Article Text

Abstract
Objectives To determine if motion control walking shoes are superior to neutral walking shoes in reducing knee pain on walking in people with lateral knee osteoarthritis (OA).
Design Participant-blinded and assessor-blinded, comparative effectiveness, superiority randomised controlled trial.
Setting Melbourne, Australia.
Participants People with symptomatic radiographic lateral tibiofemoral OA from the community and our volunteer database.
Intervention Participants were randomised to receive either motion control or neutral shoes and advised to wear them >6 hours/day over 6 months.
Primary and secondary outcome measures The primary outcome was change in average knee pain on walking over the previous week (11-point Numeric Rating Scale (NRS), 0–10) at 6 months. The secondary outcomes included other measures of knee pain, physical function, quality of life, participant-perceived change in pain and function, and physical activity.
Results We planned to recruit 110 participants (55 per arm) but ceased recruitment at 40 (n=18 motion control shoes, n=22 neutral shoes) due to COVID-19-related impacts. All 40 participants completed 6-month outcomes. There was no evidence that motion control shoes were superior to neutral shoes for the primary outcome of pain (mean between-group difference 0.4 NRS units, 95% CI −1.0 to 1.7) nor for any secondary outcome. The number of participants experiencing any adverse events was similar between groups (motion control shoes: n=5, 28%; neutral shoes: n=4, 18.2%) and were minor.
Conclusions Motion control shoes were not superior to neutral shoes in improving knee pain on walking in symptomatic radiographic lateral tibiofemoral joint OA. Further research is needed to identify effective treatments in this important but under-researched knee OA subgroup.
Trial registration number ACTRN12618001864213.
- Knee
- RHEUMATOLOGY
- Clinical trials
Data availability statement
Data are available upon reasonable request. Data that support findings of this study are available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
We used a robust randomised clinical trial design with blinded participants and assessors.
Our outcomes have strong clinimetric properties and are recommended for knee osteoarthritis clinical trials by international osteoarthritis guidelines.
We included sensitivity analyses to assess whether our findings changed when assuming full adherence to footwear.
We did not reach our intended sample size due to COVID-19-related impacts and thus we had reduced power to detect a clinically relevant between-group difference in our primary outcome.
Introduction
Knee osteoarthritis (OA) is a common and painful condition and a leading cause of global disability.1 The disease is chronic and has no cure; thus, people with knee OA have little choice but to self-manage their condition. Accordingly, advice about self-management is the cornerstone of conservative treatment, along with exercise and weight control.2 3 As abnormal biomechanics are central to OA disease pathogenesis,4 5 clinical guidelines advocate that clinicians provide advice on ‘appropriate’ footwear as part of core treatment for knee OA.2 6 However, there is scant evidence from clinical trials to guide footwear choice. Due to lack of robust clinical trials in this area, international OA organisations and the American Academy of Orthopaedic Surgeons have called for footwear trials as an OA research priority.2 6 7
To date, all clinical trials on footwear for knee OA have targeted people with medial knee OA, likely because the medial tibiofemoral (TF) compartment is affected by OA more often than the lateral compartment.8 However, 10%–55% of patients with knee OA have radiographic OA changes in the lateral TF joint,8–12 and there is evidence that coexisting lateral TF OA is associated with worse knee pain in people with mixed compartmental OA.13 Importantly, in people with medial knee OA, the aim of biomechanical interventions is to shift joint force distribution from the medial to the lateral TF compartment. However, the aim in people with lateral knee OA is to shift forces from the lateral to the medial TF compartment. Compared with medial TF OA, there is scant research evaluating non-surgical treatments for people with lateral TF OA. In particular, clinical trials that evaluate biomechanical interventions specifically designed to target the unique biomechanical needs of this lateral TF OA subgroup are urgently needed.
Biomechanical studies have shown that footwear with midsoles that are laterally stiff redistribute knee loads away from the medial towards the lateral TF compartment in people with medial knee OA.14 Conversely, footwear with medially stiff midsoles, such as ‘motion control’ shoes, shift knee loads towards the medial TF compartment,15 16 likely with concomitant reductions in lateral TF compartment load. Thus, it is possible that motion control footwear may improve symptoms in people with lateral knee OA. Although no randomised controlled trial (RCT) has assessed the effects of motion control shoes on symptoms in people with lateral compartment knee OA, there is some indirect clinical research to suggest that they may be effective. A small study of 30 women with symptomatic radiographic lateral knee OA and bilateral knee valgus deformity found that wearing medially wedged insoles (which have similar biomechanical effects on lateral TF joint loads to motion control shoes17) for 3–6 hours/day resulted in greater improvements in pain and other symptoms over 8 weeks compared with wearing flat insoles.18 Consequently, further research assessing the effects of motion control footwear in people with lateral knee OA is warranted to help inform footwear recommendations in international OA clinical guidelines and to guide clinical practice for this important but under-researched OA subgroup.
This study aimed to assess the effectiveness of motion control shoes in improving symptoms in people with lateral knee OA. We hypothesised that wearing motion control shoes would lead to greater reductions in walking knee pain, compared with wearing neutral walking shoes, over 6 months.
Patients and methods
Design
This was a two-arm, participant-blinded and assessor-blinded, pragmatic, comparative effectiveness, superiority RCT. It was prospectively registered with the Australian New Zealand Clinical Trials Registry (ACTRN12618001864213) and the protocol has been published.19 Participants provided informed consent.
Participants
Community-dwelling participants (Melbourne, Australia) were recruited using advertisements, including targeted invitations to participants on our research volunteer database who had known radiographically diagnosed lateral knee OA. Participants were eligible if they were aged >50 years; reported an average knee pain on walking over the previous week of >4 on an 11-point Numeric Rating Scale (NRS); had mild, moderate or severe radiographic knee OA (Kellgren and Lawrence (KL) grade 2–4)20; and had a grade of lateral TF joint space narrowing that was greater than the medial, determined using a radiographic atlas21 (where grade 0=no narrowing, 1=mild narrowing, 2=moderate narrowing, 3=severe narrowing). Participants were excluded if they reported knee pain for <3 months; had recent (past 6 months) or planned (next 6 months) knee surgery; or currently used foot orthoses, ankle/knee braces, customised shoes or other shoes worn regularly that would restrict their ability to wear the allocated study shoes for a minimum of 6 hours/day (eg, work boots). For participants with bilaterally eligible knees, the most painful was deemed the study knee. Full exclusion criteria are in the published protocol.19
Randomisation and masking
Participants were randomised in a 1:1 ratio. The randomisation schedule was prepared by a biostatistician with permuted block sizes of 6–12 and stratified by KL grades 2, 3 or 4. Allocation was concealed using password-protected software (REDCap) and was revealed by a researcher not involved in recruitment or outcome assessment. Participants were blinded and informed only that the trial was comparing the effects of two types of commercially available walking shoes on knee OA symptoms. We did not disclose the hypothesis or the specific footwear styles/characteristics (ie, motion control and neutral shoes) under investigation. As participants were blinded and the primary and secondary outcomes were self-reported, this trial was also assessor-blinded. The biostatisticians were blinded to all analyses.
Interventions
Motion control shoes
Black ASICS Gel-Kayano 25 shoes were chosen as the motion control shoes. These shoes have a dual density midsole which is stiffer medially compared with laterally, a feature that has previously been shown to shift knee loads towards the medial TF compartment.15 16
Neutral shoes
Black ASICS Gel-Nimbus 20 shoes were the neutral comparator shoes. These shoes have a uniformly stiff midsole and are visually similar to the motion control shoes. They are also similar in other key features including midsole foam and gel cushioning systems, an engineered mesh upper, shoe mass, and rearfoot, forefoot and heel drop heights.
Participants were fitted with their allocated shoes by a study researcher (BM). Participants were advised to commence wearing their allocated shoes for 2 hours on the first day and to increase wear time by 2 hours/day until they were wearing them as much as possible at a minimum of 6 hours/day over 6 months.
Outcome measures
Participants completed the baseline questionnaires on paper or electronically at the Department of Physiotherapy Gait Laboratory, The University of Melbourne. The 6-month follow-up questionnaire was completed either on paper or electronically at home.
The primary outcome was 6-month change in average knee pain on walking in the last week, assessed using an 11-point NRS, with the terminal descriptors ‘no pain’ (score=0) and ‘worst pain possible’ (score=10). This measure has strong clinimetric properties,22 is recommended for knee OA clinical trials23 and has a minimal clinically important difference (MCID) of 1.8 units.24
The secondary outcomes included changes in the Knee Injury and Osteoarthritis Outcome Score (KOOS) subscales of (1) physical function, (2) pain, (3) sport and recreation, (4) knee-related quality of life, and (5) patellofemoral pain and OA.25 Scores for each subscale were transformed to provide an overall value that ranged from 0 to 100 (where higher scores indicate better symptoms and function). Additional secondary outcomes included changes in quality of life, measured using the Assessment of Quality of Life 6D instrument26 (scored between −0.04 and 1.00; higher scores indicate better quality of life), and physical activity over the previous week, measured using the Physical Activity Scale for the Elderly27 (scored from 0 to over 400; higher scores indicate higher activity). We also assessed patient-perceived global rating of change in (1) pain and (2) function at 6 months, each measured using 7-point Likert scales, with the terminal descriptors ‘much worse’ to ‘much better’.28 Participants reporting they were ‘moderately better’ or ‘much better’ were classified as improved.
Descriptive measures included height, body mass and body mass index, age, gender, knee OA symptom duration, radiographic disease severity (using the KL scale20), anatomical knee alignment (measured in degrees from the knee X-ray29), employment status, treatment expectation (using a 5-point ordinal scale; anchors of ‘no effect at all’ to ‘complete recovery’), self-efficacy (using the Arthritis Self-Efficacy Scale30), cointervention use via a custom table (also assessed at 6 months), foot posture (using the Foot Posture Index31; scores range from −12 to +12, with higher scores indicating more pronated foot posture), foot mobility magnitude32 (in mm; higher values indicate greater mobility) and navicular drop33 (in mm; higher values indicate greater drop), and the motion control feature score of the participant’s usual (most commonly worn) pair of shoes (using the Footwear Assessment Tool15; scored 0–11, with higher scores indicating more motion control features).
We assessed adherence to allocated footwear using our successful strategies employed in prior footwear RCTs.34 35 Participants recorded how much they wore their allocated shoes (hours/day) for 7 consecutive days, for 1 week of every month, on logbooks. Those who averaged >6 hours/day over 6 months were classified as ‘adherent’. At 6 months, participants also rated their overall level of adherence with wearing their allocated shoes >6 hours/day using an 11-point NRS (with the terminal descriptors ‘shoes not worn at all’ and ‘shoes worn completely as instructed’) and indicated whether they stopped wearing the shoes during the study (yes or no). Participants who responded ‘Yes’ described when and why they stopped wearing their study shoes. Finally, adverse events (any problem experienced in the study knee or elsewhere in the body because of wearing the study shoes) were self-reported by participants at 6 months using a custom table.
Statistical analysis
We aimed a priori to detect a between-group difference in change in walking pain (the primary outcome) of 1.8 units (the MCID).24 We assumed a between-participant SD of 2.7 and a baseline to 6-month correlation of 0.21.34 35 Using analysis of covariance (ANCOVA) adjusted for baseline score, we needed 46 participants per arm to achieve 90% power to detect the MCID in change in walking knee pain. Allowing for 15% attrition, we aimed to recruit 55 people per arm (n=110 in total). However, due to ongoing COVID-19 restrictions in Melbourne (Australia) halting trial recruitment for a prolonged period of time and grant funding running out, recruitment was ceased with a final sample size of 40. Using ANCOVA adjusted for baseline score, we have 57.8% power to detect the MCID in change in walking knee pain (baseline minus 6 months), with a final sample size of 40 participants (assuming 20 participants per arm).
Main comparative analyses between groups were performed using intention-to-treat. As no primary outcome data were missing from the enrolled participants, multiple imputation was not applied and all analyses were performed on complete case data. Separate linear regression models were fit for each continuous outcome, including the primary outcome walking knee pain, with treatment group, outcome at baseline and stratifying variable (KL grade) as covariates. The results were calculated as the estimated mean (95% CI) difference in change (baseline minus 6 months) between groups. Regression assumptions of linearity and homoscedasticity were assessed using standard diagnostic plots. A sensitivity analysis, including all participants as randomised, estimated the complier average causal effects, which are the treatment effects on the primary outcome, assuming full adherence to shoe wear (classified as an average of >6 hours/day for 6 months, based on logbook data), using an instrumental variables approach (where randomisation was the instrument for adherence).36 Two-stage least squares models were fit: first, a model for observed adherence, including terms for randomised group, the outcome at baseline and the stratifying variable (KL grade); and second a model predicting the primary outcome, given observed adherence. Improvement based on global change scores and achievement of the MCID in improvement in walking knee pain (1.8 NRS units) were each compared between groups separately using logistic regression, adjusted for the stratifying variable (KL grade), with results reported as risk ratios and risk differences.
To assess whether the effect of shoe group on the primary outcome was moderated by KL grade, a linear regression model was fit for the primary outcome, with the outcome at baseline, treatment group and KL grade as covariates, including an interaction between treatment group and KL grade. To assess whether the effect of shoe group on the primary outcome was moderated by (1) Foot Posture Index score, (2) knee alignment or (3) KOOS patellofemoral pain and OA, separate linear regression models were fit for the primary outcome for each potential moderator, with the outcome at baseline, treatment group, relevant potential moderator and KL grade as covariates, including an interaction between treatment group and the potential moderator. Statistical analyses were performed using Stata V.16.1. The a priori statistical analysis plan is provided in the online supplemental file appendix 2.
Supplemental material
Patient and public involvement
Patients and the public were not involved in the design, conduct and dissemination of this research.
Results
Sample characteristics
Participant flow through the study is shown in figure 1. Between 29 November 2018 and 24 March 2020, we screened 261 people and enrolled 40 participants, predominantly recruited through targeted invitations to people with lateral knee OA in our research database (37 enrollees (from 65 screened) vs 3 recruited (from 196 screened) via advertising in the community). Due to COVID-19 causing extended lockdowns in Melbourne, Australia (totalling 23 weeks between 30 March and 12 May 2020 and between 8 July and 27 October 2020) and suspension of on-campus research activities, recruitment was postponed on 24 March 2020. Recruitment resumed on 13 June 2020, and by 12 November 2020 we had screened a further 10 participants without any further enrolment. The study was terminated early as it was deemed unfeasible to continue given the considerable number of participants still left to recruit, ongoing uncertainty regarding COVID-19 restrictions, poor community recruitment rates (no further recruitment possible from our volunteer database) and exhaustion of funding. At 6-month follow-up, all 40 (100%) enrolled participants had completed the primary outcome.
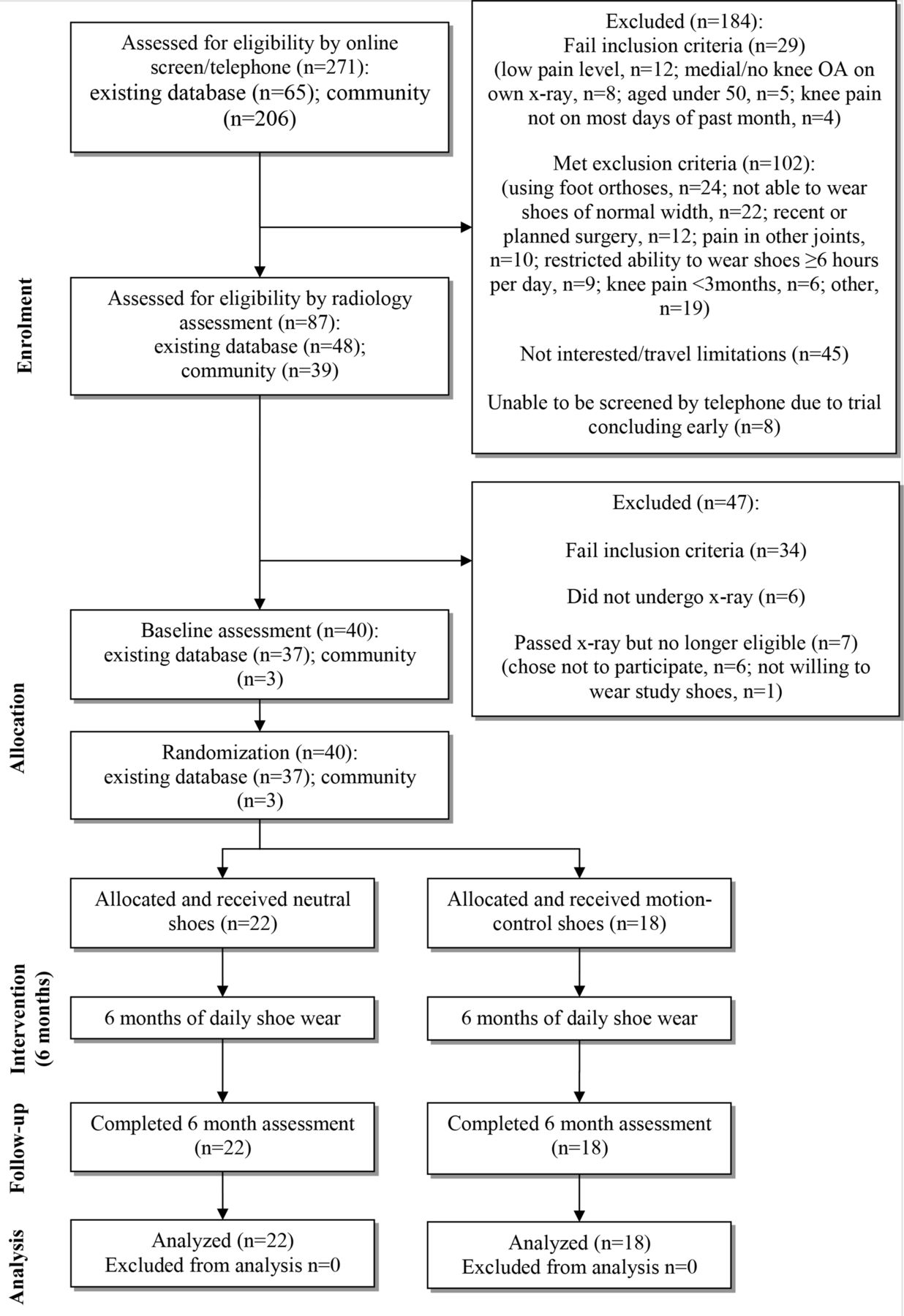
{kind=link}
Flow of participants through the trial. OA, osteoarthritis.
Participant characteristics were comparable between groups at baseline (table 1), except that a greater proportion of people in the neutral shoe group had a neutral foot posture (motion control 17% vs neutral 36%) and more people in the motion control group had a pronated foot posture (motion control 83% vs neutral 59%). Participants’ own usual footwear were similar across groups with respect to motion control features (table 1 and online supplemental appendix table 1), suggesting that on average people wore shoes with moderate amounts of motion control features. Treatment expectations were generally similar across groups prerandomisation and following shoe allocation (table 1).
Supplemental material
Baseline characteristics of participants by group
Adherence and adverse events
The mean (SD) allocated shoe wear was 7.0 (3.4) hours/day with motion control shoes and 8.0 (2.4) hours/day with neutral shoes (online supplemental appendix table 2). Ten participants (56%) were classified as adherent over 6 months with motion control shoes compared with 19 (86%) participants with neutral shoes. A similar number of participants in each footwear group reported adverse events (n=5 (28%) with motion control shoes, n=4 (18%) with neutral shoes), mostly knee pain (table 2). Cointervention use was similar between groups at baseline (table 1) and follow-up (table 2). One participant (6%) ceased wearing their motion control shoes due to a fractured ankle which was unrelated to the footwear (online supplemental appendix table 3).
Adverse events and cointerventions at follow-up according to group
Primary outcome
Table 3 summarises the primary outcome across time by group and presents the change in the primary outcome within and between groups. There was no evidence of a between-group difference in change in walking knee pain at 6 months (mean difference 0.4 NRS units, 95% CI −1.0 to 1.7, p=0.60). Sensitivity analyses found similar results when assuming full adherence (online supplemental appendix table 4).
Mean (SD) scores on continuous outcome measures across time by shoe group, mean change within groups and difference* in change between groups for continuous outcomes, using complete case data
Secondary outcomes
Table 3 summarises the continuous secondary outcomes across time by group and presents change in continuous secondary outcomes within and between groups. There was no evidence that motion control shoes were superior to neutral shoes for any continuous secondary outcome. Similar proportions (considering our small sample size) of participants reported global improvement across groups (table 4), with no significant difference between groups in the relative risk of improvement in pain (1.36, 95% CI 0.61 to 3.01, p=0.45) or function (1.43, 95% CI 0.50 to 4.10, p=0.50). The number of participants achieving the MCID of 1.8 NRS units in pain and the relative risk of achieving the MCID were also similar between groups (1.28, 95% CI 0.74 to 2.24, p=0.38) (table 4).
Number (percentage) of participants reporting global improvement or achieving an improvement of 1.8 NRS units in the primary outcome (change in knee pain on walking; baseline minus 6 months), and relative risks* and risk differences*
Subgroup analyses
The effect of the allocated shoe group on the primary outcome walking knee pain was not found to be moderated by any of the prespecified variables of radiographic disease severity, Foot Posture Index, radiographic knee alignment or KOOS patellofemoral pain, and the OA subscale score (online supplemental appendix tables 5 and 6).
Discussion
This RCT found that motion control shoes were not superior to neutral shoes in reducing knee pain on walking in people with lateral knee OA. The average within-group changes failed to demonstrate clinically meaningful improvements in knee pain for either group of footwear. Motion control shoes were not superior to neutral shoes for any secondary outcome, and a similar proportion of participants in each group reported global improvements in pain (motion control 33% vs neutral 46%) and function (motion control 22% vs neutral 32%) and achieved MCID in NRS walking pain (motion control 50% vs neutral 64%). However, we had reduced power (57.8%) to detect the MCID in between-group difference in change in our primary outcome as we did not reach our intended sample size, which may explain our findings, although the observed effect estimate was well below what is considered clinically meaningful and the MCID was not contained within the 95% CIs. These findings provide preliminary evidence to suggest motion control shoes may not be beneficial in reducing symptoms associated with predominantly lateral knee OA compared with neutral shoes. However, adequately powered clinical trials are required to confirm our results.
Although no previous clinical trial has investigated the effects of footwear in people with lateral knee OA, our findings are not consistent with the only other similar trial conducted, which evaluated shoe insoles over 8 weeks. In a previous RCT with a smaller sample size than ours (n=30), medially wedged insoles, but not flat neutral insoles, significantly reduced knee pain with movement (mean (SD) baseline and 8-week values for medial wedges: from 8.1 (1.5) to 4.2 (2.4); flat insoles: from 6.9 (2.6) to 6.4 (2.7)) and at rest (medial wedges: from 5.1 (2.3) to 2.7 (2.4); flat insoles: from 3.3 (2.2) to 3.1 (2.5)) in women with lateral knee OA.18 However, the average between-group differences were not reported in that study and thus it is possible that no significant between-group differences were observed. Although adherence rates were not reported in that study, the different outcomes may also be due to the lower proportion of participants being classified as adherent wearing motion control shoes (56%) compared with neutral walking shoes (86%) in our study. We did not identify any between-group differences in the primary outcome when assuming full adherence; however, these results assumed that participants had to wear motion control shoes for an average of >6 hours/day for 6 months in order to benefit from them. To our knowledge, no study has investigated the symptomatic effects of knee bracing or any other biomechanical intervention in people with lateral TF joint OA.
Biomechanical research has demonstrated that motion control shoes,16 medially wedged insoles37 and medial arch supports38 redistribute knee joint loading towards the medial TF compartment, likely unloading the lateral TF compartment. The lack of symptomatic benefit with motion control shoes in our study could suggest that these shoes are not effective in unloading the lateral TF compartment, that joint load reductions are not enough to result in clinical meaningful reductions in pain, and/or that relationships between lateral TF joint loads and pain are not strong. Although there has been no research evaluating the relationship between lateral TF joint loads and severity of knee pain in people with lateral TF OA, previous research by us and others on medial compartment knee OA has shown limited, and at times conflicting, associations between knee pain and medial TF joint loads.39 40 Thus, it is perhaps not surprising that our previous RCT which tested footwear designed specifically to reduce medial TF loads found that they were not superior to conventional walking shoes in reducing walking knee pain in people with medial knee OA.34 Further research is needed to investigate the associations between lateral TF joint loads and knee pain severity in people with lateral knee OA and whether interventions that produce larger reductions in knee load (eg, high tibial osteotomy and knee bracing) can effectively reduce knee pain in this population.
We failed to reach our intended sample size of 110 participants due to slow recruitment rates, impacting feasibility to complete the trial before funding was exhausted. This was largely because on-campus research was suspended at our university during 23 weeks of COVID-19-related lockdowns in 2020 in Australia. Nonetheless, it is worth highlighting that our recruitment rate prior to trial suspension was very slow (2.5 participants enrolled per month) compared with our previous footwear trials in people with medial TF OA (which enrolled 5.9–7.5 participants per month34 35). The much slower recruitment rate in the current study reflects the lower prevalence of lateral (15%) compared with medial (27%) TF OA in the community.41 It is also worth noting that, when recruiting people with lateral TF OA from the community, X-ray screening costs can be substantial given that 58% of people recruited from community sources were excluded on the basis of not having a grade of lateral TF joint space narrowing that was greater than the medial. In the present study, our most successful recruitment strategy was recruiting from our research database of volunteers, which included participants who had already undergone X-rays for our prior trials and were known to have lateral TF OA. In fact, 93% (37 of 40 participants) of our final sample were recruited this way (figure 1), and our recruitment of only 3 participants from the 206 people screened from the community resulted in a recruitment rate of only 1.46% from this source. Thus, to recruit the final 70 participants from the community would have required screening an additional 1522 participants. Future studies should take these recruitment rates into consideration when planning clinical trials in people with predominantly lateral knee OA.
Despite our small sample size, our study is the first to assess any type of footwear for people with predominantly lateral knee OA. Our findings will be important for researchers undertaking meta-analyses of biomechanical interventions for knee OA,42 and in particular will yield unique data to evaluate the efficacy of interventions in the under-researched subgroup of people with lateral TF OA. Thus, our findings also have the potential to influence knee OA clinical guidelines, most of which advocate footwear use on the basis of expert opinion alone due to the dearth of footwear RCTs in knee OA.2 6 Other strengths include our robust RCT design and the use of outcome measures recommended for knee OA clinical trials, blinded participants and assessors, excellent retention, and the inclusion of sensitivity and moderator analyses. There were also some limitations, the principal one being that our sample size was smaller than planned. As such, our trial had reduced statistical power to detect between-group differences. We evaluated a single motion control shoe model and thus our findings cannot be generalised to other motion control shoes. Similarly, the addition of medial wedges or arch support to the motion control shoes may exert greater symptomatic benefits than motion control shoes alone.
In conclusion, motion control shoes were not superior to neutral walking shoes in reducing walking knee pain in people with symptomatic lateral TF joint OA. Given the limited clinical trial evidence in people with lateral knee OA, further research is needed to confirm the findings and to identify effective treatments for this important but under-researched subgroup of patients with knee OA.
Data availability statement
Data are available upon reasonable request. Data that support findings of this study are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by The University of Melbourne Human Research Ethics Committee (#1852787). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @HinmanRana
Contributors KLP and RSH conceived the idea for the study. KLP led the trial. KLP and RSH designed the trial protocol, with input from KLB, BM, PKC, FM and KEL. FM and KEL formulated and were responsible for the statistical analysis plan and conducted the statistical analyses. KLP drafted the manuscript and all authors provided input and approved the final version. KLP accepts full responsibility for the finished work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding This study was funded by the National Health and Medical Research Council (Project Grant #1124418). KLP is supported by a National Health and Medical Research Council Emerging Leadership Investigator Grant (#1174229). KLB is supported by a National Health and Medical Research Council Leadership Investigator Grant (#1174431). RSH is supported by a National Health and Medical Research Council Senior Research Fellowship (#1154217).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.