Article Text

Abstract
Objectives (1) Assess the distribution of skin-to-deltoid-muscle distance (SDMD) at the deltoid intramuscular (IM) injection site; (2) its relationship with demographic and anthropometric variables and (3) Consider the findings in relation to clinical guidance on IM injection, such as COVID-19 vaccines.
Design Systematic review using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Data sources MEDLINE, EMBASE, ClinicalTrials.gov, Cochrane Library, CINAHL and SCOPUS between June and July 2021 with no publication date limit.
Eligibility criteria Studies reporting measurements of the SDMD in living adults aged 16 years and older, at the deltoid IM injection site, published in English were considered.
Data extraction and synthesis Two independent reviewers performed each stage of screening, data extraction and quality assessments using the Joanna Briggs Institute Critical Appraisal Checklist for analytical cross sectional studies.
Results 16 105 papers were identified, of which 11 studies were suitable for review, representing 1414 participants. Heterogeneity in the definition of the deltoid IM injection site, locations measured and methods of measurement precluded meta-analysis. Evidence from ultrasound SDMD measurements demonstrated some patients in all but ‘underweight’ body mass index (BMI) categories, may require needles longer than 25 mm for successful IM injection. Calliper measurements overestimated SDMD compared with ultrasound. Female sex, higher BMI categories and greater weight in women were associated with greater SDMD.
Conclusions The reviewed evidence was insufficient to inform definitive needle length ‘cut points’ for IM injection based on demographic or anthropomorphic variables. Contemporary clinical guidance currently based on this evidence, including the site of injection and choice of needle length, may result in subcutaneous administration in a small proportion of recipients, particularly if obese or of female sex.
PROSPERO registration number CRD42021264625.
- infectious diseases
- ultrasound
- public health
- anatomy
Data availability statement
Data are available on reasonable request. Further tabular data can be made available by emailing the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
A systematic search of six major electronic databases reported per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Inclusion of additional data and clarification was provided by authors of some of the reviewed publications, allowing further interpretation of previously published work and comparison between studies not previously possible.
Heterogeneity in the definition of the deltoid intramuscular (IM) injection site, locations measured and methods of measurement precluded meta-analysis.
This review only considered studies relating to adults, the deltoid IM injection site and which were published in English.
Introduction
The deltoid muscle is a common site for intramuscular (IM) injection. Underpenetration of the needle risks failed delivery of drugs, reduced immunogenic response to vaccinations1–3 and can cause adverse events such as local tissue reaction, abscesses and granuloma formation.2 4–6 Reaching and adequately penetrating deltoid muscle for IM delivery of drugs is of particular importance amidst contemporary global efforts to vaccinate against COVID-19. As it is not routine clinical practice to confirm IM injections have been delivered into the deltoid muscle, or indeed to assess vaccine response, healthcare professionals rely on clinical guidance to ensure IM delivery.
The skin-to-deltoid-muscle distance (SDMD) that must be penetrated for IM injection can vary with age, sex, weight, body mass index (BMI) and other characteristics such as arm dominance.7–9 Many countries adopt protocols that consider some of these factors when advising how to choose needle length in national IM injection and vaccination guidelines, but recommendations are heterogenous.2 10–12
This study is a systematic review of the distribution of SDMD and its relationship with demographic and anthropometric variables in adults which could help inform appropriate needle length for IM injection. We consider the findings in relation to clinical guidance on IM injection, and the regulatory requirement for the IM delivery of current COVID-19 vaccines.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines13 14 were used to report the process and results. A search strategy was developed with a University Medical Librarian to identify literature reporting SDMD in adults at the deltoid IM injection site, and registered on PROSPERO (CRD42021264625). Studies were reviewed for reports of associations between SDMD and anthropomorphic or demographic variables, deltoid muscle point of measurement, methods of measurement and limits of agreement between radiologic and physical measures. Inclusion criteria were non-experimental or experimental clinical trials, in living humans aged 16 years or older, reporting SDMD at the site of IM injection using radiologic or physical evaluation. Exclusion criteria included cadaveric studies, only reporting participants aged under 16 years, if a publication full text was not available in English or unable to be located.
MEDLINE, EMBASE, ClinicalTrials.gov, Cochrane Library, CINAHL and SCOPUS were searched between 27 June 2021 and 8 July 2021, with no publication date limit (search strategy provided in full in online supplemental material A). Search results were uploaded to Covidence to remove duplicates and manage screening,15 which was performed independently by two reviewers. Disagreements were discussed until a consensus reached, with arbitration by a third reviewer where necessary. The same method was used for full-text review and data extraction. Quality assessment was done using the Joanna Briggs Institute Critical Appraisal Checklist for analytical cross sectional studies.16 Two reviewers independently determined if eight quality criteria were present, decided an overall risk of bias, made prose notes, and gave an overall recommendation for inclusion or exclusion (online supplemental material B). Discordances were reviewed by discussion, and a consensus decision reached. Meta-analysis was precluded by heterogenous study sample characteristics, anatomical sites measured and measurement methods. Where appropriate, point estimates and CIs for particular comparisons for individual studies, are estimated from reported summary data. Skinfold calliper measurements were halved to convert to SDMD.17 Data were manually extracted and cross-checked by a second reviewer from figures in two papers where the authors could not be contacted to request this.9 18 A more comprehensive description of methods is available in online supplemental material.
Supplemental material
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Results
A summary of how publications were selected for data extraction is presented in figure 1. Some potentially relevant publications were excluded on the grounds of being unable to separate data for ineligible participants <16 years of age19 20; not specifying participant counts for reported groups21; a high risk of bias due to unreported key aspects of study design and participant characteristics22 and one study for which the SDMD was not a complete measure.23 For two publications identified which required further information to be eligible for inclusion; the authors were able to provide raw data which facilitated this.3 24 Table 1 presents the characteristics of included studies.
Characteristics of included studies

Study flow diagram. SCT, subcutaneous thickness.
Skin-to-deltoid-muscle distance
The mean and range (minimum to maximum) of SDMD extracted from studies reports is shown in figure 2. Poland et al proposed a definition of the needle length required for IM injection to be the SDMD plus five millimetres penetration into the deltoid muscle, to ensure adequate delivery of injected material within muscle tissue.9 Where the vertical line indicating the range for any individual study crosses the dashed red line in figure 2 this indicates participants in that group who would have required a needle longer than 25 mm to achieve IM injection.
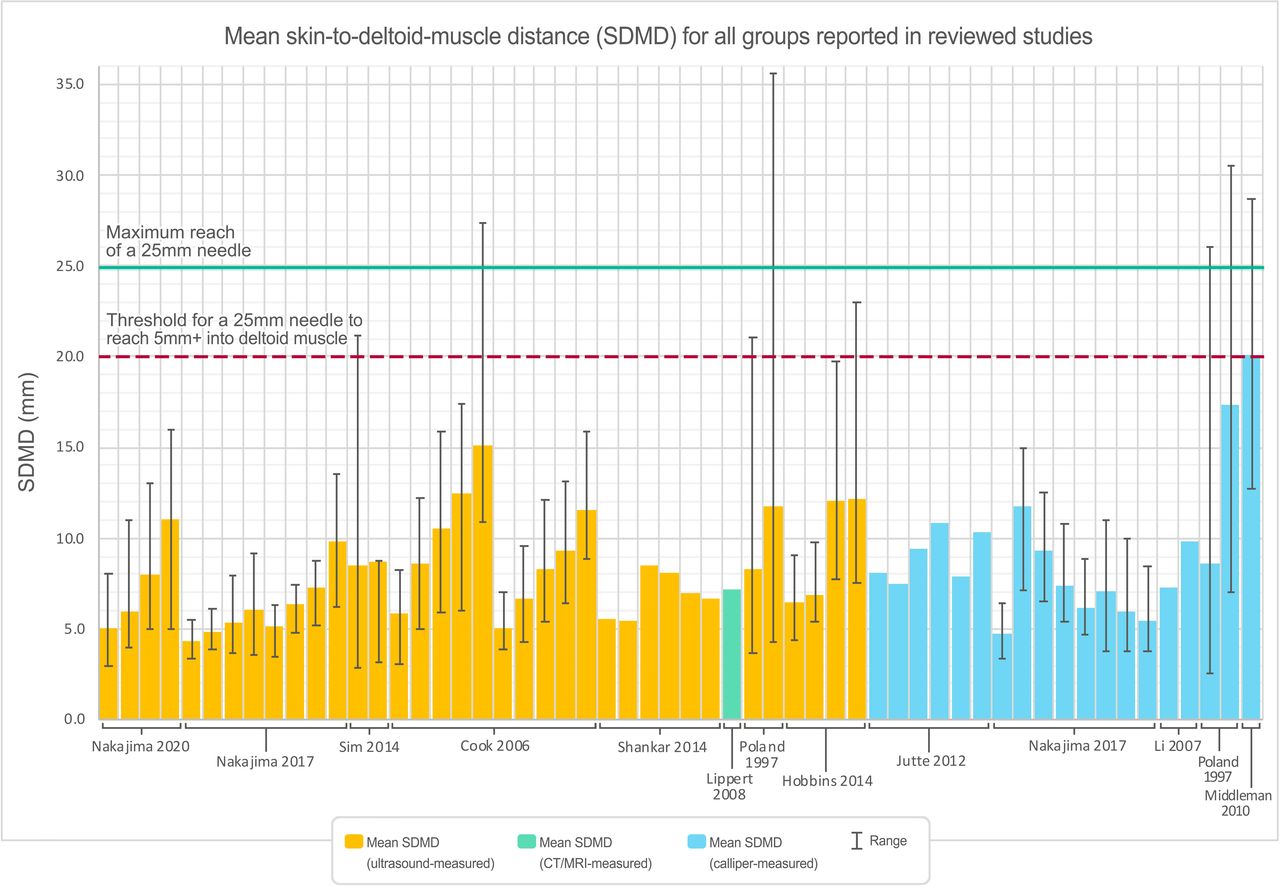
Mean SDMDs reported for participant groupings in reviewed studies, coloured to indicate method of measurement (yellow=ultrasound, green=CT/MRI, blue=calliper). Error bars represent the reported range of values contributing to each mean SDMD for data points where this information was available. Horizontal lines indicate the reach of a 25 mm needle (green solid line), and threshold for requiring a needle longer than 25 mm to reach at least 5 mm into the deltoid muscle (red dashed line).
BMI and SDMD
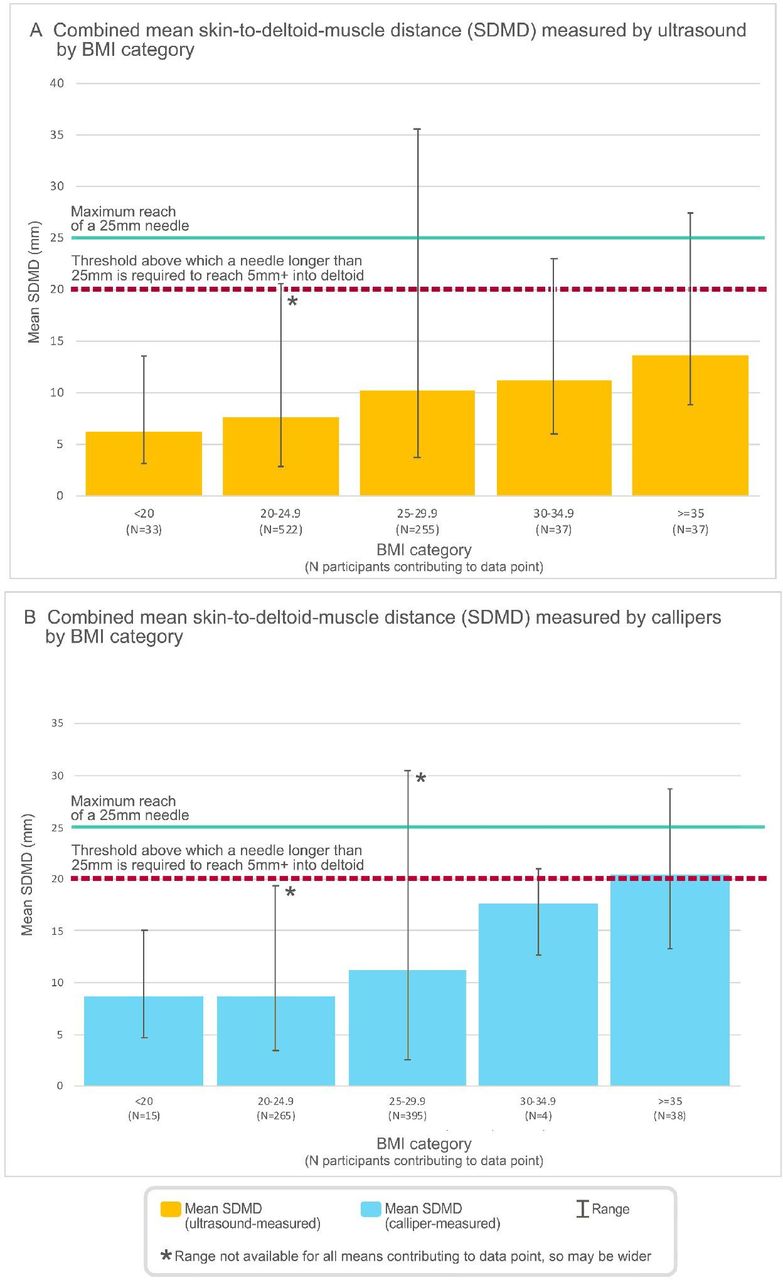
Seven studies reported mean SDMD measured by ultrasound and mean BMI data (figure 3A),7–9 24–27 and five studies reported mean SDMD measured by callipers and mean BMI data (figure 3B).3 9 26 28 29 Both figures suggest a positive association between mean SDMD and BMI category. Apart from the category of BMI <20, and BMI 20–24.9 for calliper measurements only, at least one participant in every other BMI category would have required a needle longer than 25 mm, based on the requirement of deltoid muscle penetration by 5 mm or greater proposed by Poland et al (figure 3A,B). In figure 3B, the mean needle length required for those in the BMI category of ≥35 crossed this threshold also.

Combined mean SDMDs measured by (A) ultrasound and (B): callipers, extracted from each study that also reported mean BMI. Where multiple measurements of SDMD were taken per participant (in both arms, or different IM injection sites on the same arm) the mean of SDMDs for all sites measured was used so that each participant was only counted once. The overall mean SDMD was calculated for each BMI category, weighted by the proportion of participants contributed by each mean. Error bars represent the range of values contributing to each mean SDMD. Horizontal lines indicate the reach of a 25 mm needle (green solid line), and threshold for requiring a needle longer than 25 mm to reach at least 5 mm into the deltoid muscle (red dashed line). BMI, body mass index; IM, intramuscular.
Li et al calculated the Pearson correlation coefficient of BMI and skin fold thickness (double the SDMD) to be 0.492 (significant at p=0.013), which indicates a moderate positive association between these variables.29 Shankar et al calculated regression equations and found strong positive association between SDMD measured by ultrasound and BMI in both arms.8 Sim et al included SDMD measurements by ultrasound from points on the upper arm that were below the deltoid area, but also reported positive association between SDMD and BMI in calculated regression equations.27
Weight and SDMD
Mean weight and SDMD data could be extracted from five papers; review of the data points without formal statistical analysis suggests a positive association. Poland et al reported that all 9 women who were >90 kg, and one woman who was in the 60–90 kg weight (N=86) range would have required a needle longer than 25 mm to ensure IM injection.9 All male participants would have had a successful IM injection using a 25 mm needle regardless of weight. Cook et al noted similar findings but found BMI to be a better correlate of SDMD, and for predicting the required needle length for IM injection in females.
IM injection site
The included studies variably defined the point (or area) where SDMD measurements had been made (figure 4), reflecting varied definitions of the deltoid IM injection site in clinical guidance. Where multiple sites were measured on the same participants, there was evidence of within-participant variation in SDMD.25 26

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Measured sites of SDMD in the reviewed studies.
Deltoid region of measurement
Nakajima et al measured SDMD at four sites separated vertically across the deltoid muscle height (figure 4). The chosen points were used for deltoid IM injection in clinical practice at the time of conduct. Differences in SDMD between the farthest apart sites were significant for both male and female participants, for both ultrasound and calliper measurements.26 The differences in mean SDMD by ultrasound were 1.8 mm (42%) greater in male participants and 4.7 mm (92%) greater in female participants, when comparing the thickest to the thinnest sites measured.
Nakajima et al25 made measurements of SDMD in a similar participant demographic at two sites separated vertically across the deltoid muscle height using ultrasound (figure 2). The mean SDMD between the thicker and thinner sites measured was 1 mm (20%) greater for male, and 3 mm (38%) greater for female participants.
Sim et al used ultrasound to measure the subcutaneous tissue thickness at eight locations on the upper limb, two of which appear to be over the deltoid muscle area used for IM injections, and were separated horizontally.27 The difference in mean SDMD between these two sites of 0.21 mm was not statistically significant when we performed an unpaired t-test on the reported means.
Limits of agreement between methods of measurement
Nakajima et al and Poland et al were the only studies to assess SDMD using multiple methods of measurement in the same group of participants, both using callipers and ultrasound.
Taking ultrasound measures as the true measure, they reported that callipers overestimated mean SDMD by between 0.3 and 1.0 mm in male participants (3.6–16.4%), and between 1.0 and 5.65 mm in female participants (15.6%–48.3%).
Age and SDMD
Shankar et al reported regression equations by arm dominance (right for all participants) which both demonstrated an inverse relationship between SDMD and age.8 Sim et al also found an inverse correlation between skin to muscle thickness and age, although we note that only the uppermost two out of eight upper arm sites included in this calculation appear to fall over the deltoid muscle area (the others being below this).27
Sex and SDMD
SDMD by sex could be extracted from eight studies, and whether measured by ultrasound or calliper, differences were greater for females than males at all sites (range 1.16–2.02 fold greater, online supplemental figure 1).7–9 24–28
Ethnicity and SDMD
No publication reported a breakdown of participant ethnicity or explored a relationship between ethnicity and SDMD.
Arm circumference and SDMD
One study reported maximum mid-deltoid arm circumference,9 which was greater in male participants compared with female (332 mm vs 310 mm), while mean SDMD measured by ultrasound was lower in male participants compared with female (8.3 mm (range 3.7–21.1) vs 11.7 mm (range 4.3–35.6)) and calliper-derived measurement (8.6 mm (2.5–26.0) vs 17.35 mm (7.0–30.5)).
Arm dominance and SDMD
Two studies measured SDMD in both arms of each participant.8 24 Shankar et al found the non-dominant arm had 0.3 mm (4.5%) greater SDMD than the dominant arm, which was significant at p=0.01 using paired t-tests.8 The difference in arms in Hobbins et al’s provided raw data of 0.09 mm was not significant using unpaired two-tailed t-tests.
Discussion
Key findings
This systematic review identified that there is insufficient evidence to reliably determine the appropriate needle length for deltoid IM injection in adults using demographic or anthropometric characteristics. The specific point of deltoid IM injection may be clinically important with evidence of up to almost double the SDMD between sites recommended in contemporary clinical guidance. Elevated BMI and female sex were the anthropomorphic and demographic variables most strongly associated with increased SDMD. There was some evidence of an inverse relationship between age and SDMD. Non-dominant arms had a slight (less than 5%) but significantly increased SDMD, but this is unlikely to have clinical relevance. Any potential effect of ethnicity on SDMD could not be assessed due to limited studies presenting this data, and limited variation in studied populations where available. Using the criteria that the needle length needs to be at least 5 mm more than the SDMD to ensure deposition within muscle, we found that some patients in all BMI categories (apart from underweight) would have required needles longer than 25 mm for successful IM injection. The proportion of participants affected appears to correlate positively with BMI, indicating that obese (BMI ≥30 kg/m2) populations are most at risk.
Since completion of our literature review, Sebro published a retrospective cohort study of 386 individuals using CT to measure SDMD and evaluated biometric data as a predictor of this distance.30 They found BMI and age the best predictors of SDMD, and also noted that almost a quarter of those above the Centers for Disease Control and Prevention threshold for using a longer 38 mm needle (200 pounds for females, 260 pounds for males), would still not have achieved IM injection. This highlights a further issue in recommended needle length that disproportionately affects obese individuals.
Defining the ideal needle length
We used the definition of needle length required for IM injection proposed by Poland et al of ‘penetration of the needle into the deltoid muscle layer by 5 mm or more’.9 This has been reused in subsequent research,7 8 26 and recommendations based on this definition have been incorporated and cited in contemporary national clinical guidelines.12 31 32 To our knowledge, evidence of this being the optimal muscle depth necessary for successful IM injection has not progressed beyond the level of expert opinion since proposal, and could benefit from formal assessment given the clinical decisions being made based on this. IM injection guidance could be overestimating the required needle length if 5 mm penetration is more than necessary, or underestimating this if either 5 mm is less than is necessary or space is left between skin and needle hub in clinical practice as described in their protocol.9
Methods of measurement
We have considered direct ultrasound measures as the gold standard for SDMD measurements. Callipers overestimated SDMD compared with ultrasound measurements in studies where both were performed.9 26 The degree of overestimation was greater for females than males.33 Absolute differences in millimetres were small for the sampled participants who had low-normal or healthy BMIs; but if the measurement error scales with higher BMIs it may limit the clinical utility of this method of measurement to inform needle length for IM injection. We note callipers can also underestimate subcutaneous fat through tissue compression during measurement, individual differences in tissue compressibility, and may be unsuitable in obese individuals with very thick adipose tissue.34 Skin stretching or ‘z-tracking’, where the skin is pulled to one side prior to IM injection and released after, is noted in some research, and current Canadian vaccine guidance, for example, but we are unsure of its wider prevalence.3 12 This theoretically disrupts the tract formed by injection and is intended to reduce leakage of injected material from the muscle back into subcutaneous tissues. We are not aware of evidence of whether the pressure of this technique could reduce SDMD, and it may be worthy of study to determine if it can alter the ideal needle length recommended for successful IM injection.
Deltoid region of measurement and clinical guidance
Through multiple SDMD measurements per participant, two studies demonstrated increasing SDMD with movement away from the acromion towards the deltoid tuberosity (figure 2). The IM injection sites studied are used in current national clinical guidelines, the thinnest being advised for COVID-19-specific vaccination in Ireland and the USA,31 35 and the thickest (at up to almost double the SDMD for women) being used for general vaccination in New Zealand.11 Therefore, the precise site chosen on an individual for IM injection could markedly alter the needle length required for IM injection. A further consideration is that the latter (thicker) site has been determined the safest for avoiding damage to the posterior circumflex humeral artery and axillary nerve during IM injection.26
Sim et al’s study suggested no significant variation in SDMD between two points of measurement separated horizontally over the deltoid muscle, although we note limitations of interpreting this data as the specific points measured, and distance between them is unclear, and the skin tool used to identify sites could not be located.27 We, therefore, cannot determine whether the positioning in the transverse plane of an IM injection also influences SDMD.
Arm circumference and SDMD
One study reported the mean maximum mid-deltoid arm circumference of participants,33 and noted larger mid-deltoid arm circumferences but thinner SDMD in male participants. The former may be explained by increased muscle mass in males in this area compared with females.8 9
SDMD and immunogenicity
Needle length may have implications for effective vaccine delivery and response. Compared with IM injection, subcutaneous injection of vaccines resulted in more adverse effects (high-grade evidence), and reduced or equivalent immune response (moderate-grade evidence).36 Studies have reported associations between elevated BMI and reduced serum response to vaccination for influenza,37 hepatitis B,38 rabies39 and tetanus.40 There is randomised controlled trial data demonstrating that randomising obese adolescents, who are at risk of being vaccinated with a needle of insufficient length, to a longer needle, resulted in significantly higher antibody titres following hepatitis B vaccination.3 More recently, Pellini et al studied the response to SARS-CoV-2 BNT162b2 vaccine 7 days after vaccination.41 They found a difference in immune response between BMI classes, with higher values in low-BMI and normal-BMI participants, compared with overweight and obese participants. This was significant after adjusting for age by classes and gender, but not when considering age as linear data.41 A greater chance of subcutaneous deposition of the vaccine in those with elevated BMIs could contribute to findings of reduced immune response. As obesity is a major risk factor for increased morbidity and mortality in COVID-19 infection; determining any interactions between BMI, SDMD and COVID-19 vaccine response, and whether these are clinically important, is a pertinent issue to resolve.42
Limitations
Only a small minority of the 16 485 studies reviewed, across six databases, presented relevant data on SDMD and this prevented a more granular systematic review of particular population demography or anthropometry subsets.
The demographics of the study populations in reviewed papers may not represent priority groups for vaccination. Ethnicity data were rarely reported. Participants with a BMI>30 kg/m2, a typical cut point used to define obesity, were often under-represented. Importantly, those with obesity appear to have the greatest potential need for longer needles, highlighting a need for further research that defines optimal vaccine delivery in this population.
The varied definitions of IM injection sites across studies are problematic given evidence that the precise location of measurement can alter SDMD significantly.25 26 The side of measurement also influenced SDMD to a small but important degree.8 The methods of SDMD measurement reported were not equivalent with callipers overestimating SDMD and also being influenced by gender.26 33 Although strong correlation has been established between ultrasound subcutaneous tissue measurements, and calliper-measured skinfold thickness; this lessens as fat thickness increases, and equivalence has not been validated.43 Although ultrasound has been regarded as the more accurate method, ultrasound B-mode image interpretation also has an element of subjectivity and probe pressure may reduce the SDMD adding a variable element of operator technique to these results that might limit validity of direct comparisons.44 Measures of SDMD have been performed in studies with MRI, CT and radiographs,18 22 however, direct comparisons have not to our knowledge been made and no validated gold standard exists. There was insufficient reporting of variability (eg, SD) for any of the associations preventing pooled analysis.
The needle length required for successful IM injection may be variably interpreted based on the depth of deltoid penetration considered ideal, which to our knowledge, has not been proven to date. The SDMD may be compressed by clinical techniques such as applying pressure and skin stretching when injecting, which are recommended in some clinical guidance,12 31 32 but were not considered in any of the research reviewed.
Future study
Given the practice of vaccination is conducted globally and on billions of individuals, the paucity of current literature on optimal needle length choice, and the limitations of the available studies are noteworthy. A small number of studies included in this systematic review are often referenced in immunisation guidance worldwide to inform IM vaccination delivery, but clearly this evidence is lacking. This review highlights that relatively few studies have been published specifically exploring SDMD as it relates to vaccination needle length choice. More data are needed in diverse populations, particularly those who are priority groups for immunisation programmes, such as those with obesity and associated comorbidities. Larger studies should explore the potential interactions of demographic characteristics such as age, sex, ethnicity and BMI on SDMD, and to evaluate the relationship of immune response to vaccinations with unintended subcutaneous delivery after attempted IM injection. Given the importance of mass vaccination in public health responses to the COVID-19 pandemic, and the importance of immunisation programmes generally, this is a key area where recommendations need stronger evidence to maximise the chance of success of such interventions.
Conclusion
The reviewed evidence was insufficient to make confident recommendations about required needle length for IM injection based on demographic or anthropomorphic variables. Contemporary clinical guidance for IM injection technique, including choice of needle length, may not ensure IM injections such as vaccines are always delivered into the deltoid muscle. The precise site of deltoid IM injection, which varies in international guidance, appears important when considering the needle length required in clinical practice. Standard needle lengths of 25 mm may result in subcutaneous rather than IM administration in a small proportion of recipients with normal and elevated BMI, which is particularly worrisome for obese people, especially women, for whom the limited data available suggests have greater SDMD, and thus a greater chance of requiring a longer-than-standard needle. This is troubling in the context of global mass-vaccination efforts in response to the COVID-19 pandemic.
Data availability statement
Data are available on reasonable request. Further tabular data can be made available by emailing the corresponding author.
Ethics statements
Patient consent for publication
Acknowledgments
We are grateful to University of Otago Librarian Megan Ferris who helped design the search strategy. We would also like to thank Professor Gregory Poland, and other authors wishing to remain anonymous, for discussing their publications with us and providing additional information which supported this review. We gratefully acknowledge the Ruth Maud Ring Spencer Estate, who are proudly managed by Perpetual Guardian, whose financial support helped make this study possible.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors RB, CK, SK and LH contributed to creating the research question and study design. CK led registration, conduct and writeup. CK, CH, ED, LH, PB and SK performed title and abstract screening and full text reviews such that every paper was reviewed by at least two independent reviewers. CK, CH and ED performed quality assessments and data extraction. Disagreement was resolved by consensus. MW advised on statistical analysis and confirmed meta-analysis was inappropriate. TH, SAM and RB provided senior oversight on design and reviewed writeup. All authors (CK, CH, ED, LH, PB, SK, MD, MW, TH, SAM and RB) reviewed the draft manuscript, provided edits and approved the final draft. RB is the guarantor for this publication.
Funding This study was partially funded by the Ruth Maud Ring Spencer Estate, proudly managed by Perpetual Guardian.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.