Article Text

Abstract
Introduction About 70% of patients with asthma and/or chronic obstructive pulmonary disease (COPD) use their inhaled medication incorrectly, leading to reduced disease control, higher healthcare use and costs. Adequate guidance from the pharmacy team from first dispense onwards can benefit patients in the long run. We propose an intervention (‘On TRACk’) to improve medication adherence and inhaler technique of adult patients with asthma and/or COPD. This intervention focuses on training pharmacy technicians (PTs) in patient-centred communication and inhalation instruction skills. In addition, patients are actively involved in refill consultations at the pharmacy. The aim of this study is to improve inhaler technique and better inhaled medication adherence among patients with asthma and/or COPD. This paper describes the study protocol.
Methods and analysis A cluster randomised controlled trial (RCT) with an intervention and control group of 15 pharmacies each will be conducted. Per intervention pharmacy, two PTs will be trained online. Each PT will include five patients who will prepare their second and third dispense counselling sessions by selecting three topics they wish to discuss. Pharmacies in the control cluster provide usual care. In total, 300 patients (150 per group) will be included. Up to 12 months after inclusion, patients complete 3-monthly follow-up questionnaires. Both a process evaluation and a cost-effectiveness analysis will be performed alongside the trial. Trial effectiveness on the patient level will be evaluated after the 12-month follow-up period.
Patient data will be collected through questionnaires and pharmacy refill data. Patients’ inhaler technique will be visually assessed by PTs. Semistructured interviews with PTs and patients will be conducted regarding implementation and fidelity. Direct and indirect health costs will be collected to assess cost-effectiveness.
The primary outcome is adherence to inhalation maintenance medication measured with pharmacy refill data. Secondary outcomes are inhaler technique, persistence, patients’ attitudes towards medication, self-efficacy in medication use and communication with their PTs.
Ethics and dissemination The study was approved by the Vrije Universiteit Amsterdam Ethics Committee (number: 2020.358). Results will be presented at (inter)national conferences and published in peer-reviewed journals. If proven to be (cost-)effective, the intervention should be considered for reimbursement and implementation in Dutch community pharmacies.
Trial registration number NL9750.
- RESPIRATORY MEDICINE (see Thoracic Medicine)
- MEDICAL EDUCATION & TRAINING
- Asthma
- Chronic airways disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- RESPIRATORY MEDICINE (see Thoracic Medicine)
- MEDICAL EDUCATION & TRAINING
- Asthma
- Chronic airways disease
STRENGTHS AND LIMITATIONS OF THIS STUDY
The On TRACk intervention combines two previously proven successful interventions, being a pharmacy technician (PT’s) communication skills training and patients’ consult preparation.
The intervention matches regular medication dispense moments, which facilitates implementation in pharmacy practice, has repeated evaluations of patients inhaler technique and a long-term follow-up of 12 months.
This study combines multiple outcome measures; validated patient-reported outcome measures, pharmacy refill data and PT reported inhaler technique scores.
There is a possible selection bias in the pharmacies that eventually partake due to inclusion of motivated pharmacists and technicians.
The online character of the On TRACk intervention might prevent participation from patients with insufficient (digital) health literacy.
Introduction
About 70% of patients with asthma and/or chronic obstructive pulmonary disease (COPD) do not use their inhaler medication correctly, leading to reduced disease control, higher risk of exacerbations resulting in reduced quality of life, healthcare use, work absence and increased healthcare costs.1 2 The Global Initiative for Asthma (GINA) and the Global Initiative for Chronic Obstructive Lung Disease report identified incorrect inhaler technique and poor adherence as key factors that affect disease control.3 4 Poor inhaler technique is mostly unintended as patients are often unaware of their incorrect inhaler technique.5 Poor intentional non-adherence is mostly due to concerns about (side) effects of the medication, low perceptions of the necessity of the treatment or practical problems in implementing the daily medication regimen. This causes deviation from the prescribed regimen.6–8 Actively identifying and discussing patient-level barriers for using inhaler medication (correctly) is important to reduce (un)intentional medication adherence.
To identify these barriers, adequate patient–healthcare provider communication is a prerequisite as it strengthens patients’ trust and motivation, increases knowledge and medication adherence.9 In the Netherlands, pharmacy technicians (PTs) interact with patients at medication dispense, recurring every 3 months. For this reason, they have an excellent opportunity to monitor and support patients’ in their inhaled medication use. Besides general medication use information, PTs provide inhalation instruction, currently mostly only at first dispense. Despite PTs’ potential to support patients in their medication use, research showed that providing good inhalation instructions as well as addressing topics such as adherence or psychosocial aspects of medication use during pharmacy encounters, is not yet common practice.10 11 Even when such care is provided, the effectiveness is often hindered by PTs’ inadequate knowledge of the inhaled medication and the technique required to use the inhaler device12 13 or insufficient communication skills.14
Also, the patient-centredness of communication in pharmacy counselling sessions is not yet optimal. Patients’ perceptions and preferences about medication are hardly discussed and the majority of the patients at the counter do not ask questions nor do PTs encourage them to do so.10 15–17 One the one hand, training PTs in patient-centred tailored communication specifically for inhaler medication and increasing knowledge of inhaled medication should benefit PTs’ ability to properly educate patients during counselling sessions.10 18 A previously developed online feedback training has already shown to successfully improving PTs’ patient-centred communication at the pharmacy counter.19 On the other hand, patients also need to be more involved in the counselling session with their PT, which could increase their knowledge, trust and control of their treatment.20 21 Preparing patients for their counselling sessions with healthcare providers has shown to improve the communication, patient satisfaction, empowerment, recall of information and reduces concerns.22 23 A way to prepare patients is the use of a Question Prompt List (QPL), which invites patients to select important topics they want to discuss with their healthcare provider.24
Up to now, no intervention strengthens the role of both the PT and the patient in the counselling session to improve inhaler medication adherence and inhaler technique. Most previously evaluated interventions to improve medication adherence and inhaler technique included some form of passive, one-way adherence or inhaler technique education, PT education or the provision of electronic reminders.25–28 A recent review, however, showed that interventions that address both perceptions and practicalities were more effective in improving adherence.29 Therefore, we developed an intervention that focuses on TRaining of pharmacy technicians and patient prepAration and Counselling (On TRACk). We combine an online feedback communication training for PTs specific for inhaler medication counselling, and consultation preparation by both PTs and patients to stimulate an active role in the consultation.
The On TRACk study aims to assess the effectiveness and cost-effectiveness of the On TRACk intervention in a cluster RCT. The On TRACk intervention aims to contribute to better long-term inhaler technique and to increase inhaled medication adherence among patients with asthma and/or COPD. This paper describes the protocol of this study.
Methods
Study design
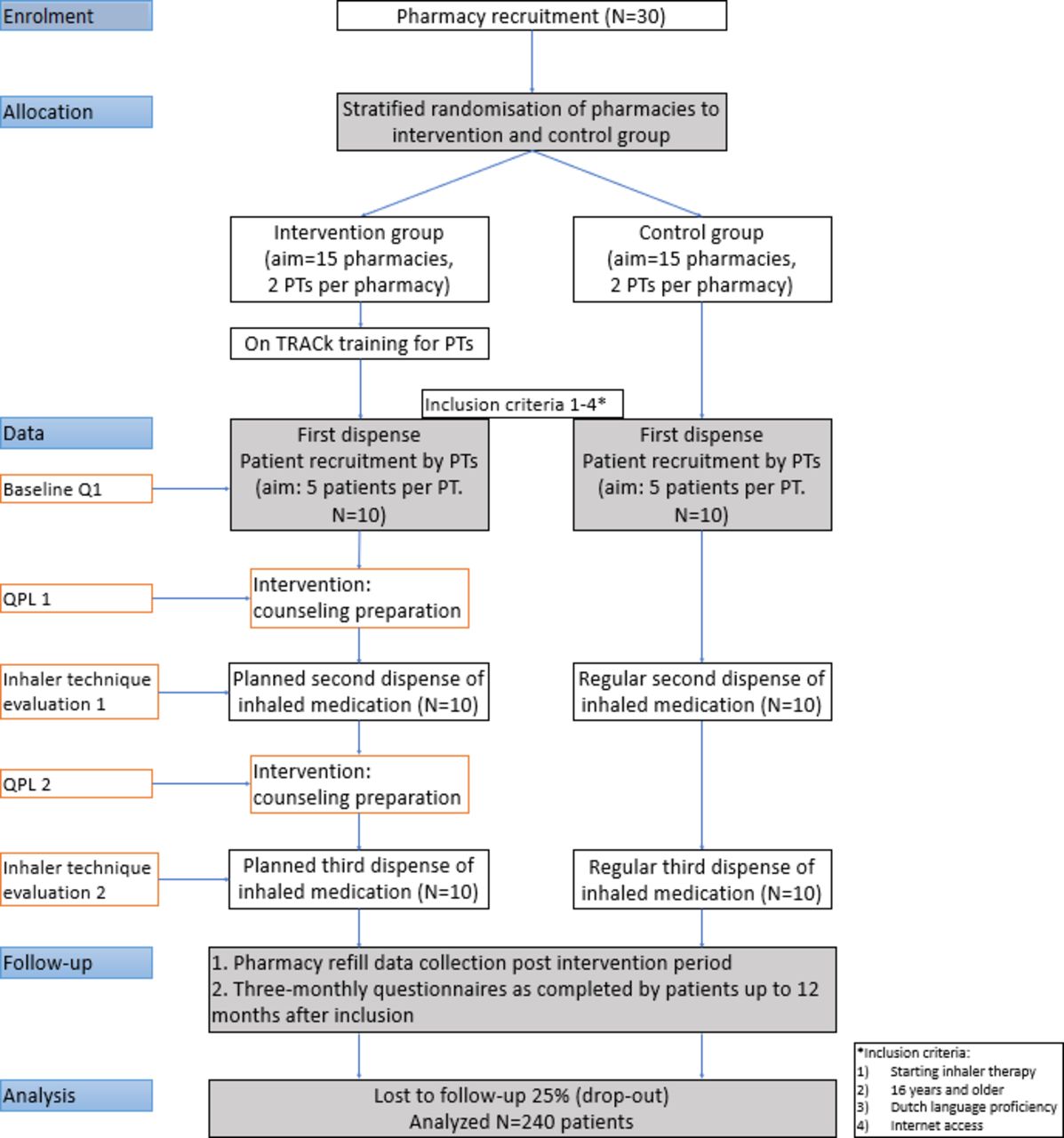
The On TRACk study is a cluster RCT with an intervention group and a control group (see figure 1). We aim to involve 15 pharmacies, 30 PTs and 150 patients in each group. Each PT recruits five patients with asthma and/or COPD. PTs in the intervention group receive the On TRACk training, which focuses on communication skills and providing an inhaler instruction. Patients in the intervention group conduct consultation preparation for the second and third dispense counselling session. Patients in the control group receive care as usual. This study protocol is reported according to the SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) checklist.30 The study is registered with the Netherlands Trial Register with trial registration number ID NL9750.

Flow chart of study design, inclusion, randomisation and follow-up of the on track intervention. PT, pharmacy technician; QPL, Question Prompt List.
Patient and public involvement
Over the course of the study, a patient panel consisting of five patients with asthma and/or COPD will be actively involved in each step of the study. Also, the Lung Alliance Netherlands (LAN) will be involved over the course of this study with a representative in the project group, since the LAN is an overarching institute in the Netherlands regarding the field of respiratory care.
Randomisation
An independent statistician will apply block randomisation to randomly assign pharmacies to the intervention and control group in a 1:1 ratio using a computer-generated algorithm. Stratification will be applied with respect to pharmacy chain, since some chains may differ in providing patient counselling, and in specific inhaler instruction. The allocation sequence will be concealed for pharmacies until their assignment. In case pharmacies drop-out during the training period, newly recruited pharmacies will be randomly assigned to one of the groups following the same randomisation procedure as described above.
Participants
Pharmacies will be recruited through email newsletters of pharmacy networks and pharmacy practice based research networks, social media channels and by presentations at national conferences. All pharmacies (either community, outpatient or independent pharmacies) in the Netherlands are eligible to participate. The pharmacy teams decide themselves which two PTs will participate. Inclusion criteria for patients are as follows: (1) starting inhaler maintenance therapy (defined as no use of any maintenance inhaled medication in the previous 12 months) with an indication for asthma and/or COPD; (2) being 16 years or older; (3) sufficient understanding of Dutch language since most materials are only available in this language and (4) access to the internet. The only exclusion criterion for patients is severe cognitive impairment, to ensure patients’ ability to complete questionnaires. Patients’ cognitive impairment will be assessed by PTs based on their judgement of patients’ cognitive presentation at the counter. Eligible patients will be invited to participate in the study by their PT prior to—or during the first dispense consultation of their inhaler medication in the pharmacy.
Intervention for PTs: On TRACk Training
PTs from the intervention group will first receive the On TRACk training: an online video-feedback training that encompasses communication training for PTs supplemented with inhaler medication counselling education, combined with consult preparation by patients. The training aims to improve PTs communication skills, as well as their skills and knowledge on how to provide a correct inhaler instruction. The On TRACk training builds on the previously developed online feedback communication training (COM-MA, in Dutch: COMmunicatieadvies op MAat voor het apotheekteam, which translates to Tailored communication advice for the pharmacy team),19 which focused on improving general patient-centred communication at the pharmacy counter. The training will be extended with elements that are specific for inhaled medication counselling, based on literature and focus groups. To meet the standards of current practice, the guidelines developed by the LAN31 32 will be used to develop the content of the training. Furthermore, focus groups with patients with asthma and COPD will be conducted to collect patient preferences and tailor the training to patients’ needs. Overall, seven main domains that were identified in the previously performed COM-MA study, were used to operationalise patient-centred communication and counselling. The On TRACk training will build on these domains and extend them with relevant aspects regarding inhaled medication management and counselling. The domains identified by COM-MA are:
Match with the information needs of the patient.
Providing essential user information and ask patients about their medication taking experience.
attention to the patient during the counselling session.
patient involvement during the counselling session.
Signalling and addressing concerns or other (negative) views of patients regarding medication.
Structure of the counselling session.
presence of preconditions like privacy or waiting time.
The online training consists of three core elements; self-reflection, feedback, direct interaction with the trainers via chat. First, for training preparation, PTs will videotape a maximum of five dispense counselling session with patients in which an inhaler instruction is provided. These videos will be send to the trainers through a secure connection. Second, the trainers select two suitable video’s per participant based on the following criteria: proper audio, clearly visible hand gestures of PTs to monitor device preparation, and no identifiable footage of the patient. If more than two videos adhere to these four criteria, we aim to select one video in which the communication scores higher and one in which it scores lower. Third, PTs will complete a self-reflection assignment for these two counselling sessions by reflecting on the seven communication domains by pointing out what aspects of the consultation went well and what elements can be improved on. Lastly, feedback will be provided on each of the domains by trainers based on the scores of the observation protocol, combined with PTs’ self-reflection, formulated as tops (what is going well) and tips (what can be improved). A chat function that contacts the trainers is at PTs disposal in case of questions.
To support the written feedback, PTs will be able to review short informative videoclips on various aspects of providing inhaler medication instruction to patients. A total of 13 clips were recorded with a PT with ample experience in providing inhalation technique training (see for a more detailed list online supplemental appendix A). While trainers can specifically point PTs to relevant clips, all clips are accessible.
Supplemental material
Intervention for patients: consultation preparation and counselling
For patients, participation in the intervention involves additional counselling by their PTs through planned second and third dispense counselling session that either takes place in the pharmacy consultation room or online, depending on the availability of a consultation room in the pharmacy. Prior to the dispense moments, patients will be asked to select a maximum of three topics they would like to discuss using the QPL: a structured list with example discussion topics designed to aid question asking behaviour and concern expression during the consultation. This ensures contemplation of patients’ personal needs and barriers and is a helpful tool to engage them in—and prepare them for—the dispense counselling session with their PT. The three topics, as chosen by the patient, will be redirected to their PT. Additional topics may be provided by patients if not suggested by the QPL.
During the planned second and third dispense counselling session, PTs will evaluate patients’ inhaler technique based on critical errors identified in the CRITIKAL study,33 and guidelines developed by the LAN.31 32 If necessary, additional inhaler technique instructions will be provided to improve patients’ inhaler technique. After the trial, patients will be invited to the pharmacy for evaluation of their inhaler technique.
On TRACk web-portal
A web-portal was developed to facilitate the On TRACk training, consultation preparation, and evaluation of inhaler technique. For the training, PTs are registered with personal accounts and gain exclusive access to their personal videotaped counselling sessions. Via this portal, PTs (A) perform self-reflection, (B) receive personal feedback, (C) have access to clips and (D) are able to contact the trainers via a chat-function. The web-portal is secured in accordance with NEN 7510, and ISO/IEC 27001.
To prevent researchers having access to individual data of patients, patients are registered to the portal by their PTs and automatically provided with a research number. Patients are provided with personal log in data to the web-portal. Here, they will find information about their medication and illness and tips and tools to support their self-management. Access logs can be accessed to evaluate patients’ utilisation of the On TRACk web-portal. After consultation, scores on patients’ inhaler technique can be entered in the database on the web-portal by their PTs. Lastly, the On TRACk web-portal invites patients to complete a total of five follow-up questionnaires every 3 months, starting right after inclusion in the trial. Reminders to complete counselling preparation or questionnaires will be send automatically as well.
Usual care group
This study aims to minimally alter usual care for control group patients, to avoid possible interference with the trial. Therefore, usual care that is provided in the control pharmacies will be mapped and evaluated, following the national guidelines for handing over inhaled medication as provided by the Royal Dutch Pharmacists Association.34 Basic guidelines for handing over medication include verification of the prescription, fitting pharmacotherapy, addressing patients’ perspective, product availability and financial handling of the product. To map usual care, participating PTs in both the intervention and control group will be asked to fill out a questionnaire covering topics regarding asthma/COPD care that will be provided to patients in daily practice. It will also cover whether PTs regularly receive training (aimed at counselling, patient communication or inhaler medication education). To compare results between intervention and control group, patients in the control group will be asked to fill out a 3-monthly questionnaire (see data collection below). After the trial, patients will be invited to the pharmacy for evaluation of their inhaler technique.
Data collection and measurements
This study will evaluate the effectiveness of the intervention both on the patient level and PT level. In addition, cost-effectiveness will be evaluated. Patients in the control group will receive the same follow-up as patients in the intervention group, except for inhaler technique assessment. Outcomes will be measured via (1) pharmacy refill data, (2) an online questionnaire including validated scales displayed on the On TRACk web-portal at inclusion (baseline), and after 3, 6, 9 and 12 months after inclusion and (3) a PT-reported questionnaire to assess inhaler technique (intervention group only). Figure 2 provides an overview of all points in time where data from patients in the intervention and control group will be collected. Table 1 provides an overview of which outcome measures are included per point in time.

{kind=link}
{kind=link}
Flow chart of data collection points in time during and after the on track intervention. QPL, Question Prompt List.
Overview of assessment of outcome measures per point in time
Outcome measures
The primary study outcome is adherence to inhalation maintenance medication. This will be measured with pharmacy refill data, calculated using the continuous multiple-interval measure of medication availability (CMA), more specifically the CMA7.35 The CMA7 takes into account carry-over from previous prescriptions (ie, oversupply is first used before a new supply). In this study, the CMA7 will be regarded as a continuous measure, as a percentage of the number of days of theoretical use of the medication, divided by the number of actual days between the start and end of our study. The theoretical days of medication use, is in this study calculated by the extraction of total number of days without available medication, by the total number of days of observation.
Medication use
Persistence with the inhaled maintenance medication (the duration of treatment) will also be measured using pharmacy refill data. The number of oral corticosteroid (OCS) courses (as indicator for poor asthma control or exacerbations) as well as the number of short-acting beta agonists (SABA) dispenses (indicator for poor asthma control) will be measured over the course of 12 months.36 37 Recent GINA guidelines stipulate ‘as-needed’ SABA or OCS use for asthma patients. Due to difficulties in measuring adherence for this group with refill data, sensitivity analyses will be performed with and without these patients in separate analyses.
Self-reported medication adherence
The Medication Adherence Report scale for Asthma (MARS-A)38 and the Test of Adherence to Inhalers (TAI)39 will be included to measure patients’ self-reported adherence. The MARS-A identifies both intentional and unintentional adherence, with 10 items on a 5-point Likert scale. The 10-item (of each five points) TAI identifies the level to which patients can be adherent, and distinguishes erratic, deliberate or unwitting non-adherence.
Attitude, self-efficacy and confidence in communication
To measure patients’ understanding and attitude towards medication, and patient–provider communication, the Beliefs about Medicine Questionnaire (BMQ)40 Self-Efficacy for Appropriate Medication use Scale (SEAMS),41 and Perceived Efficacy in Patient-Physician Interactions (PEPPI-5)42 will be included. The BMQ is a 10-item questionnaire that identifies two factors of beliefs about medication; the necessity and concerns about prescribed medication. The SEAMS is a 13-item questionnaire that addresses self-efficacy with medication among patients with a chronic disease across various levels of health literacy. The PEPPI is a 5-item tool to assess patients self-efficacy of interactions with their healthcare provider.
Inhaler technique
Patients’ inhaler technique will be assessed by their PTs during the planned counselling sessions at second and third dispense. Inhaler technique will only be evaluated in the intervention group, since patients in the control group will not have planned counselling sessions. A checklist to evaluate inhaler technique will be developed based on critical errors in inhaler technique that have a significant detrimental effect on health outcomes,33 combined with inhaler-specific observation checklists from the LAN.31
Cost-effectiveness analysis
Cost–utility will be assessed as incremental costs per quality-adjusted life-years gained determined by the EuroQol-5 Dimensions-5 Level43 and 1-year mortality. Cost-effectiveness will be assessed as costs per point improvement on the Asthma Control Questionnaire-644 or Clinical COPD Questionnaire-10.45 For both analyses, a 1-year time horizon and societal perspective will be applied. Direct costs will be calculated based on units of healthcare utilisation (general practitioner (GP) visits, emergency department visits, hospital admissions—related to their lung disease) multiplied by their standard unit prices in the Netherlands, and are assessed with a subset of the Medical Consumption Questionnaire.46 Time invested by PTs will be calculated based on interviews with PTs at the end of the intervention. Indirect costs include work or school days lost, as assessed by the Work Productivity and Activity Impairment Questionnaire, for patients with asthma.47 Various scenario and sensitivity analyses will be performed (eg, minimum and maximum effect size, payer perspective vs societal perspective and varying implementation rates).
Process evaluation
As part of the process evaluation we will monitor intervention implementation throughout the trial and gain insight into the experiences, barriers and facilitators for (not) using on TRACK through semistructured interviews with 15–20 patients and 12–15 PTs carried out by the researchers, which will be audiotaped. Patients will be interviewed regarding their experiences with the On TRACk intervention such as their planned and prepared counselling sessions. PTs will be interviewed regarding their experiences with the On TRACk training and the planned counselling sessions. To evaluate implementation factors of this intervention, the RE-AIM framework will be used.48 This framework identifies five dimensions: reach, efficacy, adoption, implementation and maintenance. The On TRACK intervention will be evaluated in terms of to what extent each dimension has been met. With reach, we will assess to what extent the intervention reaches the targeted population. The effectiveness of the intervention is assessed on patient level, as explained in the outcome measures paragraph. Adoption is defined as the amount of PTs that are carrying out the On TRACk intervention as intended. It will be assessed if and why possible drop-out occurred. With implementation, we assess the fidelity of On TRACk, which includes the extent to which the intervention is carried out as intended. The fifth and last dimension of the RE-AIM framework, maintenance, focuses on the extent to which On TRACk is, or will be, included in daily practice of the pharmacy, and which factors stimulate or impede this.
Sample size calculation
Power analysis showed that to detect a difference of 15%49 (SD=15) in adherence to inhalation maintenance medication between the intervention and control group, calculated with a power of 0.80 and an alpha of 0.05 and accounting for clustering with an intraclass correlation coefficient (ICC) of 0.10, 120 patients per group are needed. An ICC of 0.10 is considered relevant based on previous research in Dutch pharmacies identifying ICCs in the range of 0.05–0.14.50 51 Allowing a 25%52 53 drop-out rate, 150 patients will be included per group. To keep inclusion per pharmacy and workload per pharmacy feasible, with 10 patients per pharmacy over two PTs per pharmacy, 15 pharmacies per group need to be recruited. For pharmacies with larger teams, the participating in On TRACk can be higher or each PT might be able to include more patients. If this is the case, the number of participating pharmacies can then be lower, as long as the total number of patients per group will be 150.
Statistical analysis
To take clustering of patients within PTs within pharmacies into account, multilevel analyses will be performed to analyse differences in primary and secondary outcomes between the two groups. A model with random intercept will be estimated to control for repeated measurements. The data will be analysed according to the intention-to-treat principle. Furthermore, a per-protocol analysis will be conducted as sensitivity analysis. If numbers allow, subgroup analyses will be conducted for asthma and COPD patients. Sociodemographic characteristics of patients, such as age, sex, level of education, household size, status of employment, native language, will be included in the model to control for their effect. Data will be analysed with AdhereR in R, and Stata V.16.0 for Windows.
The obtained data from the post-trial interviews will be transcribed and analysed using MAXQDA software. A thematic content analysis will be performed according to Green and colleagues54 who identified a four steps approach to summarise data from qualitative sources: (1) data immersion, (2) coding, (3) creating categories and (4) identifying themes. Coding will be performed with a combination of deductive (based on the RE-AIM framework) and inductive coding. The coding will be done by two researchers, independently from each other. Differences in coding will be resolved by discussion until consensus is reached.
Discussion
The On TRACk intervention aims to tackle a complicated problem of mostly unintended incorrect inhaler technique and non-adherence to inhaler medication in patients with asthma and/or COPD. This study combines two previously proven successful interventions, online video-feedback training for PTs and consult preparation by the patient, extended to inhaled medication. Combining these interventions will better structure inhaled medication counselling sessions, increase involvement of patients in their medication intake behaviour, and improve their inhaler technique as well as their medication adherence.
The online design of the intervention contributes to easier implementation, since it provides a wider time frame in which the training can be followed or counselling preparation can performed. The portal will be easily accessible for PTs and patients at any time, at every place and with no extra costs involved. Furthermore, through matching consultation preparation and inhaler technique education with regular dispense moments as in usual care, the intervention does not require extra contact moments in the pharmacy. In the end, patients will benefit from On TRACk when problems in inhaler technique are addressed instantly, and when the consultation with the PT matches patients’ needs, concerns, (lack of) necessity and practical issues.
This study focuses on PTs to provide patients with counselling and inhaler instruction, since they are in a good position to guide patients because of their regular contact during medication dispense moments. In the Netherlands, inhaler instructions can, next to PTs, be provided by a wide range of healthcare providers, such as pulmonary nurses, GPs, general practice-based nurse specialists or pulmonologists. Coordination between healthcare providers who provide inhaler instruction is important to provide consistent information to patients. In the Netherlands, the LAN has created guidelines that strives for all healthcare providers involved with the local or regional level to work together to guide patients that start their inhaled medication treatment.32
Strengths and limitations
An important strength of this study is that it combines two successful innovative interventions, and focuses on both PT and patient education and communication. PTs receive training that boosts their skill level and knowledge of instruction of inhaled medication. Patients are motivated to actively take part in (the conversation about) their medication treatment, and receive two extra counselling sessions to bolster their inhaler technique. This two-way strategy expands this intervention’s chances to be successful.
Another strength is that a combination of multiple outcome measurements will be used in this study. Next to the primary outcome measure of adherence, this study will also provide insight into other important patient-reported outcome measures, and evaluations of patients’ inhaler technique. The combination of these measurements enables a broad evaluation of the On TRACk intervention and patients progress in disease control, inhaler technique and adherence. Moreover, this study also includes patients over a period over 12 months. Given the long time period, changes in factors such as disease control, quality of life, seasonality and other health outcomes can be evaluated accurately.
A third strength of this study is that it aims to assess cost-effectiveness, and that this intervention could be straightforwardly implemented if proven cost effective. If cost-effective, On TRACk will be included in this national guidance book and is to be seen as common practice in the community pharmacy. Therefore, this study sought to be as efficient as possible by, for example, combining consultation preparation and inhaler technique evaluation with regular medication dispenses. No extra visits to the pharmacy have to be orchestrated, which could benefit implementation. Furthermore, this study incorporates a process evaluation, in order to adapt and overcome teething problems that might occur.
One limitation is that a potential bias in the selection process of pharmacies is present. Pharmacies that eventually decide to partake in this study, are often pharmacies with either a motivated pharmacist that valued the intervention, or motivated PTs that were eager to partake in the online training. Whereas the current intervention focused on two PTs, the whole pharmacy team should be included to maximise the success of implementation of the On TRACk intervention.
A bias could be present in the inclusion process of patients. Patients with asthma and COPD might differ in terms of adherence to inhaled medication. This study does not actively select on including either asthma or COPD patients. If numbers allow, subgroup analyses will be conducted to address possible differences between patients with asthma or COPD.
A third limitation of the On TRACk intervention is that not all eligible patients will be reached due to the online nature of the intervention. Patients with less access to digital tools, or who have lower levels of digital health literacy, have difficulties in participating in this study. Limited health literacy is associated with poorer health access and outcomes.55 Lack of digital health literacy limits access to information about inhaled medication, and how to use it properly. Patients with limited (digital) health literacy, therefore, may especially benefit consultation preparation and active participation in consultation sessions with their healthcare providers. The absence of patients with low digital health literacy in both groups should be contemplated in the evaluation of the On TRACk intervention, since their absence might result in an overestimation of overall medication adherence.
Another limitation is that the control group is prone to Hawthorne effect due to intensive monitoring. Repeated measures through questionnaires may affect participants awareness of being part of a study which in turn may affect their medication adherence.
The last limitation of this research is that this intervention merely focuses on medication adherence and inhaler technique. Self-management of asthma is also affected by environmental triggers.56 External or environmental effects are not accounted for in the patient-reported outcome measures. External factors may cause unobserved effects to patients health outcomes in this study.
Ethics and dissemination
Ethical consideration
The Medical Ethics Committee of the VU Medical Centre (UMC) of Amsterdam approved the protocol (METc protocol number 2020.358). Patient anonymity is guaranteed because all data are pseudoanonymous. The researchers do not have access to information of individual patients. Only the pharmacies are able to link patient codes to individual patient information. Furthermore, all participants (both PTs and patients) will sign written informed consent.
Dissemination plan
Results will be disseminated via different communication channels. A dedicated symposium will be organised at the end of the project, for which all healthcare providers concerned with the care for lung patients (eg, pharmacy team, GPs and their practice nurses, pulmonologists and specialist lung nurses) as well as the patients themselves and other stakeholders (eg, health insurers) will be invited. Through (social) media, attention for the study and the results will be generated, for example, with news flashes or dedicated discussion groups. Results will also be shared through the professional network of the authors, relevant (inter)national scientific conferences, relevant professional journals and scientific articles in international peer-reviewed journals.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conceptualisation (main project idea): MV, LvD, AJL, JFMvB and ESK. Funding acquisition: MV and LvD. Training and data collection: RtP and MV. Writing—original draft: RtP and MV. Writing—review and editing: MV, LvD, AJL, JFMvB and ESK.
Funding This work was supported by (The Netherlands Organisation for Health Research and Development (ZonMw) grant number 80-84800-98-18089.
Disclaimer The funding source had and will have no role in the design, data collection, analysis or interpretation of this study, or in the decision to submit this manuscript for publication.
Competing interests All authors declare not to have any competing interests that are related to this study.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.