Article Text

Abstract
Introduction Psychology students at universities in Denmark and worldwide often receive relatively little clinical training, even though such training is crucial to job performance after graduation. Training common psychotherapeutic skills, such as being empathic and facilitating the therapeutic alliance, is critical since these skills are related to psychotherapy outcomes. In this study, a deliberate practice-based approach to student training will be compared with theoretical teaching. The main hypothesis is that deliberate practice training will result in a larger improvement in students’ observer-rated interpersonal skills.
Methods and analysis The TRaining of graduate students In general Psychotherapeutic Skills study has a double-centre, randomised, assessor-blinded, two-way crossover study design. About 200 graduate students from two Danish universities will be randomised into two groups, (a) deliberate practice training of common psychotherapeutic skills using role-play and Skillsetter, an online skill-building system with therapy videos or (b) theoretical teaching. Group a will first receive the experimental condition, followed by the control condition, while group b will receive the conditions in reverse order. Each condition consists of 15 hours of classroom participation and homework. The primary outcome is facilitative interpersonal skills—observer. Secondary outcomes include the facilitative interpersonal skills—self-report, the Counselor Activity Self-Efficacy Scales and the Interpersonal Reactivity Index. Outcomes will be measured at baseline (week 0), after the first condition (week 5; before the crossover, reflecting true randomisation) and after both conditions (week 10). Main outcome analyses will be performed at week 5. Several predictors of the effect of deliberate practice will be explored.
Ethics and dissemination Ethical approval from university ethics boards has been obtained. All participants will be asked to provide informed consent before participation. Once completed, the study can potentially transform the training of psychotherapy in graduate education, which, ultimately, may positively influence psychotherapy outcomes (IP-IRB / 03092021).
Trial registration number NCT05164497.
- EDUCATION & TRAINING (see Medical Education & Training)
- Clinical trials
- Adult psychiatry
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The study is a randomised controlled trial testing an innovative video-based approach to therapist training rooted in deliberate practice and evidence-based therapeutic factors against a control condition that consists of theoretical teaching similar to most teaching in clinical psychology at universities.
The study applies both self-report and performance-based outcome measures, which is essential because therapists are biased when evaluating their own skills and only performance-based measures are predictive of client outcome.
This study does not investigate whether improvement in therapist interpersonal skills can be transferred to face-to-face clinical situations and enhances client outcome, which is the next step to be tested.
With a sample of graduate students, it is unclear whether the results can be generalised to more experienced psychotherapists.
Introduction
In their review of the training of psychotherapists, Callahan and Watkins found that evidence for current training practices was lacking, and more research was warranted.1 Moreover, psychotherapists do not seem to become more effective due to accumulated clinical experience alone.2 3 Other studies have questioned whether supervision helps psychotherapists improve.4 Accordingly, the evidence for the effect of clinical training is limited or conflicting, and a thorough reconceptualisation of how we train psychotherapists is needed.
To identify the skills that should be trained, psychotherapy factors essential for psychotherapy outcome are a good starting point. In the traditional medical model, mental disorders are assumed to have disorder-specific causes and maintaining factors, targeted and treated with specific interventions in manualised treatments. It is further assumed that psychotherapy operates through therapeutic change factors specific to a particular treatment approach.5 However, these assumptions have been questioned because even though several specific psychotherapy methods are effective for specific disorders, differences in efficacy between well-established methods are typically negligible.6 7 Furthermore, studies have generally found no or very modest associations between specific therapeutic techniques and outcomes.8–10
An alternative conceptualisation of the effective factors in psychotherapy focuses on therapeutic factors, which are non-specific or common across therapeutic approaches. Research documents the impact on psychotherapy outcome of common factors, such as empathy and the therapeutic alliance across all mental disorders and psychological problems.11 12 Moreover, mastery of these common factors is a prerequisite for implementing the specific factors. Studies further indicate that the individual psychotherapist is more important for the outcome of psychotherapy than the specific therapeutic approach. For example, a meta-analysis by Baldwin and Imel found that the therapist effect explained, on average, 5% of the variance in outcome (compared with around 1% for the specific factors).13 Hougaard reviewed the research on therapeutic factors and concluded that the most effective therapists are distinguished by excellent interpersonal skills, or what Norcross and Lambert have named ‘evidence-based relationship skills’.14 15 These relationship skills include empathy, the ability to establish a therapeutic alliance, repairing alliance ruptures and obtaining feedback on the effect of the interventions. Other common competencies include the ability to formulate a case-conceptualisation and a compelling rationale for the treatment. A promising line of research has operationalised eight types of facilitative interpersonal skills (FIS): (1) Verbal fluency, (2) hope and positive expectations, (3) persuasiveness, (4) emotional expression, (5) warmth, acceptance and understanding, (6) empathy, (7) alliance-bond capacity and (8) alliance rupture‐repair responsiveness.16 Three studies found that therapist observer-rated FIS predicted client symptom change.17–19
If common competencies are crucial to the efficiency of psychotherapists, it is critical to identify the most efficient way to train and improve these competencies. However, in Denmark and other countries, undergraduate and graduate psychology students mainly read academic texts and receive limited clinical training. A study from the University of Copenhagen showed that newly educated psychologists identified an ‘ability to work with real-life problems and solutions’ as their primary deficiency after graduation.20 This corresponds to the finding that novice therapists can become emotionally overwhelmed when applying theoretical knowledge to practice.21 Likewise, several researchers have highlighted the ‘theory-practice gap’, defined as the poor transfer of theoretical knowledge to clinical practice.22 Accordingly, besides teaching theoretical models of psychotherapy, training programmes should be organised to allow students to practice clinical skills.23 24 A crucial part of learning clinical skills is to obtain direct feedback from patients, fellow students and a supervisor observing the therapist.24 25 Therefore, training procedures should resemble practice as much as possible, for instance, by including feedback on role-playing or video-recorded psychotherapy.
There are already several educational programmes that systematically train psychotherapists in evidence-based relationship skills.26 Recently, several studies have found some evidence for the effectiveness of such approaches. For example, Perlman and colleagues investigated the impact of a training protocol that integrated elements of alliance-focused training (AFT) and FIS in an RCT including 58 trainees and therapists.27 They found that a 90 min AFT/FIS workshop had a small effect on the mean post-training FIS and a large effect on the specific skills targeted in training: empathy, alliance bond capacity and alliance rupture repair. Anderson and colleagues included 101 undergraduates. They found that the intervention group, which had observed model responses of good psychotherapy skills and then practiced these skills in responses to video clips, had significantly higher FIS scores than the control group,.28
A particularly promising recent approach is Skillsetter, an online system for training of psychotherapy skills developed by Wampold and coworkers.29 Skillsetter builds on the principles of deliberate practice, a concept introduced by Ericsson et al.30 Deliberate practice is grounded in research on expert performance within music, sports and chess. It is defined as individualised training activities designed to improve performance through goal setting, dividing learning objectives into smaller units, repeated practice, feedback and successive refinement of practice.31 Applying deliberate practice to psychotherapy training, Miller and colleagues specified four primary elements: (1) a focused and systematic effort to improve performance based on clear identification of learning objectives, pursued over an extended period, (2) guidance from a coach/teacher/mentor, (3) immediate and ongoing feedback and (4) ongoing, successive refinement.32 Skillsetter uses deliberate practice by letting the therapist watch a video simulating clinical challenges and then record a response to the video. Subsequently, the therapist evaluates the response by comparing it with a checklist describing a good response and gives new responses until a self-evaluated satisfactory result is achieved and recorded. Finally, a trainer evaluates the response and provides feedback allowing gradual improvements in skill acquisition,.29
One further question related to the training of therapists is to what extent aspects of the therapist’s personality and professional characteristics are related to common psychotherapeutic skills and moderate the impact of training. A recent systematic review found beginning evidence that therapists with a more affiliative (ie, self-loving) attitude towards themselves and higher levels of attachment security achieved better client outcomes.33 Furthermore, de Jong and colleagues found that the impact of client feedback was moderated by the therapists’ feedback propensity, that is, their preference for receiving feedback from others (ie, external) versus from self (ie, internal).34 Therapists with higher external feedback propensity obtained better outcomes when receiving client feedback. Likewise, de Jong and colleagues found that therapists who rate themselves high on self-efficacy obtained better results in psychotherapy informed by client feedback.34 Accordingly, receiving feedback on performance may not be equally helpful to all therapists and may be related to their specific learning preferences and self-efficacy. Therefore, insights into individual differences in the response to training and feedback are crucial for developing customised and more effective training of psychotherapist skills in the future.
Finally, it is essential to evaluate the effect of psychotherapy training programmes through performance-based measures rated by observers, in addition to self-report measures. Research has found that observer-rated measures of relational competencies can predict psychotherapists’ effectiveness with their clients, whereas self-reported relational competencies, such as empathy and self-efficacy, are often unrelated to therapists’ effectiveness.17 One reason for this discrepancy can be that psychotherapists are, in general, poor in evaluating their relational competencies. Accordingly, research employing observed-based measures of psychotherapeutic skills, such as FIS, is warranted.
Aim and hypotheses
The overall aim is to test a deliberate practice approach to improving the psychotherapeutic skills of graduate psychology students, thereby ensuring better work performance in entry-level clinical positions. The first and main hypothesis is that the students’ observer-rated performance on the FIS will improve significantly more after deliberate practice training compared with theoretically teaching. The second hypothesis is that students’ self-reported FIS, self-efficacy and empathy will increase significantly more after training compared with theoretical teaching. The third hypothesis is that students reporting higher baseline levels of self-affiliation, attachment security, external feedback propensity and self-efficacy will have a larger increase in FIS after the training programme. The fourth hypothesis is that the amount of deliberate practice will predict improvement in FIS, whereas the students’ sociodemographic characteristics, previous experience with psychotherapy and psychotherapy approach will not be associated with improvement in FIS.
Method
Participants, inclusion criteria and setting
The participants will be graduate students at two universities in Denmark, the Department of Communication and Psychology at Aalborg University and the Department of Psychology at University of Copenhagen, who are attending a 30-hour course in clinical psychology called ‘deliberate practice training of general psychotherapeutic skills’ in the autumn semesters 2021, 2022 and 2023. Approximately 70 students are expected to participate each semester. All students participating in the course are eligible for inclusion into the study, provided they give informed consent. All participants hold a BSc in psychology and have previously completed a 30-hour course in counselling or helping skills, including classroom teaching and role-play.35
Study design
The study design is shown in figure 1. The study has a double-centre, randomised, assessor-blinded, two-way crossover study design. The study’s statistician will randomise students within each study site using a random number generator with a 1:1 allocation ratio, determining the order in which the experimental and control condition will be delivered. Half of the students will first receive the experimental condition, followed by the control condition, while the other half will receive the conditions in the reverse order. By the end of the course, all students will have received the same teaching and training, in reverse order, to meet the curriculum requirements. The 70 students at each semester will be divided into groups of four to five, working together throughout both conditions, performing role-plays and giving peer feedback in the experimental condition and discussing theory in the control condition.
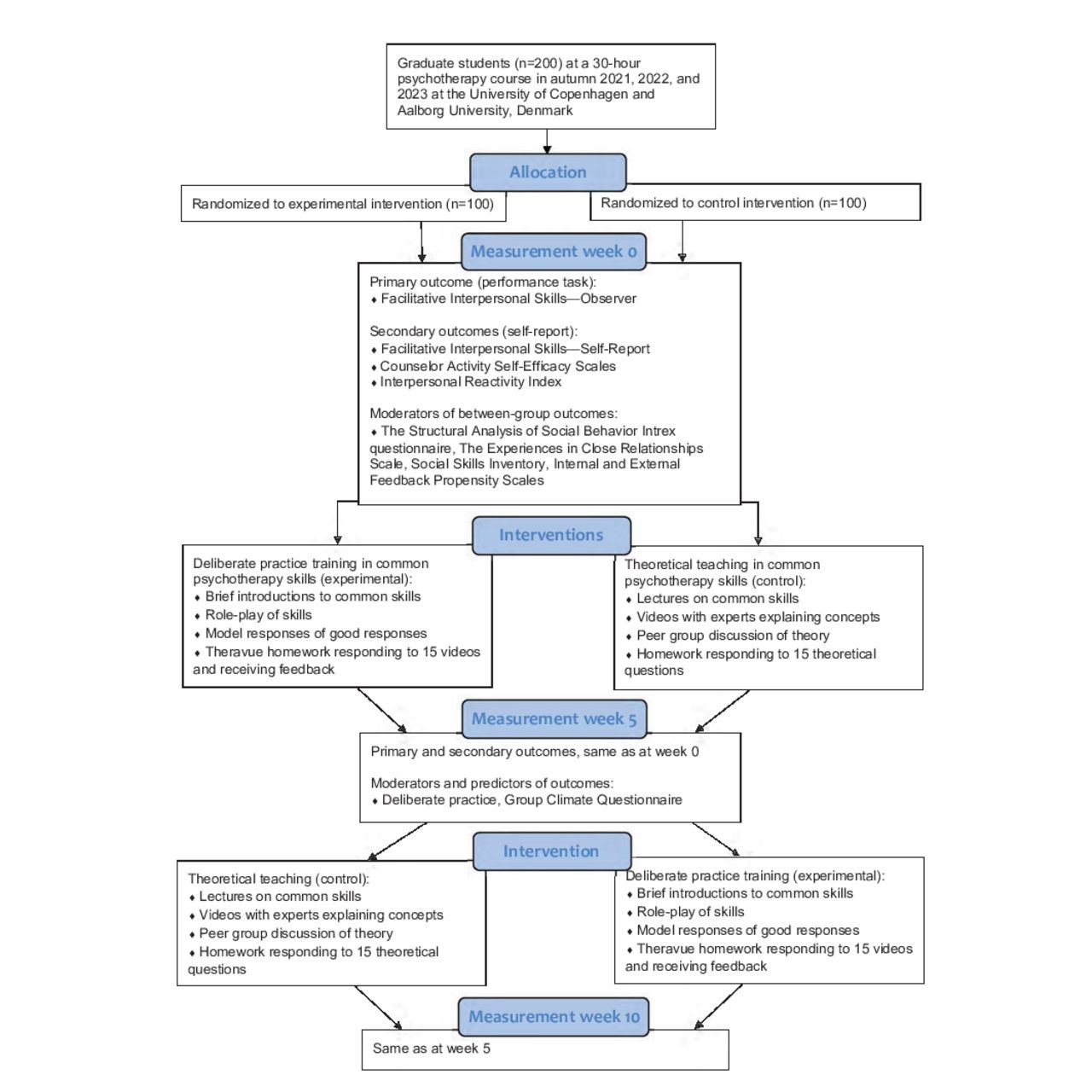
{kind=link}
Flowchart study design.
The blinding of raters will be ensured for the primary performance-based outcome by assigning the video-recorded responses randomly to the raters and concealing the group allocation (experimental vs control) and time of measurement (week 0, 5 or 10). Furthermore, analyses of outcomes and the conclusion regarding hypotheses 1 and 2 will be performed blinded to allocation (ie, results in favour of condition X or Y). Due to the nature of the intervention, it will not be possible to blind teachers and students.
The experimental and control condition
The experimental condition consists of 5 weeks of deliberate practice training of common psychotherapy skills organised as (1) classroom training and (2) homework. A clinical psychologist will lead 15 hours (5 days x 3 hours) of classroom training. Each day has a theme: (a) empathy, (b) establishing the therapeutic alliance, (c) working with alliance ruptures, (d) formulation and communication of an interpersonal focus and (e) clinical expertise—a synthesis. The training will include brief theoretical introductions, students defining individual training goals, model responses of good psychotherapeutic skills and student role-plays followed by feedback. After each of the five classes, the students will, as homework, use Skillsetter to watch and respond to three therapy videos related to the theme of the previous class. After filming and watching each response, the students will compare it to a checklist describing a ‘good response’. Subsequently, they will practice their response until they achieve a (self-rated) satisfactory result before uploading their response to receive feedback from the clinical psychologist (one video) and peer-students from their small group of four to five students (two videos). After the feedback, the students must make at least one new response to each video. Accordingly, each student will respond at least three times to 15 Skillsetter videos throughout the course. The duration of 5 weeks, including homework, was considered sufficient to allow the students to practice their skills according to the four deliberate practice principles described in the introduction.32
The control condition was created to resemble teaching in clinical psychology as it is usually conducted at universities and will consist of 5 weeks of theoretical teaching of common psychotherapy skills organised as (1) classroom teaching and (2) homework. The 15 hours (5 days x 3 hours) of classroom teaching has the same five themes as the experimental condition. Each of the five classes will consist of theoretical presentations, videos with master therapists defining core concepts and small-group discussions of literature and will not encompass training of psychotherapeutic skills. Homework will consist of students reading literature and using a restricted version of Skillsetter to record answers to three theoretical questions related to the theme of the preceding class.
Measures
Therapist primary outcome
FIS—Observer measures relationship skills exhibited in psychotherapy,.16 The students respond as helpfully as possible to video clips simulating challenging therapy situations. FIS has eight dimensions: (1) verbal fluency, (2) hope and positive expectations, (3) persuasiveness; (4) emotional expression; (5) warmth, acceptance and understanding; (6) empathy; (7) alliance-bond capacity and (8) alliance rupture‐repair responsiveness. The items are rated on a 5-point Likert scale from 1=skill deficit to 5=optimal presence of skill. FIS has a high inter-rater agreement and excellent internal consistency (α>0.91).18 36 In the present study, three different sets, each consisting of three FIS videos, will be presented to each student three times in randomised order: at baseline (week 0), after the first condition (week 5) and after both conditions (week 10). The three video sets will be matched according to their position within the interpersonal circumplex.37 The mean global FIS score of the three videos will be used as the outcome. The FIS scores will not be revealed to the students at any time.
The training of the raters will follow the FIS rating manual and has two steps.16 First, the raters will be trained using video clips from Timothy Anderson with examples of therapist responses at different levels of FIS scores, providing the raters with anchors to which they can compare their ratings of each FIS dimension. Second, the raters will individually rate video clips from a Danish sample not included in the present study, compare ratings and discuss any discrepancies to achieve sufficient reliability before rating the study videos.
Therapist secondary outcomes
FIS—Self-Report (FIS-SR) measures self-evaluated relationship skills.28 Following participation in the FIS task, participants rate their performance on the eight FIS dimensions mentioned above on a 5-point Likert scale ranging from 1=strongly disagree to 5=strongly agree. The FIS-SR has been used in one recent study, finding an excellent internal consistency of the measure (α=0.91) and a moderate correlation (r=0.44) with observer-rated FIS.28
Counselor Activity Self-Efficacy Scales (CASES) measure therapists’ experience of self-efficacy within various domains.38 The present study uses the 15 items measuring Helping Skill Self-Efficacy, and the 10 items measuring Session Management Self-Efficacy. Each item is rated on a 10-point Likert scale ranging from 0=no confidence to 9=complete confidence. In a study of novice counsellors, the internal consistency of the 25-item scale was excellent (α=0.96).39 The convergent validity has been supported by strong correlations with another measure of self-efficacy, and discriminant validity found support in low correlations with a scale for social desirability.38 Moreover, the CASES was sensitive to change throughout a one-semester practicum and able to differentiate among students with different levels of counselling experience.38
Interpersonal Reactivity Index (IRI) is a self-report measure of empathy, including cognitive and emotional dimensions.40 The IRI has 28 items, each rated on a 5-point Likert scale from 0=does not describe me well to 4=does describe me very well. The IRI has acceptable internal consistency (0.71 ≤ α ≤0.77) and test–retest reliability ranging from 0.62 to 0.71.40 Moderate correlations between the IRI and other measures of empathy have been reported,.40
The FIS-SR, CASES and IRI have been translated into Danish by the last author, back-translated into English by a native speaker and approved by the copyright holders.
Potential between-condition moderators of outcome
Therapist characteristics. A short self-report questionnaire developed for this study will obtain information on therapist sociodemographic and professional characteristics regarding (1) completed courses in psychotherapy and helping skills, (2) previous work as a therapist or counsellor, (3) supervision received, (4) professional care work, and (5) personal therapy (all reported in hours).
The Structural Analysis of Social Behavior Intrex questionnaire (SASB) focuses on self-concept and relationships.41 The study will use the 36 items measuring a person’s introject on two dimensions: (1) autonomy (self-freeing to self-controlling) and (2) affiliation (friendly to hostile). The students will be instructed to rate themselves ‘as they usually are’ to increase the probability of measuring more stable aspects of self-relatedness. The SASB Introject has obtained acceptable reliability scores and higher levels of self-attack has consistently been associated with higher levels of symptom distress, interpersonal problems and personality disorder problems.42 Moreover, the SASB has been reported to predict or moderate therapy outcome.43–45
Social Skills Inventory (SSI) brief form is a self‐report measure of social competencies.46 The SSI consists of 30 items capturing six aspects of social competencies (emotional expressivity, emotional sensitivity, emotional control, social expressivity, social sensitivity and social control). The overall mean score will be used in this study. In previous research, the internal consistency for the full 90-item scale was good to excellent (α=0.88 and 0.90).28 46 Test–retest correlations ranged from 0.81 to 0.96 for a 2‐week interval.46 Convergent and discriminant validity for the SSI has been supported in relation to other measures of non-verbal social skills and personality.47 The correlation between the overall score of the brief SSI and the overall score of the full scale is 0.91, indicating that the overall score of the brief scale can be used as a global measure of social competencies.46
The Experiences in Close Relationships Scale-Revised (ECR-R) measures attachment insecurity.48 ECR-R has 36 self-reported items covering two dimensions: (1) attachment avoidance characterised by fear of interpersonal dependence and intimacy and (2) attachment anxiety characterised by fear of abandonment and craving for interpersonal closeness. Internal consistencies of the anxiety and avoidance subscales have been found to be excellent with α=0.93 and 0.95, respectively.49 Construct validity is supported by correlations with measures of symptoms and personality.50
Internal and External Feedback Propensity Scales (IEFPS) measures feedback propensity on two subscales: (1) preference for receiving feedback from others (ie, external feedback propensity) and (2) from self (ie, internal feedback propensity).51 Each subscale consists of six items. Acceptable internal consistency has been found for the external feedback propensity scale (α=0.71 and 0.62) and the internal feedback propensity scale (α=73 and 0.71).34 52
The Group Climate Questionnaire—Short Form (GCQ-S) measures the group member’s perception of the group’s environment.53 GCQ-S contains 12 self-report items covering three subscales: The Engagement Scale, the Conflict Scale and the Avoidance Scale. In a previous study, coefficient alphas for the GCQ subscales were 0.94 for engagement, 0.92 for avoidance and 0.88 for conflict.54 Validity is supported by numerous studies finding relationships between the GCQ and outcome, group development and other process variables.55 In the present study, the GCQ-S will be used to measure the cooperation in the small groups of four to five students working together throughout the study period (ie, the group level). Item 5 was adapted by changing ‘group leader’ to ‘teacher/supervisor’.
The authorised Danish version of the ECR-R and GCQ-S will be used. The SASB, SSI and IEFPS have been translated to Danish by the last author, back-translated into English by a native speaker and approved by the copyright holders, except for the IEFPS where the authors could not be reached.
Potential predictors of outcome in the experimental condition
The amount of training and deliberate practice activity will be assessed in several ways. First, the classroom attendance rate will be registered for each student. Second, a short self-report questionnaire developed for this study will report the number of times each student role-played the therapist, the total time spent on deliberate practice homework, and the number of pages read from the syllabus. Third, the students’ use of Skillsetter will be tracked by Skillsetter as (a) the total time spent on watching and responding to videos and (b) the average number of attempts to improve the answer after the feedback.
Adherence and quality of training
The observer-rated DP Coach Competency Scale (DPCCS) will be used to assess the quality of the deliberate practice training.56 The DPCCS has two subscales: (1) the DP Coaching Tasks scale measuring if the training is on task and (2) the DP Coaching Interpersonal Effectiveness scale measuring the learning environment. Two independent observers will rate the ten items in the DPCCS on a Likert scale from 0=lack of competence to 6=excellent competence. Ratings will be based on video recordings of all training sessions.
Procedures for data collection
All data will be collected electronically through an online data collection platform three times: at baseline (week 0), after the first condition (week 5) and after the second condition (week 10). All students will contribute with data in both conditions because all students receive both the experimental and the control condition (in reverse order). Data will be collected in a private room at the universities, where the students will first complete the self-report measures and then respond to FIS videos and the FIS-SR. Outcomes will be attempted to be collected from students who discontinue or deviate from intervention protocols. The students’ responses will be recorded and stored safely. A unique student identifier will make it possible to combine the various measurements, after which the student identifier will be deleted, anonymising data.
Statistical analyses
The effect of the deliberate practice training will be analysed using linear mixed models (LMM) with repeated measures because the data have a nested structure. Regarding hypothesis 1 and 2, an effect of deliberate practice training will be indicated by a statistically significant two-way interaction between condition and time at week 5, where data come from truly randomised groups (before the crossover). Time at level 1 is nested within students at level 2, which is nested within-student group at level 3 (the students are organised in groups of four to five students working together throughout the study period). Intraclass correlation coefficients (ICC) will be calculated from the between and within variance to estimate the variance explained by the student and student-group level. If level 3 (ie, student group) does not improve the overall model fit as evaluated by a change in the −2LL fit statistics, only two levels (ie, time and student) will be included in the final model. LMM will be applied to test for a time-order effect (ie, whether it makes a difference if the deliberate practice intervention comes before or after the theoretical teaching in the control condition).
Effect sizes (ES) will be calculated as Cohen’s d. The between-group ES, expressing the incremental effect of the intervention, will be derived from the F-test (time × condition) and calculated as d=2 x  ). In the calculation of the between-group effect (time × condition), the effects will be analysed before the crossover for primary and secondary outcomes (data from week 0 and 5, reflecting true randomisation). Subsequently, the effect after the crossover (data from week 5 and 10) and the effect after both conditions (data from week 0 and 10) will be explored.
). In the calculation of the between-group effect (time × condition), the effects will be analysed before the crossover for primary and secondary outcomes (data from week 0 and 5, reflecting true randomisation). Subsequently, the effect after the crossover (data from week 5 and 10) and the effect after both conditions (data from week 0 and 10) will be explored.
Regarding hypotheses 3 and 4, moderators and predictors will be tested to investigate the potential impact of both student baseline characteristics and training-related variables on the effect of deliberate practice training. If no time-order effect is found, the full data set encompassing both the experimental and the control condition will be used in the analyses. Tested moderators will include age, gender, theoretical orientation, level of clinical experience, motivation, introject (SASB), social skills (SSI), attachment style (ECR), feedback propensity (IEFPS) and training site. Training site will be treated as a fixed factor in the model. Tested predictors will include total time spent responding to Skillsetter videos and average number of attempts to answer each video. The between-condition moderators and within-condition predictors will be tested by entering each variable one at a time into the LMM-equation and a final model will be estimated, including all significant moderators and predictors.
The maximum likelihood method and an unstructured covariance matrix will be used to estimate the parameters. Missing data will be handled by the full information maximum likelihood, which makes it possible to analyse data as intention-to-treat.
To estimate the minimum sample size required for the study, a power calculation for analysis of covariance (α=0.05; power=0.80) was conducted using GPower V.3.1.2.57 Medium effects were selected as estimates of ES based on two recent investigations of deliberate practice training.27 58 The power analysis determines that a total sample of 128 participants will be required (before adjusting for the nested structure of the data). To compensate for the statistical dependencies introduced by nesting, we multiplied the calculated sample size (ie, 128) with one plus the ICC. The ICC for repeated measures is typically about 0.55, which gives us a minimum required sample size of 198 (99 in each group). With an estimated number of participants of 70 per year, the sample size will be reached in December 2023.
Patient and public involvement
A pilot version of the course was conducted at both study sites in 2020, making it possible to redesign the course based on students’ feedback regarding feasibility and course content. A national advisory board has been established, consisting of researchers from all graduate psychology studies in Denmark, the Danish Psychological Association and a Higher Education and Science representative. The project is supported by an international scientific advisory board consisting of three leading researchers in psychotherapy training, Bruce Wampold, Timothy Anderson and Tony Rousmaniere. These advisory boards have no power of decision.
Ethics and dissemination
Before signing up for the course, the students will be informed about the course and the research embedded herein. Teachers will obtain informed consent from students agreeing to participate in the study. Students can decline to participate in the study or discontinue their participation at any time during the course without any negative consequences for their participation in the course. Ethical approval has been obtained from the Institutional Ethical Review Board, Department of Psychology, University of Copenhagen and Aalborg University. Study findings will be published in international peer-reviewed journals. Informed consent materials, data management procedures and anonymised participant-level data sets can be provided on request to the authors.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors The principal investigators of this research project, SBP and OKØ conceived the study, formulated the research design and executed the first and the final draft of this protocol. JN, CH and KKN contributed with ideas, methodological considerations and revisions of the protocol. All authors approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.