Article Text

Abstract
Introduction Prostate-specific membrane antigen positron emission tomography (PSMA-PET) has emerged as valuable imaging to assessing metastatic disease in prostate malignancy. However, there has been limited studies exploring the utility PSMA-PET as primary imaging assessing for index lesions prior to biopsy. The primary objective of this study is to compare the diagnostic accuracy of 18-fluorine PSMA (18F DCFPyL PSMA) PET scans to multiparametric MRI (mpMRI) to detect primary prostate cancer at prostate biopsy.
Methods and analysis The PEDAL trial is a multicentre, prospective, single-arm, paired comparison, non-randomised phase III trial in subjects considered for diagnostic prostate biopsy. Subjects who are eligible for a diagnostic mpMRI prostate will undergo additional same-day 18 F DCFPyl PSMA PET/CT of the chest, abdomen and pelvis. Software coregistration of the mpMRI and PSMA-PET/CT images will be performed. The reporting of the mpMRI prostate, PSMA-PET/CT and PSMA PET/MRI coregistration will be performed blinded. The diagnostic accuracy of PSMA PET/CT alone, and in combination with mpMRI, to detect prostate cancer will be assessed. Histopathology at prostate biopsy will be used as the reference standard. Sample size calculations estimate that 240 subjects will need to be recruited to demonstrate 20% superiority of PSMA-PET/CT. The sensitivity, specificity, positive predictive value and negative predictive value of the combination of mpMRI prostate and PSMA PET/CT compared with targeted and systematic prostate biopsy will be evaluated. It is hypothesised that PSMA PET/CT combined with mpMRI prostate will have improved diagnostic accuracy compared with mpMRI prostate alone for detection of prostate cancer in biopsy-naïve men, resulting in a significant impact on patient management.
Ethics and dissemination This study was approved by the independent Human Research Ethics Committee. Results will be published in peer-reviewed medical journals with eligible investigators will significantly contribute.
Trial registration number ACTRN12620000261910.
- prostate disease
- magnetic resonance imaging
- nuclear radiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This is a multicentre study.
A strength of this study is its prospective nature of the study design controlled by using patients own biopsy results as comparator, thus limiting confounders.
This is an adequately powered study with objective primary and secondary outcome measures.
Potential limitations pertain to generalisability of results given use of DCFPYL tracer for prostate-specific membrane antigen positron emission tomography (PSMA-PET/CT). There are currently limited studies directly comparing different PSMA-PET tracers.
Introduction
Prostate cancer (PCa) is very common, with one in six men being diagnosed before the age of 85 years.1 The age-standardised incidence rate has increased from 80 cases per 100 000 males to 141 cases per 100 000 males since 1982, likely driven by the implementation of prostate-specific antigen (PSA) screening. With the growing incidence of disease, prostate imaging and biomarkers2 3 has become increasingly important in the diagnostic evaluation of PCa to detect clinically significant PCa (csPCa, grade group ≥2) and assess tumour burden.
In Australia, multiparametric MRI (mpMRI) of the prostate gland has also become available under Australian government funded rebate for diagnostic evaluation of suspected PCa and active surveillance of low-risk PCa with economic analysis suggesting significant savings to the health system.4 5 mpMRI offers reliable visualisation and characterisation of csPCa compared with the traditional transrectal ultrasound (TRUS), and is seen to have greater sensitivity of detection for lesions greater than 1 cm, Gleason score of ≥7 and index lesions compared with satellite lesions, thus enabling better selection of patients for prostate biopsy.6 In a meta-analysis of 42 studies, the pooled negative predictive value of mpMRI was reported to be 90.8%–97%.7 mpMRI-targeted prostate biopsy has been reported to detect more csPCa than systematic TRUS-guided biopsy (38% vs 26%).8 Nevertheless, mpMRI is not without limitations. Variable imaging quality, interreader variability, low specificity and missed or underestimated tumours remain an issue.9 10 The PAIREDCAP trial reported 15% of patients with negative mpMRI findings were found to have csPCa on systematic prostate biopsy.11
Along with mpMRI, prostate-specific membrane antigen positron emission tomography (PSMA-PET) is one of the key advancements to emerge in PCa assessment over the last two decades.12 13 PSMA is a type II transmembrane protein that is overexpressed on PCa cell membranes in all but 5%–10% of cases showing high specificity and sensitivity relating to tumour aggressiveness and metastatic potential.14 15 18F-choline PET scans have been shown to improve risk stratification when used in conjunction with mpMRI.16 This in conjunction with the prostate specific tracer of PSMA leads to strong support using PSMA-targeted PET imaging for staging of high-risk disease and biochemical recurrence.17–20 In the proPSMA trial, PSMA PET/CT was demonstrated to have 27% greater accuracy than conventional staging (92% vs 65%) for pelvic or distant metastases, providing superior accuracy with fewer equivocal results and lower radiation exposure.17 Moreover, recent evidence demonstrate that Ga-PSMA-11 intensity on PET/CT imaging is associated with Gleason score, and is more intense in those patients who underwent upgrading of their Gleason score at biopsy to Gleason score at radical prostatectomy,21 and could develop to be a new biomarker for prognosis in PCa.
The use of PSMA PET/CT as a first line diagnostic tool for suspected PCa is under investigation.22 23 The PRIMARY study22 recently reported the additive value of pelvic-only 68Ga-PSMA PET/CT to a ‘triaged’ mpMRI population to detect csPCa in men with suspicious for PCa. The trial showed combined PSMA-PET/CT and MRI compared with MRI alone improved the negative predictive value (91% vs 72%, p<0.001) and sensitivity (97% vs 83%, p<0.001). However, specificity was reduced (40% vs 53%, p=0.01). Several other studies demonstrated similar results of improved sensitivity.12 24 Additionally, for equivocal lesions on mpMRI (ie, PIRADS 3), PSMA-PET/CT may add to stratification of these lesions, with csPCa was more often detected when any focal PSMA uptake was detected 3/6 (50%), compared with those with no appreciable PSMA uptake 2/11 (18%).25 Finally, PSMA-PET/CT in addition to mpMRI showed increased sensitivity when detecting extraprostatic extension and seminal vesical invasion,26 although specificity reduced slightly,26 as seen in the PRIMARY trial. Hybrid PET/MRI scanners using the 68Ga-PSMA ligand have also provided compelling evidence that it may be superior to prostate mpMRI alone to detect csPCa, however, use of these machines will be limited by cost and poor accessibility.27 28
Given the morbidity and mortality associated with prostate biopsy and PCa treatment, the potential for improved diagnostic accuracy using PSMA PET/CT to localise PCa in biopsy-naïve men warrants further investigation. The PEDAL trial is a prospective, single-arm paired comparison trial that aims to provide high-quality evidence regarding the diagnostic accuracy of 18F-DCFPyl-PSMA PET/CT in conjunction with mpMRI prostate for primary diagnosis of PCa.
Methods and design
Ethics
This clinical trial has been approved by the St Vincent’s Hospital, Melbourne Human Research Ethics Committee (HREC 230/19) and is registered on the Australian New Zealand Clinical trials registry (ACTRN12620000261910). The current protocol is version 3, dated June 2019. It will be conducted in accordance with the International Conference on Harmonisation protocols and Good Clinical Practice. In addition, the trial will be conducted in compliance with all applicable laws and regulatory requirements relevant to the use of new therapeutic agents in Australia and any other participating country. Funding will be acquired through Cyclotek (manufacturer of DCFPYL), General Electrical Healthcare and philanthropic grants. These parties will not be involved in study design; data processing and interpretation; writing of the report; and the decision to submit the report for publication.
The trial schema is outlined in figure 1.
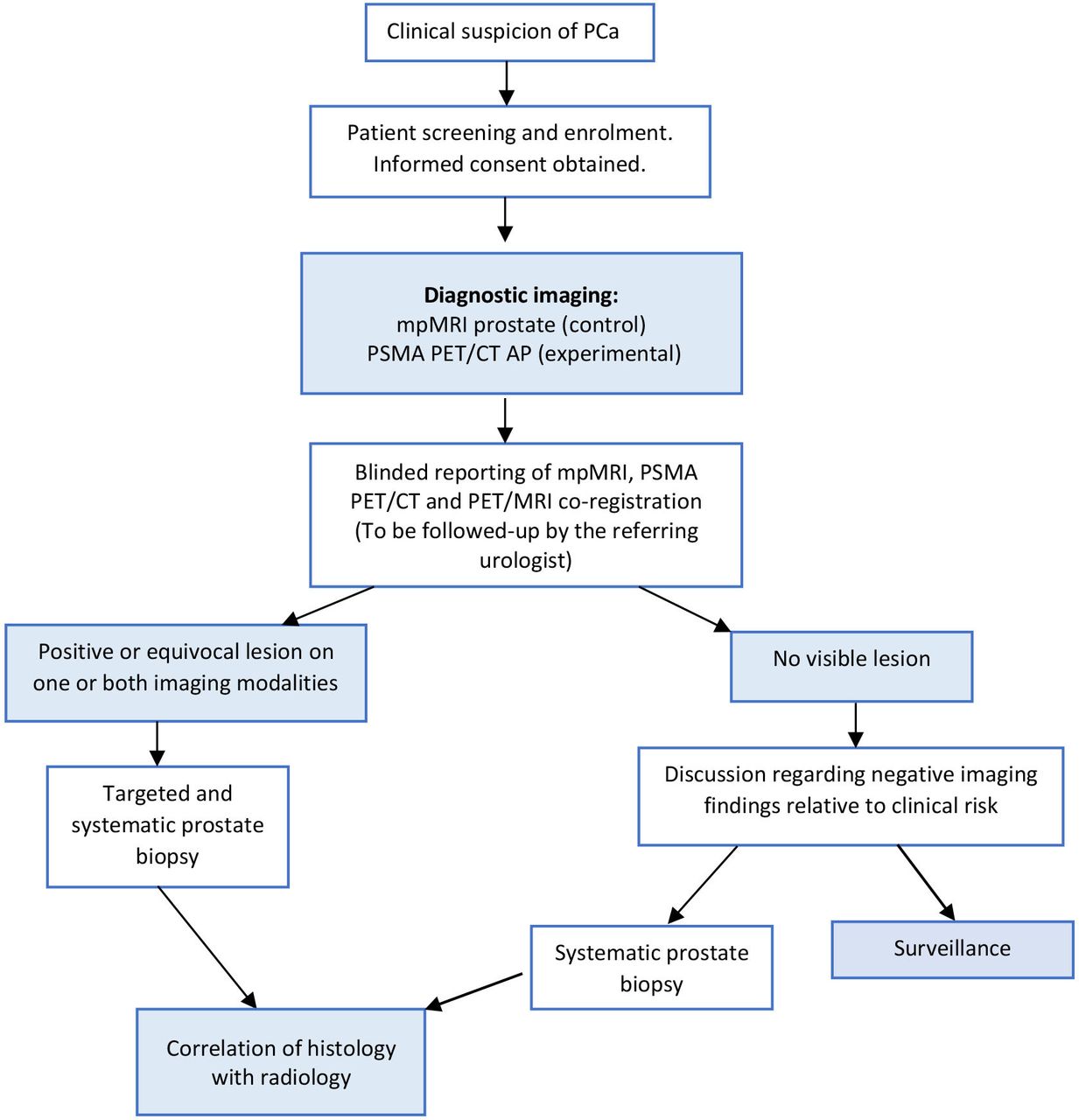
{kind=link}
Trial schema. mpMRI, multiparametric MRI; PCa, prostate cancer; PSMA-PET/CT, prostate-specific membrane antigen positron emission tomography/CT.
Patient and public involvement
No formal patient advisory committee was set up and there was no patient or public involvement in the design and planning of the study. The study was so designed as the mpMRI, PSMA-PET and prostate biopsy procedures used are not novel concepts or techniques, and are widely available in Australia as part of the Medicare system for which consumer and stakeholder comment is sought prior to inclusion of these interventions. Nevertheless, the patients are invited to provide feedback at each point of contact with the healthcare system. In addition, the results are intended for publication in peer reviewed medical journals.
Study design
This is a prospective single-arm paired comparison diagnostic phase III trial in patients who are being considered for diagnostic prostate biopsy to detect PCa. We aim to evaluate the role of PSMA-PET/CT in those with high clinical suspicion of PCa. The PSMA-PET/CT, by identifying a suspicious lesion, is likely to impact the decision for prostate biopsy and the target location. The diagnostic accuracy of the imaging studies will be assessed by comparison of imaging results to prostate biopsy results. Any modifications and updates to study protocol will be communicated to the relevant parties via email.
Patient screening, eligibility and enrolment
Patients with features suspicious for PCa based on an abnormal PSA or digital rectal examination will be screened by a urologist for trial eligibility in the study according to the inclusion and exclusion criteria listed below in box 1,29 and will be consented by the urologist (including for any ancillary studies). Where a substitute decision make is required, the legal next of kin or the power of attorney may consent in the patient’s stead. A target of 240 subjects will be recruited from multiple sites. Aside from the addition of PSMA PET/CT, all patients will follow routine care for PCa and there are no specific interventions that are prohibited or permitted.
Study inclusion and exclusion criteria
Inclusion criteria
Men (≥18 years) with an elevated PSA who are suitable for an eligible MBS mpMRI prostate.
(Medicare Benefits Scheme (MBS) items 63 541 and 63 542) and who have not had recent (≤3 years) prostate biopsy or mpMRI prostate.
For MBS items 63 541 and 63 542 (NK) the patient must be suspected of having prostate cancer based on (*):
DRE which is suspicious for prostate cancer.
In a person aged less than 70 years, at least PSA tests performed within an interval of 1–3 months are greater than 3.0 ng/mL, and the free/total PSA ratio is less than 25% or the repeat PSA exceeds 5.5 ng/mL.
In a person aged less than 70 years, whose risk of developing prostate cancer based on family history is at least double the average risk, at least two PSA tests performed within an interval of 1–3 months are greater than 2.0ng/mL, and the free/total PSA ratio is less than 25%.
In a person aged 70 years or older, at least two PSA tests performed within an interval of 1–3 months are greater than 5.5 ng/mL and the free/total PSA ratio is less than 25%.
NB: Relevant family history is a first degree relative with prostate cancer or suspected of carrying a BRCA 1, BRCA 2 mutation.
The patient has provided written informed consent for participation in trial.
In the opinion of the investigator, willing and able to comply with required study procedures.
Exclusion criteria
Known diagnosis of prostate cancer.
Previous prostate biopsy within 3 years of recruitment. A transurethral resection of the prostate performed for primary purpose of alleviating lower urinary tract symptoms is considered acceptable.
Previous mpMRI prostate within 3 years of recruitment.
History of other active malignancy within the last 3 years, with the exception of non-melanoma skin cancer or melanoma in situ.
Any absolute contraindication to 3T mpMRI prostate, or history of total hip joint replacement.
Significant intercurrent morbidity that, in the judgement of the investigator, would limit compliance with study protocols.
DRE, digital rectal examination; mpMRI, multiparametric MRI; PSA, prostate-specific antigen.
Adapted from New MBS for mpMRI of the prostate.20
Follow-up
Participants will be followed up by their referring urologist to discuss results and ongoing management of either PSA surveillance, active surveillance, radical treatment or non-curative treatment. Patient retention and follow-up is anticipated to be complete as the study patients require further testing (eg, Biopsy) to complete management of their PCa.
Funding
Subjects will be informed of the costs of participation as part of the informed consent. For those eligible, the mpMRI will be funded through the Australian Government Department of Health Medicare Benefits Scheme (ie, free of charge to the patient). The PSMA PET/CT will be funded through the clinical trial. The prostate biopsy will be funded as standard practice through the Medicare Benefits Scheme, private health insurance and subject. Subjects will not be paid for their participation and no participating clinical or researcher will be paid outside of their normal salary.
Diagnostic imaging procedures
All participants will undergo both the PSMA-PET/CT and mpMRI within 4 weeks of enrolment into this study and both scans performed on the same day to minimise disruption to participants’ personal schedules. To standardise parameters of acquisition and image quality, these will be performed at an approved study centre.
Multiparametric MRI
All subjects will undergo 3-Tesla mpMRI prostate according to standard protocols (online supplemental appendix 1). The images will be reported by a single experienced Radiologist using the Prostate Imaging-Reporting and Data System (PI-RADS) version 2.1 on a scale of 1–5 (online supplemental appendix 2). Any suspicious intraprostatic lesion described as PI-RADS 3 or greater will be considered a positive lesion with a targeted prostate biopsy recommended. The presence of extracapsular extension, seminal vesicle invasion, locoregional disease and subjective likelihood of csPCa will be recorded. The initial report of the mpMRI prostate will be blinded to the PSMA-PET/CT result.
Supplemental material
Prostate-specific membrane antigen positron emission tomography/CT
All participants will undergo PSMA-PET/CT imaging with18F-DCFPyL according to standard protocol (online supplemental appendix 3) at the participating site, on the same day as the mpMRI. The 18F-DCFPyL radiotracer will be produced in Australia and New Zealand by Cyclotek Pty Ltd, who will provide the local site with a Quality Control Release notification form. A single, intravenous bolus dose of 18F-DCFPyL PSMA (250MBq+/-50 MBq) will be administered with an uptake time of 120 min post 18F-DCFPyL injection. 18F-PSMA PET with CT chest, abdomen and pelvis will be performed for anatomic localisation and attenuation correction.
PSMA-PET/CT images will be reported at a per-patient and per-lesion level by an experienced reader at each site. The initial report of PSMA-PET/CT will be blinded to the mpMRI prostate result. To standardise lesion imaging reporting, the intraprostatic lesions will be described according to the sector map specified in PI-RADS version 2.1 for mpMRI prostate. The PSMA intensity score (SUVmax), focality and ratio to background will be assessed. The reader will report disease location and extent, as well as assign a subjective likelihood for the presence of csPCa. All lesions with SUVmax scores of 4.0 or higher are deemed appropriate for targeted biopsy. While results of the PRIMARY trial were disseminated after our protocol was designed, it also uses a SUVmax of 4.0 as at this stage the sensitivity for csPCa was 92%.22 This may be adjusted following quantitative analysis of thresholds, (liver and background prostate in particular), for the presence of malignancy, although the PRIMARY trial would suggest that adjustments will not be required.22
Coregistration of the PSMA-PET/CT with mpMRI prostate
After both diagnostic imaging arms have been independently reported, coregistration of the two modalities will be performed using the GE Advantage Workstation (General Electric, Boston, Massachusetts, USA) software. Reporting of coregistered PSMA-PET/CT with mpMRI images will be performed by an experienced dual-trained radiologist with PET accreditation and experience of reporting prostate mpMRI. A synoptic report will describe lesions seen on the mpMRI alone, PSMA-PET/CT alone, followed by the result of the coregistration process to determine concordance between 18F-DCFPyL PSMA-PET and mpMRI and the reader’s subjective likelihood of the presence of csPCa will be reported. Lesions will be numbered to enable accurate cataloguing at time of prostate biopsy, and visually represented on the PI-RADS version 2.1 prostate map.
Prostate biopsy
Prostate biopsy procedure
The referring urologist will have access to reports and images for both diagnostic imaging modalities and PSMA-PET/MRI coregistration results in order to make a clinical decision regarding prostate biopsy. Subjects with any positive and/or equivocal findings in either diagnostic imaging arm are recommended to undergo a targeted biopsy of all lesions and a systematic biopsy for histopathological analysis. Targeting is accomplished via cognitive fusion at time of biopsy. The study recommends a standardised transperineal ultrasound-guided template biopsy format perfumed under general anaesthesia. A minimum of four cores of any targeted lesion and minimum 24 systematic cores to be taken. Subjects with no abnormalities on mpMRI and PSMA PET/CT are recommended to have a systematic biopsy (24 cores). All biopsies are performed by surgeons already trained in and practicing the transperineal biopsy route, thus minimising variability and possible confounders.
Histopathology
Biopsy specimens will be labelled based on location and whether obtained through targeted or systematic prostate biopsy. Reporting of the prostate biopsy will be performed by genitourinary histopathologists at each site using standardised proformas, detailing the number of cores taken, location (including the index lesion), histological subtype and International Society of Urological Pathology (ISUP) grade group, number of positive cores per site, percentage and longest length of cancer in one core and perineural invasion.30
Study assessment
Study objective and endpoints
The endpoints of this study are summarised in box 2. The primary objective is to assess for diagnostic superiority of PSMA-PET/CT in combination with mpMRI in detection of lesions with any ISUP grade PCa. Specifically, cancer detection rates, sensitivity, specificity, negative predictive values, positive predictive values and area under the curve (AUC) are explored. The secondary outcomes involve detection of csPCa as well as a cost evaluation using a decision curve analysis.
Pedal study endpoints
Primary endpoint
Comparison of diagnostic accuracy of mpMRI prostate to PSMA-PET/CT alone and in combination with mpMR in the detection of prostate cancer (any ISUP) per patient and per lesion.
Secondary endpoints
Detection of clinically significant (ISUP grade group ≥2) primary prostate cancer at prostate biopsy.
Detection of radiologically significant lesions in the prostate at PSMA-PET/CT and MRI coregistration.
Detection of radiological evidence of metastatic lesions on PSMA-PET/CT and/or mpMRI Prostate.
Number of adverse events reported during and postadministration of radiotracer for PSMA PET/CT.
Decision curve analysis.
ISUP, International Society of urological Pathology; mpMRI, multiparametric MRI; PSMA, prostate-specific membrane antigen; PET/CT, positron emission tomography/CT.
Sample size and power calculation
The trial will proceed to recruit to an ideally powered sample size of 240 subjects to achieve a power of 0.80. Sample size calculations were based on the primary endpoint of detection of all ISUP grade PCa detection. Receiver operator characteristic and AUC, sensitivity and specificity for mpMRI and PSMA-PET/CT are 0.84, 0.603 and 0.89,31 and 0.91, 0.88 and 0.93,32 respectively. The following assumptions were made for sample size calculations: 50% of men who undergo prostate biopsy will be diagnosed with PCa, the proportion of cases (PSMA PET/CT as opposed to mpMRI) is 20% higher, the absolute margin of improvement is 7% (0.35–0.42) to declare PSMA-PET/CT is superior, the estimated correlation between the two tests is 80% and a two-sided type I error of 5%. In addition, this sample size makes allowance for a dropout rate of 10%.
Data management
Data will be collected onto a password protected files located on the institutional computer, also password protected. Access is given only relevant researchers of this study. The institutional computer is situated in a locked office with only the relevant investigators having access. Data collection is performed by investigators not directly involved in patient care with one investigator collecting data and a second reviewing data independent to ensure completeness. Given the prospective nature of this study, identifiable information is collected for enrolled patients with security measures as detailed above. Range checks will be carried out to promote quality. Data will be audited on a monthly basis to ensure quality. Auditors are investigators independent from sponsors. There is no input from any sponsors to data management. The final trial dataset will be deidentified prior to statistical analysis. The lead investigator as well as those involved in data analysis will have access to the final trial dataset
Blinding
Blinding occurs at the level of the clinician reviewing the imaging and biopsy specimens. Separate clinicians review the mpMRI, PSMA-PET/CT and coregistered PMSA-PET/CT and mpMRI images, with each clinician blinded to the results of the other two imaging assessment modalities. The uropathologist will receive tissue samples labelled as a systematic or targeted biopsy and its position, however is blinded to the results of PI-RADS score or PSMA-PET/CT positivity. There is no anticipated need for unblinding of investigator clinicians, as the complete results for each study patient will be viewed by a treating clinicians after all reporting is completed.
Results and outcomes
Summary tables will be prepared giving numbers of participants by arm, disease assessment compliance, eligibility infringements and lost to follow-up. Baseline characteristics by treatment arm will be summarised in frequency tables by the use of descriptive statistics for variables. A 95% CI for differences between arms of all important endpoints will be calculated, and p values will be two sided. Exact tests will be performed with binary outcome data. Data collection forms can be made available on request.
Diagnostic accuracy
To determine diagnostic accuracy of PSMA PET/CT compared with mpMRI prostate in the detection of csPCa, findings of imaging will be compared with prostate biopsy histopathology to determine presence or absence of cancer. Clinically significant PCa at prostate biopsy is defined as ISUP grade group ≥2. For the primary objective, positivity will be defined by histological confirmation of cancer at prostate biopsy.
Accuracy of each diagnostic imaging arm will be assessed by the AUC. mpMRI accuracy will be compared with PSMA PET/CT alone, and in combination with mpMRI. Point estimates of the sensitivity and specificity of each modality alone will be determined, and approximations to their distributions will be estimated using the normal approximation to the binomial distribution. Using independence of the sensitivity and specificity, the AUC will be calculated as the mean of the estimated sensitivity and specificity, and its variance as the sum of the variances of the sensitivity and specificity. Equivocal lesions will be considered negative for clinical purposes, however, these lesions will be targeted during biopsy and a sensitivity analysis will be performed in which lesions rated as equivocal will be considered positive for malignancy. The difference between the AUCs will be used to characterise the true underlying difference between AUCs of the two modalities and to apply a hypothesis test for the existence of a clinically important difference between them (the null hypothesis will be a 7% difference).
Cost evaluations
The potential for cost savings will be evaluated. Considerations included in our analysis are: reductions in prostate biopsy (and efficiencies in consolidation of diagnostic and staging imaging tests) and using software coregistration as an alternative to hybrid PET/MRI machines. Cost evaluations using tools such as a decision curve analysis will be conducted as a secondary outcome. This is preferred as traditional decision-analytical methodologies does not assess clinical consequences and provide results in a continuous form rather than binary.33 Decision curve analysis will be conducted according to Vickers et al33 of PSMA PET/CT compared with prostate biopsy results for clinically significant PCa.
Risks of PSMA-PET/CT
Several preclinical and clinical studies have shown the safety of 18F-PSMA. The critical dose organs are the kidneys (0.0945 mSv/MBq) and urinary bladder (0.085 mSv/MBq) and were calculated from human biodistribution data using OLINDA/EXM (Organ Level Internal Dose Assessment/Exponential Modelling) software. Based on the Food and Drug Administration (FDA), a single-organ dose of 0.05 Sv is allowable. This corresponds to an activity of 400 MBq (10.8 mCi) of 18F-PSMA for a 70–100 kg male subject with a PCa, well above the doses used in this study. Accordingly, the effective dose expected to the whole body is 0.0066 Sv, which is below the 0.03 Sv upper limit recommended by the FDA.
Adverse events and contraindications
No adverse effects due to intravenous administration of 18 F-PSMA for imaging have been reported in the published literature. There are no known contraindications for 18F-PSMA. Overall, 18F-PSMA PET scan may be used in clinical research with no risk to subjects with PCa. As such, there is no anticipated additional adverse events from PSMA PET/CT imaging.
Acute adverse events, defined as those experienced by the subject at the time of radiotracer administration and during the 2 hours following injection will be recorded. Any toxicity will be graded by National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events version 5.0.34
Discussion
The drive to accurately detect intraprostatic and extraprostatic disease at the time of PCa diagnosis has led to the intense interest in PSMA-PET/CT as an adjunct to mpMRI prostate. PSMA PET/CT has shown to be highly useful in the setting of high-risk disease and biochemical failure postradical treatment,35 36 however, its utility as a diagnostic tool for PCa evaluation until recently,22 there has had minimal high-quality prospective data. Our hypothesis is that PSMA-PET/CT will be superior in diagnostic accuracy to mpMRI prostate at identifying cancer within the prostate. As mpMRI prostate is established in its ability to successfully identify PCa, this is a high standard to achieve. Even if PSMA-PET/CT does not supersede mpMRI prostate in diagnostic accuracy, establishing comparable diagnostic accuracy may result in a viable alternative for men who have contraindications to mpMRI.
The use of PSMA intensity as a biomarker shows potential. Roberts et al demonstrated association between 68Ga-PSMA-11 intensity and Gleason score, in addition to upgrading of Gleason score between biopsy and radical prostatectomy results. Specifically, 9 of 14 upgraded patients from biopsy were from Gleason 3+4 to 4+3 on radical prostatectomy histology. This has strong implications for those Gleason 3+4 patients who were initially planned for active surveillance, with the authors suggesting SUVmax of >8 in Gleason 3+4 malignancy could be a potential prognostic biological marker of more aggressive disease.21 While our study uses 18F-DCPFyl PSMA, we expect to achieve similar results. Furthermore, several other biomarkers such as the prostate health index have emerged as promising diagnostic implement.3 The prostate health index showed high accuracy in predicting positive biopsy results.2 As such, inclusion of biomarkers as part of our study is not ruled out and development of a diagnostic algorithm including biomarkers could improve detection of clinically significant PCa.
The trial may also demonstrate (1) a synergistic effect in cancer diagnosis by the combination of the two imaging techniques, (2) a benefit for PSMA-PET/CT in men with equivocal mpMRI prostate findings; (3) benefit for men with concerning clinical features but negative/equivocal mpMRI prostate and (4) provide an all-encompassing diagnostic and staging scan for men who have high-risk features for metastatic disease at diagnosis. Unlike the PRIMARY trial, our PSMA-PET/CT protocol encompasses chest, abdomen and pelvis, so will be able to add valuable information to this outcome.
Proprietary software from the GE Advantage Workstation will perform coregistration between mpMRI prostate and PSMA-PET/CT images will be used in this trial. Coregistration has potential to improve targeting of prostate biopsy techniques, and help provide an alternative to expensive, difficult to access hybrid PET/MRI machines.
After diagnostic accuracy of PSMA-PET/CT is established, its potential for significant economic impact as a diagnostic test can be thoroughly investigated. Reductions in prostate biopsy, efficiencies in consolidation of diagnostic and staging imaging tests, and using software coregistration as an alternative to hybrid PET/MRI all represent potential economic benefits to our health system.2 3
The PEDAL trial commenced in March 2020, and although recruitment has been delayed due to COVID-19-related adjustments in healthcare delivery the current aim is to complete recruitment in 36 months. This innovative study will add valuable evidence to demonstrate the diagnostic accuracy of PSMA-PET/CT. It has potential to significantly impact how PCa is diagnosed.
Participating centres
St Vincent’s Hospital, Melbourne, Victoria.
St Vincent’s Private Hospital, Melbourne, Victoria.
The Royal Melbourne Hospital, Victoria
Epworth Healthcare, Victoria.
Sydney Adventist Hospital, New South Wales.
Pacific Radiology Canterbury, Christchurch, New Zealand.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @lawerentschuk
Contributors VT: protocol design, ethical submission, procurement of funding, data collection, statistical analysis, manuscript preparation, patient care, supervision. AH: manuscript preparation, statistical analysis. TS: protocol design, ethical submission, procurement of funding, data collection, statistical analysis, manuscript preparation, patient care, supervision. KT: protocol design, ethical submission, procurement of funding, data collection, statistical analysis, manuscript preparation, patient care, supervision. S-FL: protocol design, ethical submission, procurement of funding, data collection, statistical analysis, manuscript preparation, patient care, supervision. DL: patient care, supervision. KS: patient care, supervision. NMC: patient care, supervision. NL: patient care, supervision. HW: patient care, supervision. LT: patient care, supervision. DB: manuscript preparation, supervision. TS: patient care, data collection, statistical analysis, supervision. LT: patient care, data collection. RB: patient care, data collection. JH: patient care, data collection. EP: patient care, data collection. L-MW: protocol design, ethical submission, procurement of funding, data collection, statistical analysis, manuscript preparation, patient care, supervision.
Funding This clinical trial is supported by Cyclotek (Aust) Pty Ltd and their key partners, the Australian Government as part of its CRC Projects Program, General Electrical Healthcare, Macquarie University and the EJ Whitten Prostate Cancer Research Centre at Epworth Healthcare. We are also grateful for philanthropic donations from Reese Limited, the Pitcher and Cicutto families via the St Vincent’s Foundation.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.