is considered as important and included: love, purpose in life and being present for the PlwALS. The comments describe the realisation of the importance of closeness and ‘being present to the other’, and how an experience like this can crystallise the importance of connections that over years can be lost.
"The making a loving relationship (44 years) even more loving" (male spouse/partner, T4)
"Connection, closeness, positivity that we both found. […] he’s been brave for me and I've been brave for him" (female spouse/partner, T4)
"You take things for granted before" (female spouse/partner, T0)
There were opportunities for humour. ‘Fun/enjoyment’ contributed to meaning in life for many. This included laughing together and enjoying doing things together. This points to the importance of allowing the space for levity and humour, even in challenging situations.
"we laugh a lot, releases the endorphins" (female spouse/partner, T4)
"The laughs we can have in between the serious situations" (female spouse/partner, T4)
"He can joke about things and see the positive. Good friends which keep us upbeat" (female spouse/partner, T0)
Theme 2: Personal Satisfaction
Feeling able to provide care and being strong and healthy enough to do what is required were identified as positive factors for caregivers during their interviews.
"Feel good that I am able to look after him" (female spouse/partner, T0)
"I never thought it would happen, who does? But I'm glad I can, and I have my health to do it" (female spouse/partner, T2)
Caring was described as a fulfilling and rewarding experience, good feelings were associated with helping someone and being appreciated. A personal sense of satisfaction derived from mastering tasks identified, and from receiving positive feedback as a result of completing those tasks.
"Seeing how much she appreciates it" (male spouse/partner, T2)
"Quite joyful helping people, there is a reward" (male spouse/partner, T2)
"feel like you're doing good for someone who can't do anything themselves" (female spouse/partner, T4)
"When I see him happy makes it worthwhile" (female spouse/partner, T3)
‘Fulfilment’ of a filial or spousal duty or obligation was evident, and some people mentioned that now in times of illness the caregiver could return the care that the PlwALS had shown to them previously; reciprocity featured particularly in spousal relationships. Being able to provide care and support at home keeps the person with ALS from hospital and longer-term care was a source of satisfaction
"You just automatically do it, it falls into what you have to do" (female spouse/partner, T3)
"I suppose it cements our position together put it that way. You marry someone for rich or poorer in sickness and in health" (male spouse/partner, T0)
There was manifest reciprocity and opportunity to ‘give back’:
"If it was the other way around, he would do his best for me" (female spouse/partner, T2)
Burden category and themes
A carer burden score (ZBI) above the cut-off of ≥2442 is considered to be ‘high’ burden. Grouped into low and high burden categories according to their mean burden score at each of the five interviews, a majority, although decreasing, of caregivers were in the low burden category over time—82% at the first interview, 88%, 71%, 71% and 50% at the subsequent four interviews, respectively.
At the third interview, caregivers in the high burden category mentioned factors related to the theme of personal satisfaction as positive aspects of caregiving, as did 75% at the last interview. Half of low burden caregivers recounted aspects of personal satisfaction at the first interview, rising to three-quarters at the fifth and last interview.
High and low burden caregivers mentioned positive factors related to the theme meaning in life. At the fifth interview 63% of low burden caregivers and 38% of those in the high burden group described factors related to that theme as positive.
Discussion
This longitudinal mixed-methods study is an innovative way of examining caregiver experiences over time. Quantitative and qualitative analyses were used in combination to provide a greater understanding of informal caregiving than either approach alone would provide.48 We extended the breadth of inquiry by using different methods to assess different components of their experiences.49 50
This study examined the experiences of 17 informal caregivers over the course of 1.5–2.5 years. Considering the average duration of ALS, this has provided a remarkable insight into the lives of people living with this progressive condition. In line with previous research7 10 51 the caregivers were predominantly female and spouse/partners of the person living with ALS.10
Research has shown the negative impact and challenging life circumstances for informal caregivers in ALS. The findings in this study reflect that, with increased burden and psychological distress over time. However, it is noteworthy that over the course of the 5 interviews with these 17 caregivers, just over one-quarter reached the cut-off score for high burden and 35% for probable psychological distress. At baseline—the first interview—the only statistically significant difference between these seventeen caregivers and the larger cohort of caregivers (n = 56) was in hours of care provided per week (online supplemental appendix B). It is possible that those who consistently respond to longitudinal studies are less burdened and negatively impacted by their role and their appraisal of it.
Two main themes were inductively generated from the qualitative analysis. The themes of meaning in life and personal satisfaction reflected both the importance of the relational aspects of caregiving, and the personal fulfilment associated with being present and able to support the care recipient. Perceived gain and satisfaction are some of the positive effects of the caregiving relationship.26 30
The evaluation and re-evaluation of what is considered meaningful, satisfaction, relationship quality, the importance of time, being able and available to give care, to fulfil a role and take responsibility, and master tasks as they present themselves were described. The frequency with which the positive aspects as thematised were mentioned fluctuated across the five interviews. Previous research has noted different phases in caregiver trajectories.14 15 Our findings describe a phasic appreciation of positive factors along the care paths for this group of informal caregivers.
If we view caregiving as a phasic trajectory, it is interesting to note that aspects associated with meaning in life were mentioned more frequently at the first and final interviews, and those associated with personal satisfaction were mentioned more often at the second to the fourth interview time points. As such meaning in life comprising positive existential and relational factors were identified at the beginning and end phases of the caregiving trajectory. The middle phases may be a time when caregivers are occupied with practicalities and tasks and derive positivity when these can be acquitted satisfactorily; then closer to end of the disease course, meaning and existential factors such as time and relationship come back into focus. The positive aspects identified in this analysis point to a degree of accommodation to the biographical disruption52 of ALS, as it splinters the narratives caregivers have to understand themselves and the trajectories of their lives.
Overall, the majority of caregivers were in the ‘low burden’ category across the interview series. We examined the positive aspects of caregiving as thematised in this study and their association with burden category. When caregivers were dichotomised by high/low burden scores, positive aspects of caregiving related to personal satisfaction were mentioned alongside high burden. Almost two-thirds of low burden caregivers endorsed aspects related meaning in life at the final interview. There were small numbers for comparative analysis, but a tentative indication that positive assessments may be influenced by the burden level experienced.
The positive aspects of caregiving identified by these caregivers changed, and the adaptive cycle identified here could be useful in the future design and delivery of supportive interventions. Research on improving caregiver well-being suggests targeting predictable points in the ALS/MND timeline.53
This caregiver adaptive cycle may mirror or coexist with the cycle of anticipatory grief in terminal illness.54 Adaptation may be dependent on the caregivers individual coping style,55 which may be a key factor when acknowledging positive aspects of caregiving. Further research should evaluate how coping styles affect the adaptations identified in this study and assessment of coping should be assessed in interventions targeting caregivers. The recognition of positive aspects associated with caregiving in progressive conditions may help in mitigating the risks of burden and psychological distress, both phenomena have been well described in ALS research.10 Tracking self-reported outcomes and unstructured responses of caregivers over 2.5 years, which considering the average disease duration, provides unique insight into experiences over time and are strength of the study. The mixed-methods design is a considered approach to caregiver studies and enhances understanding of the caregivers’ experiences. The study of positive aspects of caregiving in ALS is a novel area of research and so this study adds to a modest evidence base. Additionally, the use of a mixed-methods design enhances our understanding of the caregivers’ experiences, by including both standardised measures and qualitative insights.
The absence of longitudinal cognitive and behavioural data for PlwALS, as the additional versions of ECAS had not been validated at the time of data collection, is a limitation of this study. The inclusion of cognition and behaviour measures would provide additional perspective. Findings from the study of participants (n = 17) reflect their responses and as such we cannot infer anything beyond this cohort.
Future research should continue to focus on the importance of involving family and informal caregivers in clinical care, and explore factors which facilitate participation in longitudinal research.
Interventions should be implemented for caregivers of PlwALS, which consider and use positive experiences in their design. Design of supportive interventions should include appraisal of positive aspects which may mitigate the identified difficulties. It is important to recognise the temporality and adaptation inherent in the caregiving experience. Support and interventions offered may be more appropriate at various times.
Data availability statement
Data are available on reasonable request. The data presented in this study are available on reasonable individual request from Mark Heverin Research Manager in the Academic Unit of Neurology in Trinity College Dublin.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethics (Medical Research) Committee - Beaumont Hospital.REC reference: 18/68. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors ÉC, PK and MG contributed to the manuscript write up. All authors read and approved the final manuscript. Conceptualisation: ÉC, PK, and MG; methodology: ÉC, PK and MG; formal analysis: ÉC, PK, and MG; data curation: MH; writing—original draft preparation: ÉC, PK and MG; writing—review and editing: ÉC, PK, MH, OH and MG; supervision: OH and MG; project administration: MH and MG; funding acquisition: OH and MG. MG is the author acting as guarantor. All authors have read and agreed to the published version of the manuscript.
Funding This work was supported by funding from the Global Brain Health Institute (GBHI), Alzheimer’s Association, and Alzheimer’s Society Pilot Awards for Global Brain Health Leaders (ALZ UK-20-638907). Funding of the parent ALS-CarE study was provided by the EU Joint Programme-Neurodegenerative Disease Research (JPND-2013-1) through the Health Research Board (HRB).
Competing interests OH is editor-in-chief of the ALS and Frontotemporal Degeneration Journal. She has been a consultant for Cytokinetics, Alexion, AveXis, Biogen and Novartis.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.