Article Text

Abstract
Background Concepts of moral distress (MD) among physicians have evolved and extend beyond the notion of psychological distress caused by being in a situation in which one is constrained from acting on what one knows to be right. With many accounts involving complex personal, professional, legal, ethical and moral issues, we propose a review of current understanding of MD among physicians.
Methods A systematic evidence-based approach guided systematic scoping review is proposed to map the current concepts of MD among physicians published in PubMed, Embase, PsycINFO, Web of Science, SCOPUS, ERIC and Google Scholar databases. Concurrent and independent thematic and direct content analysis (split approach) was conducted on included articles to enhance the reliability and transparency of the process. The themes and categories identified were combined using the jigsaw perspective to create domains that form the framework of the discussion that follows.
Results A total of 30 156 abstracts were identified, 2473 full-text articles were reviewed and 128 articles were included. The five domains identified were as follows: (1) current concepts, (2) risk factors, (3) impact, (4) tools and (5) interventions.
Conclusions Initial reviews suggest that MD involves conflicts within a physician’s personal beliefs, values and principles (personal constructs) caused by personal, ethical, moral, contextual, professional and sociocultural factors. How these experiences are processed and reflected on and then integrated into the physician’s personal constructs impacts their self-concepts of personhood and identity and can result in MD. The ring theory of personhood facilitates an appreciation of how new experiences create dissonance and resonance within personal constructs. These insights allow the forwarding of a new broader concept of MD and a personalised approach to assessing and treating MD. While further studies are required to test these findings, they offer a personalised means of supporting a physician’s MD and preventing burn-out.
- medical education & training
- mental health
- education & training (see medical education & training)
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The systematic evidence-based approach (SEBA) methodology allows study of data from diverse methodological sources, settings, physician populations and specialties.
The SEBA methodology adopts the structure of systematic reviews and flexibility of narrative reviews to synthesis a reproducible and accountable evaluation of all sources of data.
The clinically evidenced ring theory of personhood (RToP) allows the transparent, reproducible and personalised analysis of concepts of moral distress (MD) among physicians.
Use of the RToP and the SEBA methodology to study MD is novel and require further study.
Introduction
Care and resource limitations and concerns over compromised patient care amidst the COVID-19 pandemic have fanned reports of moral distress (MD) among healthcare professionals (HCPs) in medicine, pharmacy, allied health, psychology and social work.1–11 However, while this increase in reports of MD is unsurprising, the diverse nature of accounts of MD among HCPs suggests that concerns extend beyond Jameton’s original notion of psychological distress caused by being in a situation in which one is constrained from acting on what one knows to be right.6–11
With data suggesting that concepts of MD may also differ between HCPs by virtue of their practice and settings, we focus on the study of MD as conceived by physicians. Indeed, current accounts of MD among physician12–27 suggest MD is a product of conflicts between prevailing values, beliefs and principles (personal constructs) drawn from self-concepts of personhood and ethical, practical,28 29 clinical, moral30 and professional31 influences within a particular setting or clinical interaction (situational constructs). To better appreciate conflicts between personal and situational constructs that predispose to burnout and compromised patient care a holistic appreciation of MD among physicians is required. It is hoped that better understanding of MD among physicians will help direct personalised, appropriate, timely and holistic support to physicians facing MD and thwart threats of burn-out and resignations among physicians.
Rationale for this review
A systematic scoping review (SSR) is proposed to map the diverse conceptions of MD among physicians. Indeed, the notion that MD may take a different shape among physicians than across other HCPs may not be surprising given that Jameton’s original concept was conceived within the nursing setting replete with its hierarchical and practice culture.6 A specialty-specific account of MD will guide timely, comprehensive, and personalised appraisal, and support for physicians in need.
Theoretical lens
Two considerations guided the selection of an appropriate theoretical lens for this review. One, MD is a sociocultural construct deserving of holistic study of the physician’s practice, cultural, social, professional, academic and research circumstances including their healthcare and education systems.2 32–34 Acknowledging MD as a sociocultural construct35 underlines the need to consider the individual physician’s moral, ethical and professional beliefs, values, and principles that underpin their thinking, attitudes, decision-making and actions.36 There must also be due consideration of their spiritual, emotional, relational and social considerations which similarly impact their sensitivity or awareness of occurrences and circumstances that could provoke MD in them. In addition, recognising MD’s complex sociocultural nature underscores the importance of appreciating the physician’s narratives, competencies, experiences, reflections, abilities and available coping and support mechanisms that provide MD with its personalised and evolving nature.
Two, with a physician’s personal, moral, ethical and professional beliefs, values, and principles informed by their self-concepts of identity and personhood or ‘what makes you, you’,36 the link between personalised concepts37–39 of MD and self-concepts of personhood become clearer. Ho et al38 Kuek et al3 Chan and Chia40 and Huang et al41 provide clinical evidence of these ties between self-concepts of personhood and identity using the ring theory of personhood (RToP) to study the experiences of physicians, nurses and medical students caring for terminally ill patients and confronting the death of their patients. Similarly Ho et al’s42 study of how senior palliative care and oncology nurses at a cancer centre cope with caring for dying patients and their distress in facing the death of their patients, suggest that psychological distress akin to recent accounts of MD may be better understood through the employ of the RToP framework.3 38 40 41
These two considerations underpin the reason for the employ of the RToP as the theoretical lens for this review.
The Ring Theory of Personhood
The RToP suggests that personhood is made up of four domains. These domains include the (1) innate ring, (2) individual ring, (3) relational ring and the (4) societal ring as shown in figure 1.36 Each ring contains a set of beliefs, values, principles, thoughts, attitudes, familial customs, cultural norms, roles and responsibilities that gives rise to corresponding identities. Though each of these identities is unique, how they are manifest in different settings and circumstances is dependent on the individual underlining the need to appreciate better the context and setting and the physician’s particular circumstances (figure 1).

Ring theory of personhood.
The innate ring builds on the notion that all human beings are deserving of personhood ‘irrespective of clinical status, culture, creed, gender, sexual orientation, religion, or appearance’ by their genetic propensity to being a human and or their divine connections.36 38 The innate ring gives rise to the Innate Identity that consists of one’s religious, cultural and societal-inspired values, principles and beliefs.3 19 26 30 43–45 These values dictate the individual’s perspective and expectations on care determinations, end-of-life care and withdrawing and withholding treatment.28 29 46
The individual ring represents the features of conscious functions, including their thoughts, feelings, actions and abilities.36 The identity formed within the individual ring is informed by the values, beliefs and principles based on conscious function and the other three rings. Balancing these factors in the face of perceptual, experiential, psychoemotional and contextual considerations; prevailing ethical, moral, legal, professional and sociocultural factors; as well as personal choices, biases and decision-making styles reveals the influence of individual circumstances, choices, values, beliefs, principles, biases, norms, mores and preferences. It also demonstrates that self-concepts of personhood and identity are deeply intertwined and highly individualised.
The relational ring comprises the close personal relationships that individuals hold dear to themselves. This may include family, friends and colleagues who play a vital role in their lives.36 The Relational Identity is shaped by the individual’s values, beliefs and principles derived from the nature, values, effects and ramifications of these relationships.46 47
The societal ring is the outermost ring that contains the Societal Identity formed by how the individual views their societal position, roles and responsibilities and societal expectations, professional standards and the norms, laws, and obligations of the roles that the individual plays.36
Kuek et al note that disharmony and dyssynchrony arise when values, principles and beliefs introduced within a ring or between the different rings are in ‘tension’ with current concepts, values, principles and beliefs driven by prevailing concepts of personhood. If disharmony and dyssynchrony are not addressed appropriately, timely and in a personalised manner distress can arise. It is posited that when the sources of disharmony and dyssynchrony are understood, the means to resolve MD become clearer.3 36
Methodology
Krishna’s systematic evidence-based approach (SEBA) is adopted to guide this SSR (SSR in SEBA) is used to map what is known about MD on physicians.48–51 This SSR aims to identify existing information, key characteristics and knowledge gaps in the concept of MD in current literature. This SSR in SEBA’s constructivist ontological perspective and relativist lens recognises MD as a sociocultural construct.52–55 It also facilitates the systematic extraction, synthesis and summary of application and actionable data across a variety of study formats and overcomes the absence of a common understanding of MD.
To provide a balanced review, this SSR in SEBA is overseen by an expert team comprised of medical librarians from the Yong Loo Lin School of Medicine (YLLSoM) and the National Cancer Centre Singapore (NCCS), and local education experts and clinicians at NCCS, the Palliative Care Institute Liverpool, YLLSoM and Duke-NUS Medical School. The expert team guide, oversee and support the 6 stages of SEBA to enhance the reproducibility and accountability of the process.3 38 48–51 56–62
The SEBA process comprises of six stages, namely—(1) systematic approach, (2) split approach, (3) jigsaw perspective, (4) funnelling process, (5) analysis of data and non-data-driven literature and (6) discussion (figure 2).

SSR in SEBA process. SEBA, systematic evidence-based approach; SSR, systematic scoping review.
Stage 1 of SEBA: systematic approach
Determining the title and background of the review
Guided by the expert team, the research team curated the primary research question to be ‘How do physicians conceptualise MD?’. The secondary research questions were ‘What are the characteristics of MD?’, ‘What are the sources and consequences of MD on physicians?’ and ‘What are the tools and interventions used to assess and manage MD on physicians?’. These questions were designed based on the population, inclusion criteria and exclusion criteria (PICo), and were guided by the Preferred Reporting Items for Systematic review and Meta-Analysis Protocols (PRISMA-P) checklist.63 64
Inclusion criteria
The PICo format (table 1) was employed to guide the research process.
PICo, inclusion criteria and exclusion criteria applied to database search ring theory of personhood
Searching
Twelve members of the research team carried out independent searches that were conducted on seven bibliographic databases (PubMed, Embase, PsycINFO, Web of Science, SCOPUS, ERIC and Google Scholar) between 17 December 2021 and 17 January 2022. The search process was guided by three experienced senior researchers who are well-versed in the use of the SEBA methodology and SSRs. Each senior researcher met with a team of four medical students to guide them on the search of the seven databases. This method was adopted to facilitate the training of amateur researchers and ensure that at least two independent teams were reviewing each database. Each team met regularly to discuss their findings. The senior researcher and medical students met online to compare their findings of the first 100 articles on their assigned database. Following this, teams met at specific time points after reviewing a predetermined number of included articles. Concerns and opinions were exchanged while simultaneously advancing the team’s knowledge of the area of study and the research process. Interrater reliability was not evaluated.
In keeping with Pham and Raji’s recommendations, searches were restricted to articles published from 1 January 1990 to 31 December 2020 to sustain the research process and adapt to existing time and manpower limitations.65 Quantitative, qualitative and mixed research methodologies that met the inclusion criteria were included. The full search strategy can be found in online supplemental material A.
Supplemental material
Extracting and charting
Each team reviewed the titles and abstracts and discussed their findings at regularly scheduled meetings. The teams employed Sandelowski and Barroso’s ‘negotiated consensual validation’ to achieve consensus on the final list of titles to be reviewed.66 67 The teams repeated this process independently. They studied all the full-text articles on the final list of titles and curated their list of articles to be included. The findings were then discussed via online meetings and consensus was achieved on the final list of articles to be analysed.
Stage 2 of SEBA: split approach
To enhance the reliability of the data analysis, the ‘split approach’ was used.65–71 Three groups of researchers analysed the included articles independently.
The first team summarised and tabulated the included full-text articles in keeping with recommendations set out by Wong et al’s RAMESES publication standards and Popay et al’s ‘Guidance on the conduct of narrative synthesis in systematic reviews’.72 73 The tabulated summaries functioned to ensure that important elements of the articles were not lost (online supplemental material B).
Supplemental material
Simultaneously, the second team analysed the included articles using Braun and Clarke’s approach to thematic analysis.74 In phase 1, the team conducted independent reviews and ‘actively’ read the included articles to find meaning and patterns in the data. In phase 2, ‘codes’ were constructed from the ‘surface’ meaning and collated into a codebook to code and analyse the rest of the articles using an iterative step-by-step process.75 As new codes emerged, these were associated with previous codes and concepts. In phase 3, an inductive approach allowed themes to be ‘defined from the raw data without any predetermined classification’.76 In phase 4, the themes were refined to best represent the entire data set and discussed. In phase 5, the research team discussed their independent findings and employed ‘negotiated consensual validation’ to determine the final list of themes (online supplemental material C).67
Supplemental material
The third team employed Hsieh and Shannon’s approach to directed content analysis to analyse the included articles.77 This involved ‘identifying and operationalising a priori coding categories’.77–82 In the first stage, the team drew categories from ‘Understanding the fluid nature of personhood—the RToP’ to guide the coding of the articles in the next stage.36 Any data not captured by these codes were assigned a new code (online supplemental material C).81
Stage 3 of SEBA: jigsaw perspective
The expert and research teams reviewed the categories and themes as part of SEBA’s reiterative process. The themes and categories were viewed as pieces of a jigsaw puzzle that saw overlapping/complementary pieces combined to create a bigger piece of the puzzle referred to as themes/categories.
The jigsaw perspective employed phases 4–6 of France, Uny’s adaptation of Noblit, Hare’s seven phases of meta-ethnography to create themes/categories.83 84 In keeping with phase 4 of France, Uny’s approach, the themes and categories identified during the split approach were grouped together according to their focus. These groupings of themes and categories were then contextualised through the review of articles from which they were drawn from. As per France, Uny’s approach, reciprocal translation was used to determine if the themes and categories could be used interchangeably.
Stage 4 of SEBA: funnelling
As per phases 3–5 of France’s approach, the funnelling process begins with juxtaposing the themes/categories identified in the jigsaw approach and the key messages identified in the tabulated summaries to create domains.83 The funnelled domains created from this process forms the basis of the discussion’s ‘line of argument’ in stage 6 of SEBA.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this study.
Results
A total of 30 156 abstracts were identified from 7 databases, 2473 articles were reviewed and 128 articles were included as shown in figure 3.

Preferred Reporting Items for Systematic review and Meta-Analysis (PRISMA) flow chart.
The jigsaw process saw the themes identified which were characterisation, causes, influences, impacts, tools and interventions of MD combined with the categories identified which were the innate ring, the individual ring, the relational ring, the societal ring, disharmony and dyssynchrony. The five funnelled domains identified were as follows: (1) current concepts, (2) risk factors, (3) impact, (4) tools and (5) interventions.
The five funnelled domains provide a clinical depiction of current reports of the physician’s experience of MD and addresses the paucity of knowledge of MD through the lens of the RToP.
Domain 1: current concepts
Some included articles adopt Jameton’s definition, which assumes the physician has knowledge of the right course of action but is unable to follow through with that course of action.1 2 32 34 85–164
Most included articles however chose to adapt Jameton’s definition, due to contextual165 166 and practice differences between nurses and physicians.89 99 106 113 Greater awareness of MD, a general frustration with the medical hierarchy that often does not consider a nurse’s view or limits their input in care determinations2 98 119 124 129 161 167 and the presence of support mechanisms168 also encouraged nurses to report more episodes of MD2 85 88 89 98 99 112 116 119 121–126 129 161 169 170 than their physician colleagues.115 116 120 159 160 167
Still other included articles afforded alternate definitions.89 99 106 113 Abbasi et al’s89 definition of MD focused on personal powerlessness to ‘preserve all interests and values at stake’. Green et al106 suggest that MD was akin to ‘an attack on one’s integrity’ and is not just about ‘feeling badly’. Varcoe et al33 acknowledge the influence of the community and institution on MD. Other reasons for a new definition for MD include acknowledging resource limitations and allocations, concerns over the quality of care, ethical dilemmas such as prognostication and end-of-life matters, and confrontations with family, patients and other HCPs.2 33 98 116 118 119 124 129 161 167
Additionally, analysis of accounts of MD through the lens of the RToP15 highlights current failures to recognise conflict between the rings of personhood (dyssynchrony) or within a ring (disharmony) as a source of MD.3 38
Dyssynchrony
Perhaps the most common source of MD is dyssynchrony. The most common form of dyssynchrony is a conflict between personal and societal expectations, values, behaviours and practices. This may be a conflict between innate and/or individual rings nd the societal ring. Another example is when the healthcare team limits or withdraws care or facilitates abortions when it runs against the physician’s religious beliefs.105 139 166 171 Similarly, Daniel’s172 experiences rationing oxygen to the ‘most medically salvageable’ patient in the ICU after the 2010 Haiti earthquake saw her question whether her decision was ‘a medical judgement based on a comorbidity or a value judgement based on (her) own latent biases’.172 These accounts underline the influence of individual experiences, upbringing, religious beliefs and sociocultural background on the occurrence and or perception of MD among physicians.
Disharmony
Accounts of disharmony often revolve around conflicts between professional obligations. de Boer et al’s study of MD found disharmony arose physicians and nurses questioned the extent of care afforded patients at a neonatal ICU and if they were an example of overtreatment by the team.116 Brown-Saltzman’s qualitative study on MD reported disharmony within the innate rings where there was a conflict between ‘sanctity of life and the sanctity of choice’ in a patient’s care.113
Domain 2: risk factors
Risk factors for MD were also identified across the rings of personhood.
Innate ring
Women are more likely to report MD and also suffer greater emotional exhaustion and ethical issues.2 88 91 107 108 132 159 173 The propensity for younger physicians to report MD may relate their limited role in care determinations and treatment decisions within the medical hierarchy.88–91 108 174
Individual ring
Personality traits and values such as a deep sense of service and caregiving, a lack of assertiveness, poor self-esteem and lack of flexibility predispose to MD.1 94 117 150 151
Relational ring
Marital conflict, family disruption and feelings of isolation from family and friends lead to a poorly supported physician at risk of MD.88 102 113 139 160 175 176
Societal ring
Contextual factors such as the employ of perceived futile care,2 97 99 100 108 115 116 120 121 130 131 134 157 161 162 167 171 177–179 resource constraints leading to prioritisation of care between patients,4 85 91 97 99 100 107 108 114 116 117 121 132 135–137 140 143 144 164 166 167 180–185 institutional rules, policies and organisational pressures that prevent physicians from providing appropriate patient care,4 85 94 99 113 114 120 124 140 147 150 151 153 166 168 175 177 180 185 186 and the disconnect between perceived ethical practice and delivered clinical practice predispose to MD.97 109 112 152 160 187
Domain 3: impact
MD often manifests as anger, frustration, sadness, depression or guilt.1 89 90 94 97 104–107 113 115 119 120 122 123 136 137 143 151 154 157 160 164 168 173 188 A sense of powerlessness and the erosion of individual values and moral integrity may culminate in the intention or act of leaving one’s job,1 94 107 113 121 129 141 143 154 164 168 189 medical errors,1 2 88 89 96 98 99 101 107 108 112 113 115–117 119–126 136 148 151 155 159 161 164 167 168 170 176 190 191 a compromise in patient care1 34 90 111 112 116 119 120 122 124 144 151 159 160 165 169 192 or the transfer of the physician’s emotions onto patients.1 85 97 102 112 119 122 129 137 141 147 149 161 164 168 Multiple unresolved episodes of MD may lead to more severe consequences.85 86
Howe; however, proposes that MD could be an ‘alarm signal’ to alert physicians to reflect, develop and engage others for guidance and support32 104 114 and trigger more inclusive discussions and the re-evaluation of care plans.34 87 98 109 111 130 138 149 158 193
Domain 4: tools
The MD Scale and its successor the Standard Hamric MD Scale-Revised (MDS-R) is the most commonly used tool to evaluate MD.1 2 85 88–91 96 99–101 103 107 108 111 115 117 120 121 127 132 142 151 155 156 160 161 165 179 192 194 These tools have been employed in clinical situations, such as end-of-life care, staffing, resources, communication and decision-making to determine the presence and extent of a physician’s MD. Other tools such as the Measure of MD for Healthcare Professionals (MMD-HP) determine the presence of MD while the MD thermometer assesses the intensity of MD.96 127 130 151 MDS-R and MMD-HP also evaluate the sources of conflict reviewing conflicts between personal and professional expectations on conduct, and professional and familial sources of MD.89 98 161 195
Domain 5: interventions
Management of MD may be categorised into individual coping mechanisms and organisational interventions. To counter negative coping strategies such as distraction and excessive alcohol consumption,97 119 132 mindfulness training, meditation, healing rituals, exercise, naming the feeling,97 119 129 132 175 189 193 rationalisation and positive reframing have employed to manage MD.87 106 126 129 153 158
Organisational interventions include team-based discussions,2 88 95 97 100 104 105 119 120 124 127 129 132 135 139 144 creating a conducive environment,158 196 increasing education and counselling,4 88–90 104 105 151 175 191 and providing an MD consultation service have been suggested.105 150
Stage 5 of SEBA: analysis of evidence-based and non-data-driven literature
The majority of included articles were data driven (83 out of 128). However, concerns that evidence taken from non-data-driven articles (position, perspective, conference, reflective and opinion papers, editorials, commentaries, letters, posters, oral presentations, forum discussions, interviews, blogs, governmental reports, policy statements and surveys) which are often neither evidenced-based nor quality assessed, could bias the discussion saw the team thematically analyse the data from data driven and non-data driven articles separately. The themes from both groups were similar emphasising that the non-data-based articles did not bias the analysis untowardly.
To further advance the transparency and accountability of this review quality appraisals using MERSQI and COREQ were conducted (online supplemental material B).197 198
Stage 6 of SEBA: synthesis of SSR in SEBA
The synthesis of the discussion was guided by the Structured approach to the Reporting In healthcare education of Evidence Synthesis statement and Best Evidence Medical Education Collaboration guide.199 200
Discussion
In answering its primary and secondary research questions, this SSR in SEBA suggests that physicians’ concepts of MD extends beyond Jameton’s notion of ‘(A) the psychological distress of; (B) being in a situation in which one is constrained from acting and (C) on what one knows to be right’.1 2 6–10 32 34 85–118 120–123 125–164 Indeed this SSR in SEBA reveals that physicians also include contextual, practice, environmental, cultural, community and institutional factors, resource limitations and allocations, quality of care and ethical dilemmas2 33 108 117 118 125 132 138 143 148 180 186 and personal factors including feelings of powerlessness and ‘attacks’ on their integrity,89 99 106 113 personal values,116 professional codes172 and existential beliefs105 139 166 171 as situational constructs that shape their personal constructs within their rings of personhood.3 38 Personal factors including gender, specialty, personality traits, principles, values, beliefs, experiences, circumstances and the availability of support mechanisms psychoemotional states, familial issues, and sociocultural factors also influences the perceptions and responses to MD.2 6–11 97 99 100 108 115 116 120 121 130 131 134 157 161 162 167 171 177–179 This combination of personal and situational constructs may explain the individual variations in the nature, intensity, duration and onset of anger, frustration, sadness, depression and or guilt1 89 90 94 97 104–107 113 115 119 120 122 123 136 137 143 151 154 157 160 164 168 173 188 and the presence of ‘distress’ even when the ‘right’ action is taken2 85 89 94 98 105 116 118 119 124 129 133 140 141 146 151 156 157 161 164 165 167 172 177 179 201 202 among reports of MD. Insights into the effects of personal and situational construct on the physician’s RToP and the resultant dyssynchrony and or disharmony also help early identification of risk factors for MD, guide personalised support, provide the selection of appropriate interventions to attenuate these issues and monitor the physician’s progress over time.
These insights allow the forwarding of a clinically relevant evidenced based definition that characterises MD among physicians as ‘cognitive, existential and or emotional distress that arises with recognition that patient care may or has been compromised. Sources of MD extend beyond organisational limitations and include dissonance between a physician’s values, beliefs and or principles and clinical, research, administrative practices that threaten the physician’s personal, professional, spiritual, moral, ethical, relational and societal identity and self-concepts of personhood. MD is also informed by individual narratives, personal characteristics, coping, abilities, reflections, emotional states, and relational, psychosocial, financial, societal and contextual considerations and circumstances’. We believe that this definition of MD for physicians and data from this SSR in SEBA allows the forwarding of a holistic and clinically relevant framework that could guide the design of a tool to better assess MD in the absence of a longitudinal assessment tool that considers environmental, contextual, experiential, personal and psychoemotional factors.32
The RToP-MD reflective tool
The data from this SSR in SEBA lays the foundation for a new approach to assessing MD. The RToP-MD reflective tool (table 2) acts as a stimulus for reflection on dyssynchrony and disharmony and personalised study of MD with a trusted and trained senior clinician. This will provide personalised and timely support to the physician as they reframe, reflect and integrate new insights into their practice (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
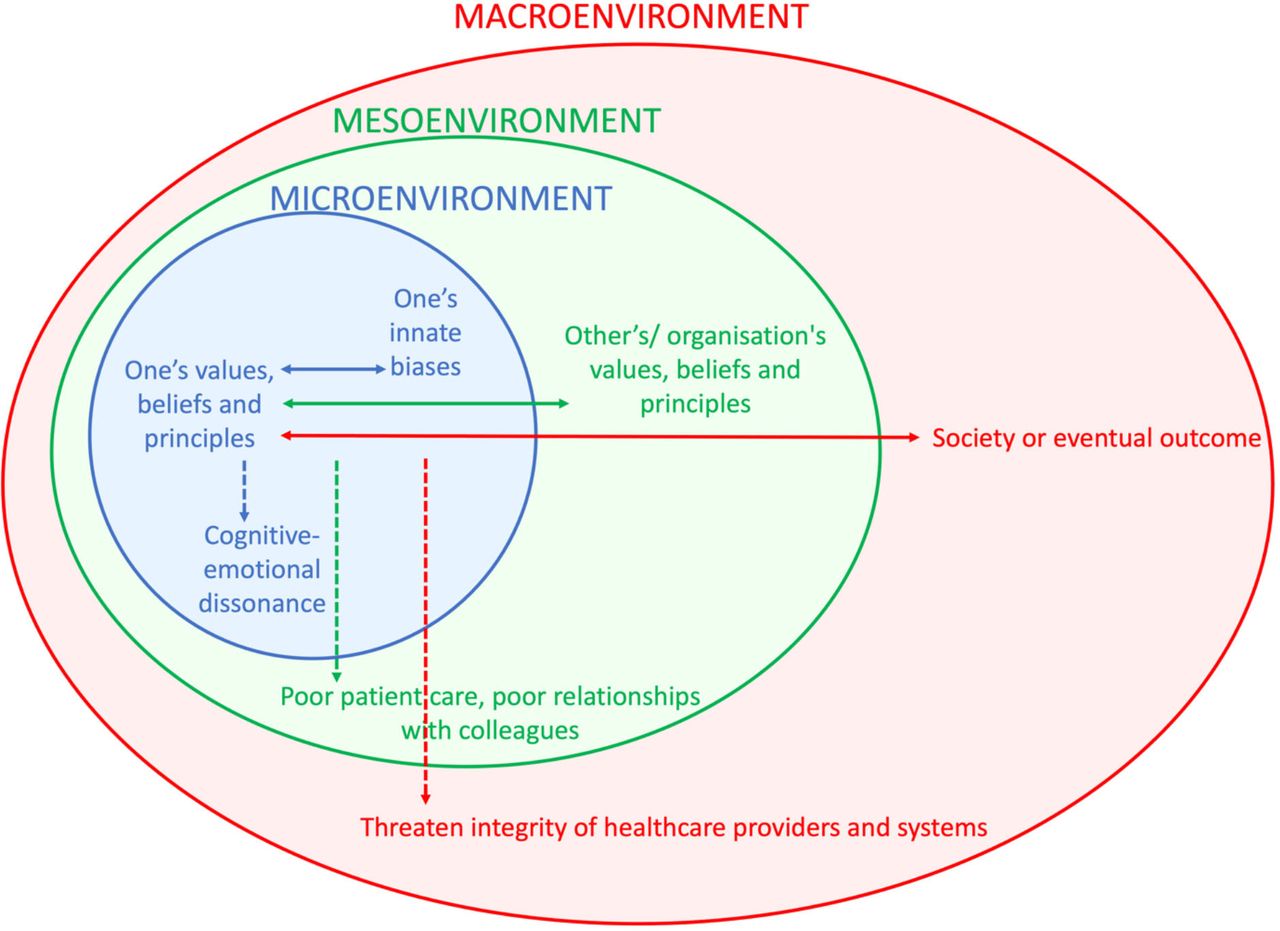
Framework to understand MD. MD, moral distress.
RToP-MD tool (with sample responses)
There are two aspects to the RToP-MD reflective tool. The first considers demographical information and the reporting of physicians’ awareness of the key issues. An example is highlighted in table 2.
The second aspect of the tool is the data collected during the interview with the trained and trusted senior clinician. This qualitative aspect of the tool focuses on the physicians personal and situational constructs through the employ of the RToP.
The data collected represented by figure 4 focuses on three domains or rings acknowledging MD as a highly individualised sociocultural construct. The outer ring represents information on the macroenvironment. This includes the practical, ethical, legal, clinical, sociocultural and professional factors that influence thinking, decision making, practice and the conduct of the physician.
Elements within the macroenvironment also influences the mesoenvironment which is the middle ring. The mesoenvironment concerns the influence of the various stakeholders, and the organisation where MD occurred. This ring also concerns itself with the individual and the contextual factors.
The innermost ring or the microenvironment is influenced and influences the two outer rings. The microenvironment considers the physician’s narratives including their previous experiences,37 demographics, training, skills, personality, attitudes, resilience, current coping, and the values, beliefs,39 and principles10 62 within each of the 4 rings of the RToP.38 This ring also considers conflicts between and within the rings of the physician’s RToP. Here, the interview process will also seek to determine the relative weight afforded to each of the competing principles by the physician.
We believe that the findings of the RToP-MD tool203 will help direct a holistic, appropriate, accessible, personalised, longitudinal and timely support to physicians from members of a multidisciplinary mentoring,204 supervision205 and or coaching team which would also include a psychologist and or counsellor.206
The proposed framework for a RToP-MD tool also serves to highlight the shortfalls of the current management of MD (online supplemental materials D and E) that tends to be singular, short term and impersonal when what is required is a holistic, appropriate, accessible, personalised, longitudinal and timely approach to overcome MD.
Supplemental material
Supplemental material
Limitations
We acknowledge several limitations to this study. Despite vetting and evaluation of the search process by the expert team, the inclusion of only English language articles and the exclusion of grey literature precipitates a risk of failing to capture important articles.3 Concurrently focusing on publications in English focuses our attention on Western practice where distinct sociocultural, practice, education and healthcare considerations may limit the applicability of these findings in settings beyond the North American and European setting.
The purposeful selection of search terms and the employment of a wide range of databases broadened our approach to obtaining essential publications. However, the inclusion of articles that explicitly mention the term ‘MD’ and exclusion of non-healthcare settings, such as war, may limit our analysis of the conceptualisation of the phenomenon.
Although the thematic analysis was conducted by independent members of the team to improve the credibility and reliability of the data, inherent bias cannot be eliminated entirely.3 In addition, meetings were conducted at various time points of the coding and analysis process to enhance the consistency and validity of the data. However, articles that conflate the findings of MD in physicians and nurses still potentiates the risk of error in data extraction despite attempts to isolate the information.
Conclusion
In forwarding an evidence-based concept of MD among physicians and an accompanying framework, and RToP-MD tool, this SSR in SEBA reveals that this richer more complex concept of MD that extends beyond Jameton’s idea that suggests that other HCPs may have their distinct concepts of MD that ought to be studied separately. Even as these findings demand more attention to the timely, context-specific, culturally appropriate and personalised identification, assessment and support of MD among physicians, similar attention is owed other HCPs. In addition, with evidence acknowledging MD as a sociocultural construct future studies ought to be appropriately situated, longitudinal and holistic.
As we look forward to continuing our discourse on MD, we hope to share our findings into the further study, assessment and validation of this new definition, framework and tool with our research, education and clinical colleagues.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants as it is a systematic scoping review. It analyses data from articles gathered from scholarly databases; no human participants were recruited in this study. Animals’ involvement: This study does not involve animals as it is a systematic scoping review. It analyses data from articles gathered from scholarly databases; no animal subjects were involved in this study.
Acknowledgments
The authors would like to dedicate this paper to the late Dr. S Radha Krishna and A/Professor Cynthia Goh whose advice and ideas were integral to the success of this review and Thondy and Maia Olivia whose lives continue to inspire us. The authors would also like to thank Alexia Sze Inn Lee for her help in searching and coding the articles and Nur Diana Abdul Rahman at the Division of Cancer Education, from National Cancer Centre, Singapore, for her contributions. The authors would also like to thank the anonymous reviewers whose comments greatly enhanced this manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CWNQ, RRSO, RSMW, SWKC, AK-LC, GSS, AYTT, AP, NB, YAW, RCHC, CYLL, KWL, GHNT, REJL, NSYK, YTO, AMCC, MC, CL, XJZ, SYKO, EKO and LKRK were involved in data curation, formal analysis, investigation, preparing the original draft of the manuscript as well as reviewing and editing the manuscript. All authors read and approved the manuscript. LKRK accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.