Article Text

Abstract
Introduction Attention deficit hyperactivity disorder (ADHD) is characterised by significant deficits in attention and inhibition. These deficits are associated with negative sequelae that emerge in childhood and often continue throughout adolescence. Despite these difficulties adolescents with ADHD often demonstrate poor treatment compliance with traditional interventions (eg, psychostimulant medication). Virtual reality (VR) presents an innovative means of delivering engaging cognitive interventions for adolescents with ADHD and offers the potential to improve compliance with such interventions. The current parallel, randomised controlled trial aims to evaluate the effects of a VR intervention (Alfi) designed to improve inhibition in adolescents with ADHD.
Methods and analysis A sample of 100 adolescents (aged 13–17) with elevated ADHD symptoms will be recruited from secondary schools and ADHD organisations located in the state of Victoria, Australia. Participants will be randomly assigned to either an 8-week VR intervention or a usual care control. The VR intervention involves the completion of 14 sessions, each 20 min in duration. Participants will complete computerised assessments of inhibition and risk-taking preintervention and immediately postintervention. Parents/guardians will complete online questionnaires about their child’s ADHD symptoms and social functioning at each of these timepoints. The primary outcome is change in inhibition performance in adolescents who received the intervention from preintervention to postintervention compared with adolescents in the control condition. Secondary outcomes include change in risk-taking, ADHD symptoms and social functioning in adolescents who received the intervention from preintervention to postintervention compared with adolescents in the control condition. If the intervention is shown to be effective, it may offer a supplementary approach to traditional interventions for adolescents with ADHD experiencing inhibitory control difficulties.
Ethics and dissemination This trial has ethics approval from the Monash University Human Research Ethics Committee (HREC) (21530) and the Victorian Department of Education and Training HREC (2020_004271). Results will be disseminated through peer-reviewed journals, conference proceedings and community activities. Individual summaries of the results will be provided to participants on request.
Trial registration number ACTRN12620000647932.
- Child & adolescent psychiatry
- Impulse control disorders
- Clinical trials
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The intervention used in the study is a novel virtual reality programme designed to train inhibitory control in adolescents with elevated attention deficit hyperactivity disorder symptoms.
The trial follows an established framework (the Obesity-Related Behavioral Intervention Trials [ORBIT] model) for designing and evaluating interventions.
The study includes measures to assess the near and far transfer of trained skills.
The inclusion of participants with autism spectrum disorder and other common comorbidities contributes to the ecological validity of the findings.
A limitation of the study is the use of a usual care active control group rather than a placebo virtual reality task due to ethical concerns.
Introduction
Attention deficit hyperactivity disorder (ADHD) is a common childhood disorder with a prevalence of approximately 7% among school-aged children.1 ADHD is characterised by significant cognitive and behavioural deficits, with diagnosis based on age-inappropriate and impairing levels of inattention and/or hyperactivity and impulsivity.2 These symptoms have a significant impact on daily functioning and are associated with a range of negative sequelae, including poor academic achievement, social difficulties, mental health problems and overall poorer quality of life.3
Not only are the difficulties associated with ADHD far-reaching, they are also enduring. Symptoms and functional impairment emerge during childhood and often persist throughout adolescence and beyond, with an estimated prevalence of 3% for adults with ADHD.4 Despite the significant, long-lasting consequences of ADHD symptoms, treatment compliance remains a challenge in adolescents with ADHD. While pharmacological treatments have efficacy in managing ADHD symptoms,5 it is estimated that around half of adolescents with ADHD exhibit some non-compliance.6 High levels of non-compliance coupled with the social and academic consequences of unmanaged ADHD symptoms necessitate the development of appealing and engaging treatment options that can complement and supplement pharmacological treatment.
Cognitive training has been suggested as an engaging and potentially effective intervention for many clinical populations, including children with ADHD, and may offer an adjunctive intervention to medication.7 8 Cognitive training is based on the premise of neural plasticity and asserts that deficits in cognitive functions can be improved long term through repeated, targeted training.9 Many cognitive training interventions have targeted cognitive difficulties in ADHD with mixed results.9 10 These interventions have predominantly focused on improving cognitive skills such as working memory.8 However, a large body of research indicates that inhibition is a central cognitive deficit in ADHD.11 12 Inhibition can be defined as the voluntary control of responses and stimuli, and deficits in inhibition can contribute to behavioural and social problems in adolescents with ADHD.13 Previous investigations of computerised inhibitory control training in children with ADHD have shown positive impacts of the intervention on symptoms of ADHD.14 However, to date no study has investigated the potential benefits of inhibition training in adolescents with ADHD.
Computer-based and digital training tools offer an innovative platform to deliver these cognitive interventions, with one particularly engaging and emerging tool being virtual reality (VR). VR provides an immersive environment that helps to limit extraneous distractions, making it a promising tool to target cognitive functioning.15 For children and adolescents with ADHD, VR is particularly beneficial due to its novel and dynamic format which allows for better focus and concentration on a task by excluding distractions in the real world.
There has been increasing interest in the use of VR as a means of delivering assessments and interventions in ADHD. While there are no known trials of VR-based interventions for adolescents with ADHD, the results of VR-based assessment studies have been promising.16–18 VR-delivered assessment tasks such as the continuous performance task (CPT), a common measure of assessing sustained attention, demonstrate greater ability to differentiate between children with and without ADHD and increased ecological validity when compared with traditional versions of the task.16–19 While traditional CPT tasks in children with and without ADHD tend to show difference in reaction time of medium effect size, in VR these differences were of large effect size.17 This increased sensitivity and ecological validity has been one of the key drivers for the use of VR in children with ADHD. Furthermore, these studies provide evidence of the usability and tolerability of VR in adolescents with ADHD.
Objectives
Although cognitive training interventions delivered via VR show considerable promise as a means of remediating cognitive deficits in adolescents with ADHD,20 the novel nature of VR and the lack of VR-based interventions for ADHD mean that it is yet to be widely tested. The Alfi Virtual Reality (Alfi VR) programme aims to fill this gap. Alfi VR was designed to train inhibitory control in adolescents with ADHD. While an initial proof-of-concept trial has been completed in typically developing adolescents, Alfi VR is yet to be trialled in adolescents with significant inhibitory control deficits, such as those with ADHD. The primary objective of this pilot study is therefore to assess whether completion of the Alfi VR programme is associated with any change in inhibitory control in adolescents with ADHD as compared with usual care.
It is hypothesised that Alfi VR will be associated with significant improvements in the primary outcome measure of response inhibition when compared with usual care. The secondary objective of the trial is to assess for any improvements in related, untrained domains such as impulsivity, ADHD symptoms, emotion regulation and social skills following completion of the Alfi VR intervention as this will help determine whether training leads to changes in functional outcomes. An additional exploratory analysis will be conducted to assess the impact of sociodemographic (eg, family environment and socioeconomic status) and prognostic (eg, social anxiety) factors on change in the primary outcome from preintervention to postintervention.
Methods and analysis
Study design and setting
The Alfi VR trial is an unblinded, randomised controlled trial with two parallel groups and equal allocation ratio (1:1). The effects of the VR intervention compared with a usual care control will be assessed preintervention (week 1) and immediately postintervention (week 9). The trial will be conducted and reported in accordance with the Consolidated Standards of Reporting Trials statement.
The trial will be run across two urban, Australian community-based settings. Data collection and intervention sessions will be run at participating government and independent schools across metropolitan Melbourne and at Monash University. The trial commenced in February 2020, with an estimated completion date of August 2022.
Patient and public involvement
The public were able to provide feedback on the intervention during a proof-of-concept trial of Alfi VR. Proof-of-concept phases represent a key step in ensuring the appropriateness of the intervention prior to undertaking a pilot study. Typically developing teenagers from Melbourne, Australia were invited to participate in three Alfi training sessions, after which they provided feedback on the enjoyability, usability and accessibility of the training programme. This feedback was incorporated into the latest build of Alfi VR, which is being used for this trial, and was informed the timing and number of sessions in the current trial. Details of dissemination of results to participants and the public can be found under the Ethics and dissemination section.
Eligibility criteria
The study is targeted at adolescents, which is defined by the WHO as children between 13 and 19 years of age.21 Children will be eligible to participate in the trial if they are (1) aged between 13 years and 17 years 11 months at the time of enrolment into the study and (2) have elevated ADHD symptoms. Elevated symptoms are defined as t-scores above 58 on either the inattention or hyperactive/impulsive scales, or a t-score of above 58 on either the ADHD inattentive or ADHD hyperactive/impulsive Diagnostic and Statistical Manual of Mental Disorders: Text Revision (DSMIV-TR) scales of the Conners-3 Parent Rating Scale. Children will be excluded if they have (1) a diagnosis of developmental delay or borderline intellectual delay (defined as a Full Scale IQ of less than 80 on the Kaufman Brief Intelligence Test - Second Edition(KBIT-2)); (2) a history of neurological impairment including epilepsy, acquired brain injury or any history of seizures; and (3) any sensory or motor impairment or comorbid diagnosis that may prevent them from completing the intervention or understanding study instructions (eg, visual impairment, paralysis, severe obsessive-compulsive disorder). Screening questions pertaining to all exclusion criteria will be included in the demographic questionnaire, and clarification from parents/caregivers will be sought where responses are ambiguous or the level of impairment is unclear. Details of current medication use will be obtained through the demographic questionnaire. Children who are on a stable dosage will not be excluded from enrolling in the study; however, changes to dose or commencement of medication will result in withdrawal from the trial (see the Discontinuation criteria section).
Intervention
The intervention is an inhibitory control training intervention called Alfi VR. The Alfi VR intervention uses immersive VR technology to deliver a game-based version of an anticipated response stop-signal task.22 This paradigm has been used in studies of children with ADHD previously, with children with ADHD showing deficits on this task when compared with typically developing (TD) controls.23 Anticipated response versions of the stop-signal task require a fixed go response initiation time, rather than a speeded response as in reaction time versions of the stop-signal task. This affords greater control over the timing of the go response, and by extension the timing of stop cues relative to the go response.24 Furthermore this paradigm has been well characterised as targeting behavioural response inhibition.24 The intervention is graded in difficulty and includes task conditions that train reactive and proactive inhibition,25–30 as well as selective inhibition.31–35 As such, the Alfi VR intervention is immersive and challenging and targets core cognitive processes involved in inhibitory control throughout the course of training.
Adolescents are equipped with an HTC Vive VR headset and two controllers, with base stations mounted on stands. Within the programme users play the role of a wizard who must protect a magic crystal from dragon attacks by casting spells. Users are required to hold down the triggers on both controllers at the start of each trial. In Go trials, users release the triggers to cast spells at certain times to defuse the dragon’s fireball attacks (figure 1A). At the start of the intervention, the dragon’s fireball attacks occur on both sides, requiring users to release both triggers on the controllers. As the intervention progresses, the Stop trials are introduced requiring the user to inhibit their primed response to simultaneously release both fireballs on a proportion of trials (25%). In the first block that includes the Stop trials, wizards are introduced who are also able to cast spells and defuse the fireballs. When a wizard has defused a fireball, users must inhibit any initiated responses (eg, trigger releases), otherwise the fireball will become active once more (figure 1B). The timing of the wizard spell represents the stop signal delay (SSD). The SSD represents the amount of time between the onset of the Go signal and the Stop signal, with a longer SSD often associated with increased errors.36 The tracking method is used to adjust the SSD, increasing and decreasing by 33 ms (approximately two screen refreshes) depending on the correct or incorrect responding on the previous Stop trial.24

Trial structure and timing. 1a. Go trials; 1b. Bimanual stop trials; 1c. Selective stop trials; 1d. Stop trials with cues (bimanual shown). L = Left; R = Right.
As the levels increase in difficulty, the fireballs may also occur from either the right or left side only, requiring one trigger to be held down while the other is released (selective inhibition; figure 1C), and cues are introduced which indicate the increased likelihood of the next trial being a stop trial (proactive inhibition; figure 1D). The use of a bimanual and selective paradigm requires the participant to attend to multiple streams of information simultaneously, increasing the ecological validity of the training. Furthermore, the introduction of cues in later trials (indicating the increased likelihood of a stop trial) allows for proactive inhibition to be trained in addition to reactive inhibition.
By providing variability in trial types and having an adaptive SSD, the potential for maintaining participant engagement is maximised. These variables ensure that the task remains challenging without becoming too difficult. Participants receive feedback on all responses, which includes corrective feedback when participants respond incorrectly or fail to respond. To provide motivation throughout training sessions, participants can monitor their progress and ingame statistics and receive virtual ingame rewards that can be used to personalise certain aspects of gameplay.
Researchers will observe and monitor participant progress throughout the session via the computer monitor. Training sessions take 20 min to complete, with each block within the session lasting approximately 6 min. The individual blocks comprise a 3:1 ratio of Go trials (75%) to Stop trials (25%). Participants will complete the Alfi programme twice per week for 8 weeks, totalling 16 training sessions. The dates and times of all training sessions are recorded to monitor treatment adherence, with treatment compliance defined as having completed 12 of the 16 allocated training sessions (75%).
Discontinuation criteria
Participants may be withdrawn from the trial if they (1) commence any medication or therapy for the purpose of addressing ADHD symptoms or if there are any changes to their current treatment (eg, increase in medication dosage); (2) experience recurrent or persistent symptoms of cybersickness; or (3) experience a serious adverse event.
Outcomes
Primary outcome
All outcome measures were designed to be used with adolescents and are appropriate for use in children with ADHD. The first primary outcome of the study will be the difference in pretraining to post-training response inhibition between the Alfi VR intervention group and the control group. Response inhibition will be measured using an anticipated response stop-signal task designed to assess the ability to inhibit prepotent responses. This task has been designed in line with recommendations in the 2019 consensus statement on stop-signal tasks37 and is similar in structure to the Alfi VR intervention and our previous work.22 24 26 The anticipated response task is completed on a laptop computer. The task comprises a short practice block of 5 Go trials, followed by a block of 30 Go trials. Participants are then presented with another practice block of 10 trials, of which 5 are Stop trials. These practice trials are followed by 5 blocks of 40 trials, each comprising 25% Stop trials. The tracking method is used to adjust the SSD with a step size of 25 ms, initialised at 500 ms, and bounds of 50 ms and 775 ms.
During the task participants are required to focus on the yellow target markers. In Go trials, participants must then hold down the space bar and release the space bar once the indicator bar the yellow target. In Stop trials, the indicator bar stops prematurely, requiring participants to inhibit the primed response to release the response key. Reactive response inhibition will be assessed by determining the stop-signal response time (SSRT) using the integration method, with reductions in SSRT indicative of improvements in inhibitory control. Proactive response inhibition will be calculated by comparing the Go reaction time between the block containing only Go trials and the blocks comprising both Stop and Go trials.
Secondary outcomes
The secondary outcome measures are outlined in table 1. These measures cover a range of domains commonly impaired in ADHD, including behavioural attention, impulsivity, risk-taking behaviour, autism features and social skill. These measures have been included to assess whether far transfer occurs following completion of the intervention.
Schedule of measures
Additional measures
Additional measures have been included based on previous research which highlights the impact of factors such as anxiety and socioeconomic status on cognitive development and training outcomes.38 39 Measures of autism symptoms and emotional and behavioural concerns have also been included due to the high comorbidity between ADHD and other disorders that may be associated with differences and changes in inhibitory control, such as autism spectrum disorder (ASD), oppositional defiant disorder and mood disorders.40–42 The psychometric properties of all measures are outlined in table 2.
Psychometric properties of measures
Sample size calculation
A priori power analysis was conducted in G*Power V.3.1 to determine the necessary sample size required to detect significant changes in inhibitory control from pretraining (baseline) to post-training between groups. An estimated effect size of 0.3 was used based on the results of a small proof-of-concept study of the Alfi intervention in typically developing adolescents conducted by the authors. A total sample size of 97 was required for a power of 90%. The study will therefore aim to recruit 100 participants, with 50 per group assuming a 1:1 allocation ratio. This is consistent with previous trials evaluating cognitive training interventions in individuals with ADHD.43
Recruitment
Participants will be recruited through a number of avenues. The primary recruitment pathway will be through local government and independent schools. Researchers will contact schools within 40 km of the Monash University Clayton campus. A sampling matrix will be used to ensure that participants are recruited from a range of geographical regions across metropolitan Melbourne and to ensure diversity within the sample with regard to socioeconomic status. Interested schools will be provided with study information packs to disseminate to students and their families.
Participants will additionally be recruited via ADHD-related websites, community groups and ADHD-related social media groups. Due to the requirement for intervention sessions to take place at schools or at Monash University, it is anticipated that participants will predominantly reside in metropolitan Melbourne.
Interested families will contact the research team directly via phone or email and will be given the opportunity to discuss the study further. If families complete the informed consent form, they will be invited to participate in screening. Screening will take place online, with parents emailed a link to the demographic questionnaire and the Conners-3 Parent Rating Scale, which will be used to confirm clinical diagnosis of ADHD. Should children meet all the inclusion criteria and none of the exclusion criteria, they will be accepted into the trial.
Participant timeline/procedure
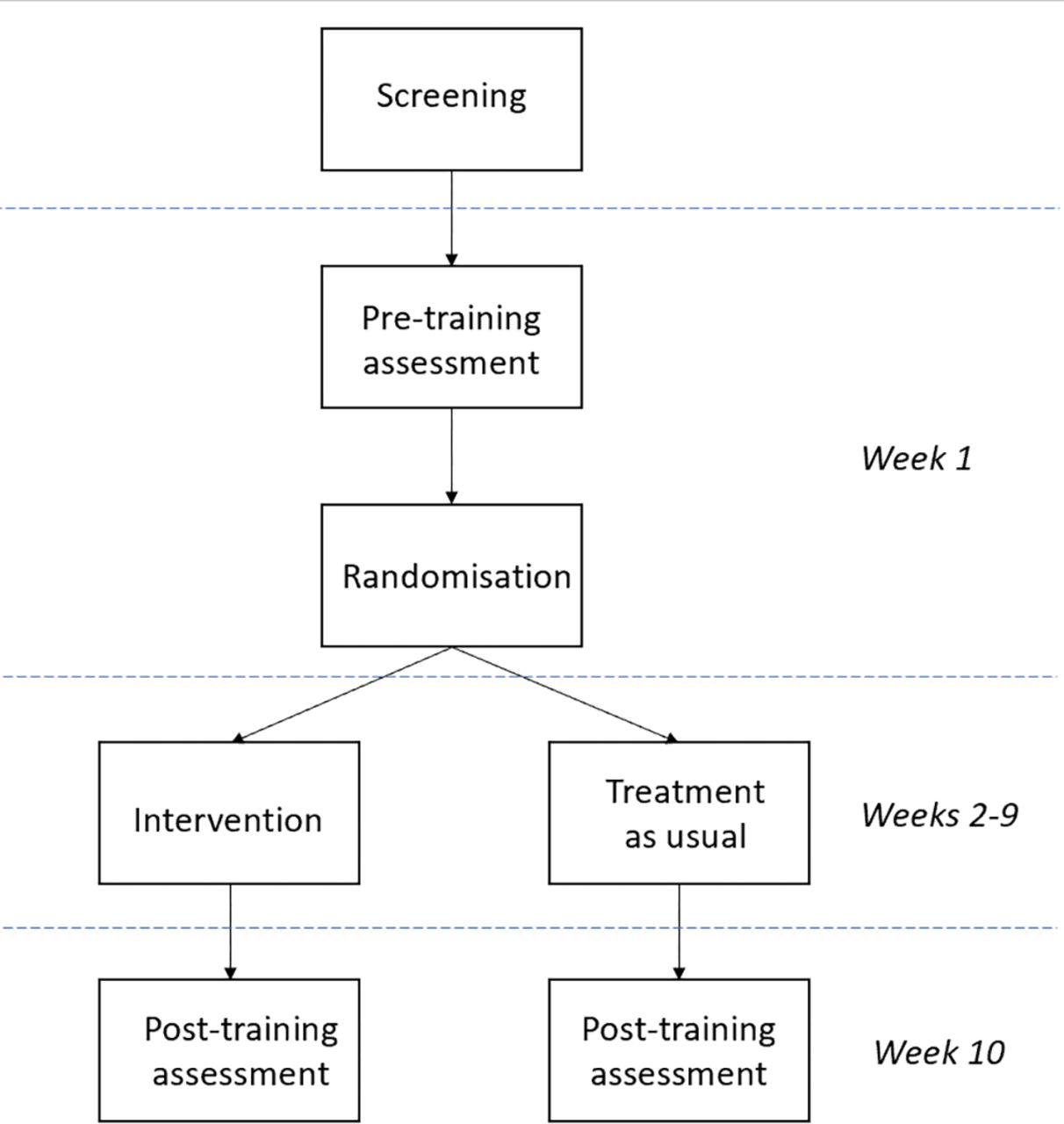
The timing of screening, randomisation, assessments and intervention can be seen in figure 2. The pretraining intervention will take place a week prior to the commencement of the intervention. The intervention period will run for 8 weeks, with the post-training assessment taking place a week after completion of the intervention. Refer to figure 2 for the intervention and assessment schedule.
{kind=link}
{kind=link}
Intervention and assessment schedule.
Allocation
Participants will be randomised following completion of the pretesting assessment. Block randomisation will be used, with blocks of four. As there are significant sex differences within ADHD,44 45 randomisation will be stratified by sex to ensure an even distribution of boys and girls between the intervention and control groups. Randomisation will be completed by a member of the research team using R. Group allocation will be communicated to participants and their families and recorded in the study database.
Concealment
Group allocation will be completed by an independent researcher who is not a member of the trial study team to reduce bias. A randomisation sequence will be generated in RStudio and printed onto folded cards with the group allocation listed on the inside. Following enrolment into the study, the participants’ study identification will be provided to the independent researcher, who will record it on the outside of the card and provide it to the trial researcher in a sealed opaque envelope. Following completion of the pretraining assessment, the envelope will be opened and the participant assigned to their allocated group.
Statistical methods
Data obtained during screening will be analysed to determine study eligibility; no further interim analysis will be conducted. At the completion of the trial, study data will be analysed using an intention-to-treat approach, meaning that outcome data for all participants will be included regardless of treatment compliance. Primary outcome data will be analysed in SPSS version 27 using analysis of covariance (ANCOVA) to examine changes in response inhibition from pretraining to post-training between groups. ANCOVA will allow for inclusion of covariates to minimise the impact of extraneous variables such as age, ASD traits (as measured by the Social Responsiveness Scale, 2nd Edition (SRS-2)) or cognitive function (as measured by the KBIT-2), where indicated. Multivariate analysis of covariance will be used to analyse differences in secondary outcome measures, with post-hoc tests completed for any significant results.
After completion of the primary intention-to-treat analysis, a sensitivity analysis using a per-protocol approach will be conducted to assess the robustness of the results and to determine whether there are any differences in outcomes between participants who met the criteria for programme compliance and those who did not.46 The management of missing data will be dependent on the amount of data missing and the pattern of missing data.47
Data collection/data management
Data will be collected by researchers trained in the administration and scoring of the study assessment measures. In week 1 families will be emailed links to the pretraining surveys for completion by the participant and a parent. These surveys take approximately 25 min to complete and responses can be saved and the survey resumed at a later time if required. Participants will concurrently complete the pretraining assessment session at week 1. This session will take place face-to-face and will be facilitated by two researchers. Following the 8-week intervention period, families will be emailed links to the post-training surveys and participants will concurrently complete the face-to-face post-training assessment session. These surveys must be completed within 2 weeks of completing the intervention. Study progress will be recorded for each participant in the study database.
Participant data will comprise a combination of electronic and paper-based records. Electronic data will be recorded and stored within a secure Research Electronic Data Capture (REDCap) database. Paper-based data will be identified by participant number only and will be stored securely and retained in accordance with relevant government regulations. As the study is unblinded a data monitoring committee was not deemed necessary. This role will be undertaken by the study team.
Ethics and dissemination
The Alfi VR trial has ethics approval from the Monash University Human Research Ethics Committee (HREC) (project ID: 21530) and the Victorian Department of Education and Training HREC. The Alfi VR trial comprises adolescents aged 13–17 years and therefore written informed consent will be obtained from the parent or primary caregiver in addition to assent from adolescents.
As the Alfi VR intervention will be completed during scheduled class time, ethical concerns regarding removing children from the classroom to complete an inactive VR task with no perceivable benefits prevent the use of an active control programme. The use of a usual care active control group mitigates this concern by not disadvantaging children through missed educational activities.
At the conclusion of the study parents will be provided with a summary of their child’s individual performance on request. Researchers will offer to run information sessions at each participating school to share deidentified study findings with participants and their families. A community-based seminar will also be organised to disseminate study findings, and findings will be shared on the study website for public access. The findings of the trial will be published in journals and conference proceedings and will form part of a PhD thesis. All published and disseminated data will be deidentified and analysed as a group to ensure confidentiality and protect the privacy of participants.
The protocol and study information can be publicly accessed through the Australian New Zealand Clinical Trials Registry. Enrolled participants will be notified of any relevant changes to the protocol.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to thank Ms Rachael Martin for her assistance with manuscript preparation.
References
Footnotes
EM and HK are joint first authors.
Contributors HK and KC were responsible for the initial conception of the work. EM and DC contributed to study design, with input from MAB and JC. EM wrote the initial manuscript draft, with subsequent drafts written by EM and with input from HK. DC, JC, AA, MAB, HK and KC reviewed and provided feedback on all drafts. Revision was completed by EM and HK. The revised and final manuscript was approved by all authors.
Funding This work was supported by a philanthropic donation from the 5Point Foundation and Australian Government Research Training Program (RTP) scholarships awarded to EM.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods and analysis section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.