Article Text

Abstract
Objectives To identify the barriers and enablers to implementing clinical practice guidelines (CPGs) recommendations in primary care and to provide recommendations that could facilitate the uptake of CPGs recommendations.
Design An overview of systematic reviews.
Data sources Nine electronic databases (PubMed, Cochrane Library, CINAHL, MEDLINE, PsycINFO, Web of Science, Journals @Ovid Full Text, EMBase, JBI) and three online data sources for guidelines (Turning Research Into Practice, the National Guideline Clearinghouse and the National Institute for Health and Care Excellence) were searched until May 2021.
Eligibility criteria Systematic reviews, meta-analyses or other types of systematic synthesis of quantitative, qualitative or mixed-methods studies on the topic of barriers and/or enablers for CPGs implementation in primary care were included.
Data extraction and synthesis Two authors independently screened the studies and extracted the data using a predesigned data extraction form. The methodological quality of the included studies was appraised by using the JBI Critical Appraisal Checklist for Systematic Reviews and Research Syntheses. Content analysis was used to synthesise the data.
Results Twelve systematic reviews were included. The methodological quality of the included reviews was generally robust. Six categories of barriers and enablers were identified, which include (1) political, social and culture factors, (2) institutional environment and resources factors, (3) guideline itself related factors, (4) healthcare provider-related factors, (5) patient-related factors and (6) behavioural regulation-related factors. The most commonly reported barriers within the above-mentioned categories were suboptimal healthcare networks and interprofessional communication pathways, time constraints, poor applicability of CPGs in real-world practice, lack of knowledge and skills, poor motivations and adherence, and inadequate reinforcement (eg, remuneration). Presence of technical support (‘institutional environment and resources factors’), and timely education and training for both primary care providers (PCPs) (‘healthcare provider-related factors’) and patients (‘patient-related factors’) were the frequently reported enablers.
Conclusion Policy-driven strategies should be developed to motivate different levels of implementation activities, which include optimising resources allocations, promoting integrated care models, establishing well-coordinated multidisciplinary networks, increasing technical support, encouraging PCPs and patients’ engagement in guideline development, standardising the reporting of guidelines, increasing education and training, and stimulating PCPs and patients’ motivations. All the activities should be conducted by fully considering the social, cultural and community contexts to ensure the success and sustainability of CPGs implementation.
- PRIMARY CARE
- Health policy
- Organisation of health services
- Protocols & guidelines
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
An internationally recognised guideline (the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guideline for overview) was followed to enable a transparent presentation of the methods and a replication of this study.
A very comprehensive database search was conducted (nine electronic databases and three other relevant online sources) to help achieve adequate and efficient coverage.
The barriers and enablers were categorised with the guide of a specific framework—Theoretical Domains Framework of identifying influencing factors of the implementation of clinical practice guidelines into practice.
Subgroup analysis was not conduced based on the types of health conditions, which could limit the generalisation of the study findings to one specific health condition.
Language bias could not be excluded as only English papers were included in this study.
Introduction
Clinical practice guidelines (CPGs) refer to the medical recommendations that are systematically developed based on the latest available scientific evidence, with the aim of facilitating evidence-based decision-making.1 2 Appropriate use of CPGs recommendations can bring potential benefits to patients, healthcare providers and healthcare systems by enhancing the quality of care, decreasing costs and inappropriate practice variations, and reducing preventable adverse events and mistakes.3 4 Although many CPGs are available and accessible to health providers, the underutilisation of the research evidence in CPGs is still suboptimal in primary care.5–7 The proportion of non-adherence to CPGs was up to 60% in primary care settings.8 As a result, many patients still receive suboptimal health services, and variable, costly and even inappropriate care that is inconsistent with the recommendations in CPGs.5 9 For instance, a cohort study with 438 cardiovascular disease patients from 21 primary care centres in Spain reported that 61.4% of the patients did not receive drug therapies recommended in the guidelines due to the underutilisation of the CPGs.8 Non-adherence to CPGs can lead to negative health outcomes for patients and unnecessary medical expenditures and resource use for health systems.10 11 A retrospective observational study reported that non-adherence to CPGs on psychopharmacological prescriptions can lead to two times higher incidence of adverse effects and medication costs than those adherence to CPGs.12
The implementation of CPGs in clinical practice is a complex and challenging process, as it can be influenced by different levels of factors.13–16 For example, a systematic review (SR) conducted by Flottorp et al14 summarised 57 influencing factors in seven domains (guideline-related, patient-related, individual health professional-related, professional interactions, organisational, incentives and resources, and social, legal, and political-related factors) for healthcare professional practice using the method of expert consensus. Specifically, lack of financial support, resources and staff shortage, inadequate knowledge and skills, and negative attitudes towards the CPGs are the common factors identified across practice settings and countries in previous studies.13–16 Identifying the relevant key influencing factors, including the enablers and barriers, for implementing CPGs in clinical practice is highly desirable, which can inform the development of tailored and effective CPGs implementation strategies and promote the implementation of evidence-based recommendations into practice.17 18
Several evidence syntheses studies have been conducted to conclude the influencing factors of implementing CPGs in different healthcare settings including primary care and secondary care.13 19 In 2008, an overview of SRs was published with the aim of exploring the factors that affect the CPGs implementation, in which five aspects of factors (guideline, implementation strategies, healthcare professionals, patients and environment-related factors) were categorised.13 In 2020, an updated overview was published with the literature search conducted in 2018.19 However, both the 200813 and 202019 overviews included studies in different levels of care without specifying and summarising the barriers and enablers to implementing CPGs in primary care.19 Primary care, as the first contact, continued, comprehensive and coordinated health service, plays a critical role in the provision of healthcare, where the patients can present any kind of health problems to the healthcare professionals and where most of the patients’ health needs (health promotion, disease prevention, treatment and rehabilitation) can be addressed as early as possible.20 The WHO has estimated that, in low-income and middle-income countries, improving primary care could reduce 60 million of deaths and increase 3.7 years of average life expectancy by 2030.20 Primary care and secondary care are two distinct paradigms of healthcare,21 and findings from secondary care may not be fully suitable for primary care. Given that an increasing number of SRs on CPGs implementation in primary care has been published since 2018 and none of the published overviews specifically focused on the primary care setting, this current overview of SRs was therefore conducted to achieve a full understanding of the influencing factors for the implementation of CPGs recommendations in primary care, with the following objectives: (1) to identify and synthesise the available evidence regarding barriers and enablers to implementing CPGs recommendations in primary care and (2) to proffer recommendations for implementation strategies that could facilitate the uptake of CPGs recommendations.
Methods
Study design
An overview of SRs design was adopted to synthesise the barriers and enablers to implementing CPGs recommendations to inform future practice, research and policy. This overview is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.22
Data sources and search strategies
Nine electronic databases, including PubMed, Cochrane Library, Cumulative Index to Nursing and Allied Health Literature (CINAHL), MEDLINE, PsycINFO, Web of Science, Journals @Ovid Full Text, EMBase, and Joanna Briggs Institute (JBI), were searched systematically to locate potentially eligible reviews from the inception of each database to May 2021. No restrictions regarding the language of publications were applied. Mesh terms, keywords and free words such as “Practice Guidelines”, “Guidelin*”, “Primary Health Care”, “Guideline Adherence”, “barrier*”, “enabl*”, “facilitat*” and “Systematic Review [Publication Type]” were used to develop the search strategies. In addition, we also searched the Turning Research Into Practice (TRIP), the National Guideline Clearinghouse and the National Institute for Health and Care Excellence (NICE) as the secondary resources. References of the included studies and relevant overviews on barriers and/or enablers of CPGs implementation were also searched to further identify any potentially eligible studies. Details of the used Mesh terms, keywords and free words, and search strategies of each database were reviewed by two authors with extensive experience in doing SRs and a librarian. One representative search strategy is presented in table 1. Search strategies for all the databases are presented in online supplemental file 1.
Supplemental material
Mesh terms, key words and free words, and one representative search strategy
Eligibility criteria
The inclusion criteria were: (1) study design: SRs or Meta-analyses, or other types of systematic synthesis of quantitative, qualitative or mixed-methods studies; (2) topic/interest/outcomes: barriers and/or enablers for CPGs implementation and (3) sample and context: primary care setting from the perspectives of either patients, informal caregivers, primary care providers (PCPs) (such as general practitioners (GPs), nurses and allied healthcare professionals (eg, pharmacists, physiotherapists, physical therapists) or policy makers of health services. Original studies with the aim of exploring barriers and/or enablers for the implementation of CPGs and the studies on the implementation tools of CPGs were excluded. In this study, CPGs refer to guidelines and/or recommendations that were systematically developed for clinical practice decision-making based on the available scientific evidence. Barriers and/or enablers were any influencing factors that could promote or hinder the implementation of CPGs in clinical practice. Barriers and enablers were distinguished based on how it was categorised/described in the included studies. General practice, community health and other healthcare settings outside the hospital were viewed as primary care settings in this study.
Study selection and data extraction
All the identified studies were imported into reference management software (EndNote) to check duplications. After removing the duplications, two authors (TW and X-LL) independently screened the title and abstract of the studies to locate potentially eligible studies. Then the full texts of all potentially eligible studies were obtained for full assessment by the same two authors in accordance with the eligibility criteria. Any inconsistency during the process were addressed via discussions between the two reviewers. If necessary, a third reviewer (J-YBT or IZ) from the review team was involved. Reasons for exclusion were recorded.
A predesigned data extraction form was used to extract the following information: study authors and publication year, type of review (qualitative, quantitative or mixed based on the data analysis method used in the included review), number of studies included in the review, study country/region of the original studies, targeted health problem, methodological quality of the review and relevant risk of bias appraisal tools. For the barriers and/or enablers, we went through the results of each included study carefully, and then extracted (direct citation or summarising the results) and categorised the barriers and/or enablers based on predefined content categories. The content categories/subcategories were determined based on the checklist for identifying determinants of healthcare practice,14 the Theoretical Domains Framework of identifying influencing factors of the implementation of CPGs into practice,23 and two previous SRs on CPGs implementation.13 19 Any barriers and/or enablers that were not covered by the predefined content categories were extracted in a separate table, and all those were further analysed by using summative content analysis to form new categories. More details about the predefined content categories and the development of new categories are presented in the section of data synthesis.
Methodological quality assessment
Methodological quality and evidence quality of the included SRs/meta-analysis were appraised independently by two reviewers (TW and X-LL) using the JBI Critical Appraisal Checklist for Systematic Reviews and Research Syntheses.24 The JBI Checklist includes eleven criteria: (1) ‘Is the review question clearly and explicitly stated?’; (2) ‘Were the inclusion criteria appropriate for the review question?’; (3) ‘Was the search strategy appropriate?’; (4) ‘Were the sources and resources used to search for studies adequate?’; (5) ‘Were the criteria for appraising studies appropriate?’; (6) ‘Was critical appraisal conducted by two or more reviewers independently?’; (7) ‘Were there methods to minimise errors in data extraction?’; (8) ‘Were the methods used to combine studies appropriate?’; (9) ‘Was the likelihood of publication bias assessed?’; (10) ‘Were recommendations for policy and/or practice supported by the reported data?’ and (11) ‘Were the specific directives for new research appropriate?’ (p.3).24 Each of the criteria includes four answers: ‘yes’, ‘no’, ‘unclear’ and ‘not applicable’. Any inconsistencies during the process were addressed by discussions between the two reviewers and/or the third reviewer (J-YBT or IZ).
Data synthesis
Content analysis was used to synthesise the data extracted from the included reviews. A priori content categories of the barriers and enablers to implementing CPGs in primary care were developed first to guide the data synthesis. The content categories and subcategories were determined based on the checklist for identifying determinants of healthcare practice,14 the Theoretical Domains Framework of identifying influencing factors of the implementation of CPGs into practice,23 and the findings of previous systematic synthesis on CPGs implementation.13 19 The proposed categories included: political, social and culture-related factors, institutional environment and resources factors, guideline-related factors, healthcare provider-related factors and patient-related factors. Data extracted from the included reviews were compared, combined and clustered with respect to the predefined categories. For new categories that were not covered by the above-proposed domains, summative content analysis was adopted.25 Rectification/verification of the subcategories and categories was performed throughout the coding process level and the whole dataset level to ensure all the extracted data was grouped into the most appropriate categories or subcategories. To further support and reinforce the meaning of the identified categories or subcategories for the enablers and barriers, representative data such as the text quotes in the included reviews were extracted and presented in the results section.
As this study is an overview of SRs, the ‘corrected covered area’ (CCA) was calculated to determine the overlaps of the original trials in the included SRs.26 A CCA value of 5% or below was regarded as a ‘slight overlap’, 6%–10% as a ‘moderate overlap’, 11%–15% as a ‘high overlap’ and above 15% was regarded as a ‘very high overlap’.26 A lower CCA indicates a lower likelihood of overlaps. In this study, no overlap of original trials was identified in the included SRs.
Patient and public involvement
No patients or members of the public will be involved in the design, conduct, reporting or dissemination plans of our research.
Results
Study selection
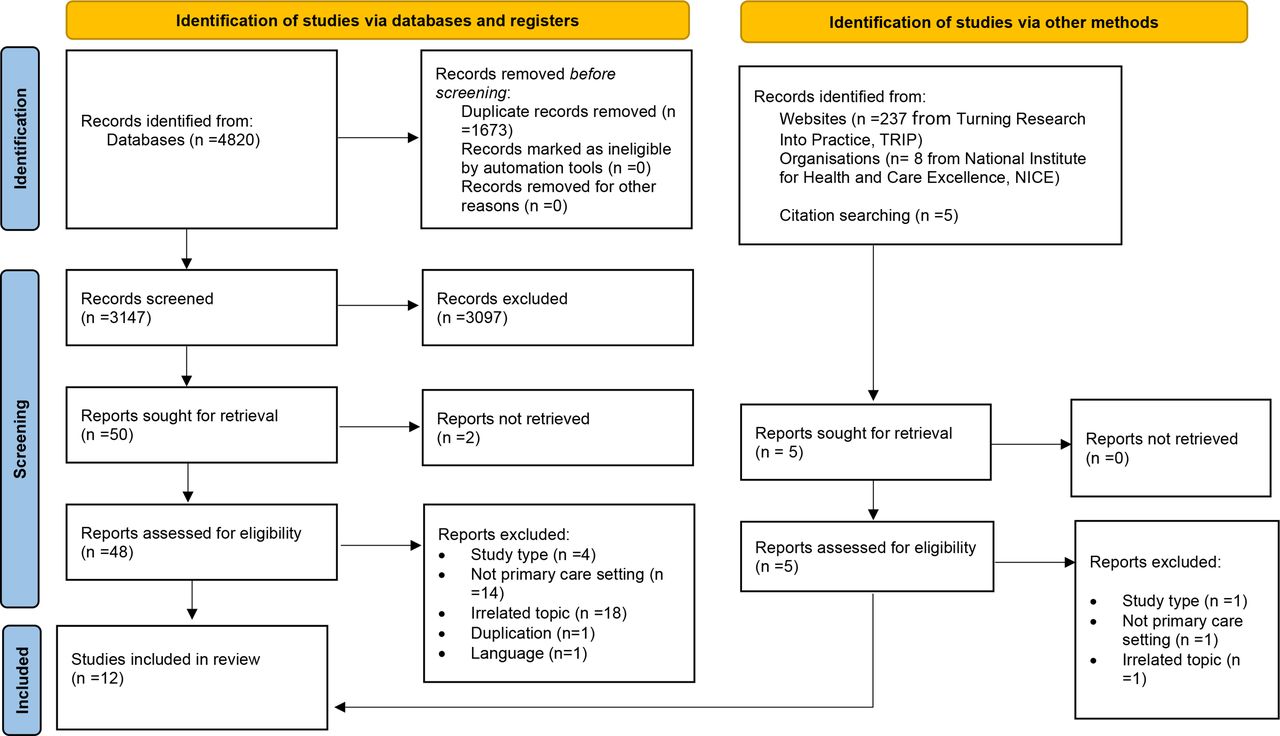
A total of 4820 articles were identified. After excluding the duplicates (n=1673), 3147 articles were left for title and abstract screening. The full texts of 50 potentially eligible records were retrieved for further assessment based on the inclusion and exclusion criteria. Ten studies27–36 were identified for inclusion. Relevant websites and organisations (TTRIP, NICE) as well as the reference list of the included articles were also searched, which yielded 250 records for eligibility assessment, and two articles37 38 were included. Thus, 12 studies were finally included in this current overview. The study selection process is presented in figure 1.
{kind=link}
PRISMA flow diagram for study selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Characteristics of the included reviews
The 12 reviews27–38 were published between 2014 and 2020, and involved 276 articles (275 studies) that were conducted in different countries or regions including the USA, the UK, Canada, Australia, Sweden, Germany, the Netherlands, Saudi Arabia, Taiwan, New Zealand, Singapore, France, Germany, Mexico, Switzerland, Belgium, Norway, Oceania, Israel, Ireland, Uzbekistan, Spain, Pakistan, Italy, Denmark and some other Asia and Africa countries or regions (not specified). Ten reviews (n=10/12)27 28 30–34 36–38 analysed the data using qualitative method (eg, thematic analysis) and the other two using mixed methods.29 35 For the participants of the included reviews, nine reviews27 29–33 35 37 38 involved PCPs only, including GPs, nurses and other allied healthcare professionals (eg, pharmacists, physiotherapists, physical therapists), while the other three reviews28 34 36 involved both PCPs and patients. The included reviews focused on various health conditions, with two reviews27 34 on osteoarthritis, and one each on asthma,28 mixed health problems,29 37 chronic kidney disease,30 diabetes,31 low back pain,32 heart failure,33 HIV,35 cardiovascular diseases36 and depression,38 respectively. A summary of the characteristics of the included reviews are presented in table 2.
Characteristics of the included reviews
Methodological quality and risk of bias of the included studies
Results of the methodological quality and risk of bias for all the included reviews are shown in table 3. The methodological quality of the included reviews was generally robust, with all the reviews receiving a quality score of 7 or above out of 11 criteria. All the reviews clearly and explicitly elaborated the review questions, data resources and the implications for policy and/or practice. Inclusion criteria, critical appraisal criterial /tools and the approach of evidence synthesis were appropriately used in most of the included reviews. Several reviews did not clearly present the search strategies,27 28 31 36 whether the quality appraisal was conducted by two reviewers independently,28 30 32 35 37 and the implications or directives for future research based on their findings.27 30 33 36
Methodological quality of the included reviews
Barriers and enablers for CPGs implementation in primary care
A total of six categories regarding the barriers and enablers for CPGs implementation in primary care were identified. These categories included political, social and cultural factors, institutional environment and resources factors, guideline-related factors, healthcare provider-related factors, patient-related factors and behavioural regulation-related factors. Some of the categories had a few subcategories for both the barriers and enablers, which were similar but not entirely the same (table 4).
Categories, subcategories and examples of the barriers and enablers to implementing clinical practice guidelines
The first five categories were consistent with two previous overviews (one was conducted in 2008 by Francke et al,13 and the other one was conducted in 2018 by Correa et al19) on different levels of care including primary, secondary and tertiary care. Although the above-mentioned five categories were also reported in other levels of healthcare, this current study identified some barriers and/or enablers within each category that were specific for primary care setting, for example, limited healthcare networks (political, social and cultural factors), limited services for specific patient groups or needs (institutional environment and resources factors), limited technical support and PCPs’ negative attitudes towards the consequences of CPGs (healthcare provider-related factors). In addition, a specific category was identified in this current study, which was the category of behavioural regulation-related factors such as remuneration, rewards and financial incentivisation for the healthcare practice or primary care professionals. Of the identified six categories, the most commonly reported categories for barriers were healthcare provider-related factors (n=10), institutional environment and resources factors (n=9), guideline-related factors (n=9) and patient-related factors (n=8); for enablers, the most frequently reported category was institutional environment and resources factors (n=10) while all other categories of barriers were only reported by half or even less than half of the included studies. More details about the barriers and enablers within each category and subcategory are presented in online supplemental file 2.
Supplemental material
Political, social and cultural factors
Barriers
This category emerged from five reviews,28 30 35 37 38 with the number of included original studies ranging from 12 to 35. The frequently mentioned barriers were the limited healthcare networks35 38 and poor interprofessional communication pathways28 30 38; conflicts between the public’s views and recommendations in CPGs35 37 and language barriers and culture diversities particularly in multiethnic contexts.28 37 Other reported barriers were too many state/federal regulations for CPGs implementation,35 uneven health resources distributions due to socioeconomic and political impacts,37 and poor coordination between different levels of care.37
Breakdowns in networks and communication pathways were seen as major barriers in many papers reviewed. (Wood, et al., 2017, p39)38
Within the domain of ‘social influences’, insufficient communication between members of the healthcare team was identified as a barrier. (Neale, et al., 2020, p10)30
Language barrier also hindered PCPs [primary care professionals] in Singapore from effectively educating their multiethnic asthmatic patients (Ezeani, 2016, p83)28
“Citizens’ views can also affect what the professional feels is feasible to do in PC [primary care]. For instance, drinking advice may be in conflict with citizens’ views about drinking as a social activity.”,(Rubio-Valera, et al., 2014 p8)37
Enablers
Only one review35 reported enablers in this category, which were developing supportive policy like congruent federal guidelines and making the recommended practice as routines; improving public’s views towards the recommended practice via public education; and state/county health department engagement with primary care.
HIV providers believed that state/county health department engagement with community based organizations and clinics was a facilitator to testing (Tan & Black, 2019, p5)35
Institutional environment and resources factors
Barriers
This category was clustered based on nine reviews,27–32 35 37 38 with the number of included original studies ranging from 8 to 35. The frequently mentioned barriers were time constraints and heavy workload of PCPs,27 28 30–32 35 37 38 financial burden including increased expenditure and inadequate funding28 31 35 38; limited availability of resources like medicines, specialists and some certain equipment and devices27 28 30 31 37; lack relevant strategies/plan for guideline implementation and dissemination28 31 35; poor referral pathway or resources27 35 37; limited technical support such as unfriendly used software/system for disease management30 38; administrative barriers such as lack of administrative support/staff35 37 and limited services for specific patient groups or needs.31 35 Other additional barriers were changing the organisations’ structure,29 38 other priorities of the clinics37 and variations in practice operations.30
Inadequate time has been highlighted as a major barrier…… Inadequate time hinders meaningful physician and patient asthma management education. Health care professionals had inadequate time to discuss patient’s medication, use of WAAP and management of asthma symptoms with their patients.(Ezeani, 2016 p84)28
Time Constraints Make it Difficult to Implement the Guidelines: Clinicians appeared to be facing an information overload. The volume of all the guidelines with which clinicians are faced can be overwhelming in terms of having time to read them and assimilate into clinical practice(Slade, et al., 2016, p809)32
Financial factors were the most cited barrier in six articles and included lack of reimbursement from third party insurance providers; lack of financial support to conduct testing; and the cost of rapid testing (Tan & Black, 2019, p4)35
Enablers
The commonly reported enablers were identified from nine reviews,27–30 34–38 which were increasing capable healthcare providers and managers38; increasing technical support and assistance such as establishing electronic payment system,27 health records,28 disease management plan,28 flexible booking system37 and integrated systems of collaboration promotion between PCPs and other professionals (eg, specialists, distant health professionals)30 36; financial support such as federal funding35; clearly and easily accessible health networks like multidiscipline corporations29; effective interprofessional communication through standardised care pathways30 35; incorporating CPGs recommendations into current clinic workflow28 35; and a clear leadership structure for the CPGs implementation.35 38
The use of computers, particularly the adoption and implementation of electronic health records (EHRs) can facilitate adherence to the use of asthma management guidelines. The technological system can be used to remind physicians when certain patients’ require asthma care. The system can be used in the development of asthma management plans and management of asthma prescription and medication activities. Technological systems can also be used to promote patient’s education by distributing educational materials electronically,(Ezeani, 2016 p96)28
Guideline itself related factors
Barriers
This category emerged from nine reviews27 28 30–35 37 with the number of included studies ranging from 8 to 35. Perceived limited applicability of the CPGs in real-world situations28 32–34; lack of clarity or specificity of CPGs27 30; not suitable for some specific patients like those with comorbidities30 33 and conflicts between the guideline recommendations and the commonly used medical heuristics28 34 were the frequently mentioned barriers in relation to the guidelines. Some other identified barriers were frequent change of the CGPs30; perceived limited credibility of the CPGs28 31 32; depersonalised and invalidated guidelines within specific context37; the guideline can restrict current clinical judgement and challenge the autonomy of PCPs,32 and complicated implementation procedures.35
Additionally, GPs felt that guidelines were rarely applicable to real-world practice (Smeets, et al., 2016, p3)33
A substantial number of studies highlighted physicians' concerns about the applicability of the asthma management guidelines in certain situations. (Ezeani, 2016, p81)28
Clinicians perceived that the guidelines lacked clarity or specificity. They indicated that there are issues with how guidelines are written, for example, the level of detail they provide and whether they are easily implementable in clinical practice”,(Egerton, et al., 2017 p631)27
Some clinicians (chiropractors, GPs, and PTs) believed that current guidelines were constraining and prescriptive, designed to control practice and subjugate clinical judgment by reducing medicine to algorithms, were autocratic in nature, and stifled professional autonomy and clinical reasoning. (Slade, et al., 2016, p807)32
Enablers
Some enablers regarding guideline itself were also identified from four28 29 32 33 reviews, which were developing tailored guideline with considering patients’ needs28; involving PCPs into guideline development process28; adopting cost-effective, time-saving and easy-to-use approaches as recommendations29; adaption and validation of the guideline within specific context33 and a good compatibility of the recommendations with current practice.32
Some GPs suggested the development of locally drafted guidelines to ensure a locality based, contextualised approach to overcome local organisational factors around the provision of specialised services and professional interactions between primary and secondary care,(Smeets, et al., 2016 p9)33
They (professionals) agreed with the LBP guidelines, found them compatible with their current practice, and believed that using them would help in preventing persistent disability (Slade, et al., 2016, p807)32
Healthcare provider-related factors
This category was clustered based on ten reviews,27 28 30–35 37 38 with the number of studies analysed in the reviews ranging from 4 to 35. Lack of relevant knowledge and skills,27 31 32 35 37 unclear role and identity for CPGs implementation,30–32 34 37 lack of self-confidence and/or self-efficacy regarding their capacity of using guideline to manage health conditions,28 37 negative beliefs towards the consequence of guideline,27 28 37 and low motivation or interests27 28 33 37 38 were the commonly reported barriers.
Knowledge and skills
Barriers
Lack of training, knowledge and skills about the CPGs content or recommended practice27 31 32 35 37 was the most mentioned healthcare provider-related barrier. In addition, lack of communication/language skills,27 31 and lack of knowledge about risk evaluation, motivational interview and counselling37 were also identified as significant barriers.
Professionals think that the curriculum in university and the pharmaceutical industry have an impact on their behavior. Lack of undergraduate training in PP&HP activities is perceived as a barrier,(Rubio-Valera, et al., 2014 p8)37
Specific gaps in provider knowledge that created barriers included lack of knowledge about CDC guidelines (Tan & Black, 2019, p7)35
Clinicians lack knowledge about recommended practice’: some clinicians' comments demonstrated that they, or their colleagues, were not familiar with specific treatments recommended in CPGs,(Egerton, et al., 2017 p631)27
Enablers
Relevant enablers were provision of timely education and training for PCPs28 30 33 35 36 to maintain their existing skills, and developing new skills and knowledge related to guideline implementation. For example, developing good communication skills to promote effective communication and rapport and trust relationships between PCPs and patients.
It has been recommended that there should be workshops and seminars for training PCPs about guideline use. (Ezeani, 2016, p93)28
To evaluate the influence of multimodal strategies including provider education, a second analysis was performed and 11 additional trials with multimodal strategies were included. The resulting overall OR was 1.34 (95% CI 1.08 to 1.65). A sensitivity analysis included only two trials with overall low risk of bias (16,47) where the effect was stated (OR 1.48; 95% CI 0.97 to 2.24). For these reasons, a moderate increase of physician adherence by strategies including provider education can be considered to be robust.,(Unverzagt, et al., 2014 p259)36
Professional role and identity
Barriers
Lack of clear delineation about the role, identity and responsibility of PCPs for CPGs implementation30–32 34 37 was the most frequently reported barrier. Misunderstanding or underestimation of the role of PCPs for disease management by other healthcare professionals30 was another barrier.
Nurses’ and physicians’ roles have evolved as diabetes care has become integrated into primary care, with nurses playing a central role. However, both physicians and nurses express uncertainty or disagreement over who is responsible for various elements of patient care,(Rushforth, et al., 2016 p e116 &e119)31
A number of barriers relating to the professional role of PC-Ps were reported. Six studies reported barriers that were related perceived misunderstanding about the role of PC-Ps in the management of CKD by other healthcare professionals (for example nephrologists). Some studies reported that general practitioners felt that other healthcare providers underestimated their role, and did not appreciate their expertise or their ability to competently manage the disease.,(Neale, et al., 2020 p6)30
Enablers
Several reviews also mentioned some facilitators within this subcategory, which were ensuring the ownership, flexibility and autonomy of the PCPs29; and well-organised practice and a clear clarification about the role of PCPs in disease management.30
A ‘bottom-up’ approach, including early engagement and collaborative working, and the ability of community nurses to tailor the innovation to meet individual needs was an important facilitator (Mathieson, et al., 2018, p7)
A facilitator is a well-organized practice where everyone knows their role regarding PP&HP and which has referral services within the practice,(Rubio-Valera, et al., 2014 p4)37
Beliefs about capabilities
Barriers
The subcategory mainly refers to the lack of self-efficacy28 and self-confidence37 of PCPs in terms of their capacities and personal experiences to deal with health problem based on patients’ experiences and needs.
Inadequate self-efficacy as a result of low confidence may result in non-adherence to the established asthma management guidelines. Four studies included in this review highlighted that this barrier impacted on preventative health education indicating that lack of self-efficacy can be a significant barrier to the adoption and implementation of the asthma management guidelines,(Ezeani, 2016 p84)28
Intrapersonal factors: ……, and their self-concept (self-confidence in their capacities and personal experiences with the problem: e.g., a smoker physician dealing with tobacco cessation or an obese nurse dealing with nutrition recommendations),(Rubio-Valera, et al., 2014 p3)37
Enablers
Within this subcategory, several enablers were identified, including sufficient training for PCPs to improve their confidence37 38; fully understanding the patients’ socioeconomic and psychological characteristics, expectations and cultural background27 32 35 37; and strength of peer learning and support.38
Papers found having structured management plans for patients, made of high quality materials provided alongside in-depth staff training, and confident staff to deliver it were key elements in the successful implementation of Collaborative Care,(Wood, et al., 2017 p39)38
Beliefs about consequences
Barriers
The barriers within this category were doubts about the effectiveness27 37; negative attitudes towards the disease and disease management27 and lack of expectation28 regarding the outcomes of using CPGs.
‘Doubts about treatment effectiveness’: a lack of belief in effectiveness or adequacy of available interventions was evident in participant quotations and in the summary of findings from two articles,(Egerton, et al., 2017 p632)27
Outcome expectancy can be described as the anticipation that certain behavior will result in a given outcome. If a general practitioner believes that a recommendation will not result in improvement of a particular outcome, there is less likelihood that the practitioner will follow the guideline recommendation. An important reason for the general practitioners nonadherence to the laid down asthma management guidelines is the belief that they will not be effective,(Ezeani, 2016 p84)28
Enablers
In this occasion, healthcare providers’ positive attitudes towards the programmes and guidelines35 was reported as one important enabler.
Attributes of providers facilitating testing included positive attitudes toward programs and guidelines. Clinician acceptance of the implemented testing program was associated with its success in a pediatric emergency department (Tan & Black, 2019, p8)35
Emotion/motivation
Barriers
Clinical inertia (eg, low motivation/interests) of PCPs28 due to reasons such as fear of damaging the patient-physician relationship and personal stress32 38 or negative emotions27 31 due to the volume of guideline were identified barriers within this subcategory.
Clinical inertia can be described as the PCPs reluctance to diverge from the established code of practice, and is usually entrenched in over-estimation of the quality of the prevailing clinical practices, personal disagreement with the recommended changes or PCPs ignorance,(Ezeani, 2016 p82)28
The professionals prefer not to implement PP&HP when they are concerned about damaging the patient-physician relationship, for instance, in dealing with issues related to alcohol consumption when this is not the motive for the consultation,(Rubio-Valera, et al., 2014 p4)37
Enablers
No significant enabler within this subcategory was identified from the included reviews.
Patient-related factors
Barriers
This category emerged from eight reviews,27 28 30–32 34 35 37 with the number of included original studies ranging from 4 to 32. The frequently mentioned barriers included lack of interest and poor adherence27 28 30 31 37; lack of knowledge and low literacy and health literacy28 30 31 35; dissonant expectations/goals with disease management27 28 32 34; misconceptions about the disease consequence30; patients’ characteristics such as psychological comorbidity,31 35 37 competing health needs and level of self-empowerment capacity35 and negative attitudes towards CPGs.31
Low patient adherence to management strategies, particularly lifestyle strategies, were reported as a common barrier (Neale, et al., 2020, p6)30
Lack of education about HIV and low literacy/health literacy also contributed to low testing rates (Tan & Black, 2019, p7)35
The data suggest that GPs are challenged by patient expectations that are not in agreement with their own views, but still influence GP management of the disease.,(Egerton, et al., 2017 p633)27
PC-P [primary care provider] felt that due to the asymptomatic nature of CKD, patients did not understand the seriousness of CKD and were unlikely to prioritise its management until the disease reached a more severe stage with symptoms,(Neale, et al., 2020 p6)30
Patients’ socioeconomic situation, occupation, carer status, comorbidities, mobility problems, polypharmacy, and self-empowerment capacity acting as barriers to care (Rushforth, et al., 2016, pe117)31
Some of the responses provided by patients/caregivers indicated that they view the asthma management guidelines as only suitable to certain patient populations, particularly those with severe asthma and youngsters being taken care of in schools. Parents/caregivers viewed asthma management plans as inappropriate or unnecessary since they had adequate knowledge on what they could do if their child’s asthma became worse,(Ezeani, 2016 p88-89)28
Enablers
Some of the enablers within this category were timely education and training for patients27 28 35 36; use of appropriate education materials that can be easily understood by patients38; patient’s appropriate expectations27; alignment between CPGs recommendations and the views of PCPs and patients.34
We state a moderate increase of physicians’ adherence (on guideline implementation) by strategies including patient education (Unverzagt, et al., 2014, p259)36
Behavioural regulation and reinforcement
Barriers
The barriers within in this category were mainly related to inadequate reinforcement for the implementation behaviours,30 34 37 for example, lack of remuneration, rewards or incentivisation.
the way in which practices were rewarded and incentivized for meeting Quality and Outcomes Framework (QOF) targets, significantly affected their prioritization of workload and desire to implement best practice for a condition that produced no financial gain,(Swaithes, et al., 2020 p106)34
Enablers
Several enablers were identified, which included regular supervision schedules and feedback38; appropriate follow-ups38; continuous audit programmes28; using reminder systems36 37; and appropriate remuneration28 and financial incentives.37
Audit and feedback (A&F) is a continuous improvement initiative that can be used to evaluate performance and present reports that reflect on the status of guideline use. It was suggested that this process can result improved asthma care by modifying clinical practice behavior in primary care settings,(Ezeani, 2016 p95)28
Discussion
Summary of the findings
To our best knowledge, this is the first overview of SRs that aim to explore the barriers and enablers to implementing CPGs in primary care. Numerous barriers and enablers were identified in this overview by synthesising 12 SRs with 275 original studies, which could provide evidence for the development of a theoretical basis for creating CPG implementation strategies in the primary care setting. Barriers related to ‘healthcare provider-related factors’ were most commonly reported, particularly a perceived lack of knowledge and skills about CPGs, which was followed by ‘institutional environment and resources factors’ (time constraints), ‘patient-related factors’ (poor motivations and adherence), ‘guideline-related factors’ (poor applicability of CPGs in real-world practice), ‘political, social and culture factors’ (suboptimal healthcare networks and interprofessional communication pathways), and factors about ‘behavioural regulation and reinforcement’ (inadequate reinforcement, eg, remuneration). The study findings were supported by a previous overview conducted by Correa et al,19 which examined the barriers of CPGs implementation by including studies in different levels of care (primary, secondary and tertiary care). In Correa et al’s study,19 five categories of barriers were identified except for the category of ‘behavioural regulation and reinforcement’. Changes in individuals’ behaviours are important requirements for new practice implementation.24 According to the Theoretical Domains Framework for implementation research,24 behavioural regulation and reinforcement are important contributors to changing individuals’ behaviours. Presence of technical support (‘institutional environment and resources factors’), and timely education and training for PCPs (‘healthcare provider-related factors’) and patients (‘patient-related factors’) were identified as frequently reported enablers in primary care, which was also consistent with the enablers identified in other levels of care such as secondary and tertiary care.19
For the detailed barriers within each category, some findings in this overview were in line with Francke et al’s13 and Correa et al’s overview.19 For example, time constraints and heavy workload of the healthcare providers, poor interprofessional coordination and communication, limited availability of resources, CPGs lack of clarity, conflicts between guidelines and PCPs, lack of knowledge and skills, unclear role and identity of PCPs, poor health literacy of patients, language and culture diversities, patients’ dissonant expectations for disease management, and patients’ negative attitudes towards CPGs. All of which indicated that some barriers commonly existed in different levels of care as both Francke et al’s13 and Correa et al’s study19 were not primary care focused. Those identified similar barriers highlighted opportunities for developing strategies (eg, integrated care pathways) that can be adopted by different levels of care to promote the management of patients’ health conditions across primary, secondary and tertiary care. This overview also found some barriers that were not specified in Francke et al’s13 and Correa et al’s studies,19 such as limited healthcare networks, uneven health resources distributions, limited technical support, limited services for specific patient groups or needs, conflicts views between the public and CPGs recommendations, limited applicability of the CPGs in real-world situations, PCPs’ negative attitudes towards the consequences of CPGs, and inadequate reinforcement such as remuneration, rewards and incentivisation. Those specific barriers identified within primary care highlighted potential opportunities and implications for developing tailored and effective strategies to promote the implementation of evidence-based recommendations and health services into primary care practice. More specific implications are detailed in the section of implication for CPGs implementation in primary care and future research.
Quality of the evidence
Although the quality of the included reviews was generally appraised as robust, there were still some methodological limitations in some of the included reviews. Identification of all eligible studies through rigorous and comprehensive search strategies is an important feature of high-quality SRs.39 However, 4 out of the 12 included reviews did not clearly present the detailed search strategies, which make it difficult to determine whether the used search strategies were appropriate or not. Quality appraisal and data extraction of an SR are required to be conducted by multiple individuals independently to minimise bias and errors.39 However, several reviews failed to report whether the quality appraisal (n=5/12) and data extraction(n=3/12) were conducted by two or more independent reviewers. Guidelines such as the PRISMA guidelines22 should be used in future to improve the reporting quality of SRs in this area.
Implications for CPGs implementation in primary care and further research
Political and institutional barriers, such as limited healthcare networks, poor interprofessional communication and referral pathway, limited availability of resources and uneven health resources distributions, could be improved via the strategy of ‘strengthening organisational governance arrangements’ (p.9).19 Insufficient physical preparation and resources as the frequently reported barriers indicated that, prior to the implementation of CPGs, organisations’ relevant physical situations and resources need to be fully investigated via approaches like comprehensive surveys or deep communications to ensure that the organisation is physically well prepared.38 Care models such as GP-led and shared care models40 that can highlight the leading role of PCPs in CPGs implementation and the importance of multidisciplinary collaborations between different care levels could be considered to improve the PCPs’ recognition of their role, identify and responsibility for CPGs implementation. In addition, given barriers like the financial burden and PCPs shortage were prominent and frequently reported, smooth integration of the CPGs recommendations into existing care models should be considered to minimise the additional burden on the health system and PCPs. In addition, to address the issue of time constraints of PCPs, the low efficient communication between PCPs and patients should be recognised, which could be improved via communication skills training and technical support such as an electronic disease management plan,30 flexible booking system37 and integrated systems of interprofessional collaboration promotion.30 36
For barriers like language and culture diversities, the importance of needs assessment should be recognised particularly the culture and language-specific needs of minorities, which can facilitate more individualised and cultural-based recommendations that are tailored to the minorities. Providing necessary language support services could be an important strategy to overcome the language barrier. Disconnections between the guideline recommendations and ‘real’ clinical practice (applicability issue) were identified as one of the frequently reported barriers, which could be partly addressed by using a collaborative model of codesign and coproduction (involving clinical personnel and end-users such as PCPs, managers, patients in the guideline development process).41 In addition, a detailed description of the recommendations such as the dosage of the intervention (frequency, intensity and duration) could be another strategy to overcome the barrier of lack of clarity, specificity and applicability of CPGs.27 30 The collaborative partnerships between researchers and clinical personnel and end-users can transcend the boundaries between research and real world, as well as promote the compatibility of the recommendations with real practice.34 42 Moreover, the specific context that the guideline would be implemented in should be fully considered,33 and necessary adaption and validation are needed to guarantee success and sustainability. Appropriate recommendations used in GPGs need to be determined based on not only its therapeutic effects but also the characteristics of cost-effective and time-effective, clinical utility and convenience.29 Evidence resources of each recommendation should be clearly presented to increase the credibility of the guidelines.31 Guideline reporting checklist, such as Reporting Items for practice Guidelines in HealThcare and Appraisal of Guidelines, REsearch and Evaluation II assessment tool,43 can be used to ensure the guidelines are reported in a clear, structured and easy-to-understand manner.
Some barriers that were related PCPs and patients, including inadequate knowledge and skills, lack of self-confidence, negative attitudes towards the consequences of guidelines, and low motivation and interests, low health literacy, and inconsistent expectation between PCPs and patients, could be well addressed through timely and adequate education and training. To improve the PCPs’ adherence to guideline-related training and education, relevant education and training contents can be incorporated into existing education programmes such as the annual continuing professional development programmes for PCPs. As suggested by previous research, a lack of knowledge and skills can make PCPs feel underprepared27 for using guidelines to manage patients’ health issues, which can further decrease their confidence and interests in using guidelines. Adequate education and training can help PCPs have a better understanding of the advantages of evidence-based recommendations and a more positive attitude towards the CPGs. A greater familiarity with guidelines can contribute to stronger confidence and higher adherence to recommendations.44 Also, adequate knowledge and skills can promote effective conversations among PCPs and patients, which are vital in ensuring the delivery of high-quality care and the establishment of good patient–clinician relationship. Digital technology can be used to promote education and training such as distributing educational sessions and materials electronically, which is much more convenient particular for PCPs and patients who live in rural areas without easy access to face-to-face healthcare resources.45 Given that changes of individuals’ behaviours are usually required when implementing new practices,24 strategies such as regular supervision schedules with feedback,38 continuous practice audits28 36 and appropriate remuneration28 and financial incentives37 could be considered to reinforce the PCPs and patients’ behaviours change and the sustainability of their adherence to the CPGs.
Although the above-mentioned implementation strategies were proposed based on the current literature and the identified enablers of CPG implementation in this current study, the CPG researchers, users and implementers should be aware that well-constructed empirical studies are still needed to further confirm the effectiveness of the potential strategies. In addition, whether a combination of implementation strategies (multifaceted strategies) is more effective than specific single strategies is worth further exploring as well in future research.
Study limitations
As most of the included SRs identified the barriers and enablers from the perspectives of PCPs only, more studies from the perspectives of patients in primary care can be conducted in future. Findings of this overview, to some extent, are difficult to be generalised to one specific type of health condition given that the included reviews focused on a wide range of health conditions and subgroup analysis based on the type of health conditions were not conducted due to the limited number of included studies and the variety of health conditions of the included studies. Different methods of barriers classification are another major challenge for categorising the barriers into predefined categories in this overview. For instance, in Ezeani’s study,28 time constraint was categorised as a barrier related to healthcare professionals, while it was coded as an institutional and resources-related factor in Neale et al’s study.30 Language bias was also a concern to hinder the generalisability of the study findings, as only English papers were included.
Conclusion
This study identified a wide range of barriers and enablers to implementing CPGs recommendations in primary care settings. Given that the barriers involve different levels (healthcare system, organisational and individual level), policy-driven strategies should be developed to motivate different levels of implementation activities, which could include optimising resources allocations, promoting integrated care or other new care models, establishing well-coordinated multidisciplinary networks, increasing technical support, encouraging PCPs and patients’ engagement in guideline development, standardising the reporting of guidelines, facilitating education and training, and increasing motivations via incentives. All the implementation strategies need to be conducted based on a full consideration of the social, cultural and community contexts to ensure the success and sustainability of CPGs implementation. Well-constructed empirical studies are also needed in future to further confirm the effectiveness of all the potential strategies.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors TW contributed to the study conception and design, literature search, data extraction, data analysis and manuscript drafting and revision; J-YBT and X-LL contributed to the study conception and design, data extraction, data interpretation and manuscript revision; IZ contributed to the study conception and design, data interpretation and manuscript revision.
Funding This study was supported by the Charles Darwin University (CDU) Institute of Advanced Studies (IAS) Rainmaker Start-Up Grant, and the COVID-19 Supplementary Funding Pool (CSFP) Research Fund Scheme.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.