Article Text

Abstract
Objectives Survival following traumatic injury has increased, requiring ongoing patient follow-up. While longitudinal outcomes of trauma patients are reported, little is known about optimal delivery of follow-up service for this group. The aim of this scoping review was to identify and describe the structure, process and outcomes of postdischarge follow-up services for patients who sustained major trauma.
Evidence review This scoping review was conducted by searching CINAHL, MEDLINE and EMBASE databases. Articles were screened by three independent reviewers. The data of selected articles were organised in the categories of the Donabedian quality framework: structure, processes and outcomes.
Results Twenty-six articles were included after screening by title/abstract then full text against the inclusion/exclusion criteria; 92% (n=24) were from the USA.
Follow-up services were provided by designated trauma centres and delivered by a mixture of health disciplines. Delivery of follow-up was multimodal (in person/telehealth). Protocols and guidelines helped to deliver follow-up care for non-physician led services.
Ongoing health issues including missed injuries, pain and infection were identified. No standardised criteria were established to determine recipients, the timing or frequency of follow-up was identified. Patients who engaged with follow-up services were more likely to participate in other health services. Patients reported satisfaction with follow-up care.
Conclusion There are wide variations in how follow-up services for major trauma patients are provided. Further evaluation should focus on patient, family and organisational outcomes. Identifying who is most likely to benefit, when and how follow-up care is delivered are important next steps in improving outcomes.
- Organisation of health services
- ORTHOPAEDIC & TRAUMA SURGERY
- Trauma management
- TRAUMA MANAGEMENT
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The review contains a robust search strategy devised in conjunction with an experienced librarian using multiple databases to ensure a comprehensive search was undertaken.
Following a published scoping review framework, the screening process (title and abstract and full text) was performed by three reviewers using a recognised software review programme; the review team worked independently of each other during the selection process to ensure integrity in the selection of the articles. We did perform a double identification of articles to include but we did not undertake double data extraction. To compensate for this, one author checked 20% of the included articles to ensure consistency and comprehensiveness of the data extracted.
Only published articles were included, and no search of grey literate was undertaken. A preliminary review of grey literature (such as hospital websites) was undertaken prior to formalising the inclusion/exclusion criteria identified limited extractable information in relation to the S/P/O format, out-of-date information displayed and follow-up services not identified when it was known that a follow-up service existed. It was beyond the scope of this review to contact individual healthcare institutions to retrieve information; however, this has been identified as a deficit and is the focus of future work.
Introduction
Worldwide, traumatic injury kills 4.4 million people annually, which accounts for almost 8% of global mortality.1 Specialised trauma centres and well-organised emergency services (Trauma Systems) have assisted in reducing trauma-related mortality by up to 25%.2 3 This reduction has led to an increase in survivors of traumatic injury; however, this is not without consequences for both patients, families and health services. Many survivors incur temporary or permanent disabilities4 with long-lasting physical limitations having a major impact on quality of life.5 For non-fatal traumatic injury, it is estimated there are dozens of other hospitalisations, hundreds of emergency department (ED) visits and thousands of doctors’ appointments/consultations.1 It has been suggested that up to 17% of patients discharged from a trauma service have ongoing significant health issues.6
Increased survival from traumatic injury has led to a higher demand for follow-up services when patients are discharged from hospital. Further, injured patients have greater health service utilisation after hospital discharge when compared with the general hospitalised population and this health service resource use remains elevated for several years after injury.2 The ongoing health issues experienced by trauma patients have been linked to increased healthcare expenditure.7 While these findings largely refer to patients with major traumatic injuries, as defined by an Injury Severity Score (ISS)8≥129 or ISS≥15,10 11 patients with minor to moderate injuries (ISS<12 or an ISS<15) can also experience ongoing physical and psychological problems and require ongoing support mechanisms to allow them to return to their preinjury health status.12 A detailed description of the Injury Severity Score can be found in online supplemental file 1.
Supplemental material
Injured patients have the best chance of recovery if a trauma system performs well and is effectively integrated into the wider health and social care systems.13 For patients with traumatic injury, follow-up after hospital discharge is commonly performed by general practitioners (GPs) who have little experience or expertise with recovery after trauma and maybe ill-equipped to address ongoing treatment questions from patients and their families. Patients who have experienced traumatic injury report that GPs have little understanding of their needs and that this has resulted in an increased level of dissatisfaction with postdischarge care.14
While the literature contains a wealth of information in relation to the longitudinal health-related outcomes for patients with traumatic injury, there is a dearth of information relating to the immediate postdischarge recovery period. Designated trauma clinics to address the complex post discharge needs following traumatic injury is one strategy to fill this gap. In some areas of the USA, trauma clinics have been mandated15; however, this is not a universal. In Australia and New Zealand, trauma follow-up clinics have historically been managed by the specialist surgical team responsible for the major injury,16 such as neurosurgical clinics following Traumatic Brain Injuries (TBI). This diverse approach to follow-up care following traumatic injury raises many questions about services provision and models of care and how these impact outcomes for patients and their families, as well as for healthcare organisations.
The purpose of this scoping review is to identify and describe what has been reported in the literature regarding the structure, process and outcomes of postdischarge follow-up services for patients who have sustained major trauma. The following research question was formulated: how are follow-up services delivered to patients of any age with major trauma after hospital discharge described in the literature?
Methods
A scoping review approach was used as this methodology allows for a determination of the state of the current evidence and the identification of any potential gaps within the current evidence base.17 The framework by Arskey and O’Malley17 was used to guide the approach to the review and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews statement for the reporting of scoping reviews was followed when reporting this review.18
Identification of relevant studies
Search strategy
A systematic literature search was undertaken using three healthcare databases including the Cumulative Index to Nursing and Allied Health Literature (CINAHL via OVID), PubMed and Medical Literature Analysis and Retrieval System Online (MEDLINE via OVID). The search was undertaken from inception to June 2021. Forward and backward citation searching of included articles was undertaken to identify additional literature. Duplicate publications were removed prior to assessing for eligibility (see online supplemental file 2).
Study selection
Eligibility criteria
All types of published research reports were included to allow for comprehensive reporting.
Articles were eligible for inclusion where the focus was on patients of any age with major trauma; engaging with any type of service delivery of health-related care following discharge from hospital; involved any health professional and any method of service provision (ie, face to face or telehealth) and included a follow-up component focusing on improving clinical care and/or patient outcomes. Descriptors such as ‘major’, ‘severe’, ‘severely injured’, ‘polytrauma’, ‘severely injured’ and ‘Injury Severity Score’≥12 as per Australian Trauma Registry9 were used to identify articles where the focus was on patients who had sustained a major traumatic injury.
Articles were excluded if they reported military or veterans suffering from trauma; physical trauma resulting from domestic and/or sexual violence and physical trauma resulting from self-harm because these groups often require and receive specialised follow-up services due to the nature of the trauma; therefore, these services may not be applicable to the wider general trauma population. Further exclusion criteria are patients suffering from psychological trauma where there was no component of physical injury and patients attending fracture clinic for isolated limb trauma and articles where only the abstract could be obtained.
Study selection procedure
Eligible articles were identified through two phases using Rayyan.19 In phase one, the reviewers (EW, JR, APM) independently reviewed the titles and abstract of the retrieved publications and selected articles that met the inclusion criteria. In the second phase, the full texts of the remaining articles were reviewed following the same process. Disagreements about study inclusion and exclusion were discussed and resolved through consensus between all authors.
The reference lists of all selected articles were examined using forward and backward citation searching, against the inclusion/exclusion criteria using the above procedure.
Charting the data
For the selected articles, data related to the structure, process or outcomes were systematically charted into a form developed in Microsoft Excel. Data included: organisational elements (layout, resources, equipment) healthcare staff involved and type of follow-up service; delivery of care activities (physical examination, referrals, medical imaging review) and quality of care provided; and outcomes including patient and family and organisational (appointments, readmission rates). Data extraction was completed by a member of the review team (EW) and checked by with APM or JR.
Collating, summarising and reporting the results
The data of the selected articles were organised into the three categories of Donabedian quality framework (figure 1).20 The framework is described as a conceptual model and assumes that healthcare quality should be based on three components: structure (the context in which the care is delivered); process (the combination of the actions that make up the service delivery) and the outcomes (the effects of the healthcare).20 Each component of the model has a direct influence on the next.21

Donabedian model.
The Donabedian model framework has been used to assess the quality of care delivered across several areas including ED triage processes,22 palliative care for dementia patients,23 and its use is advocated by NHS Improvement24 and the Royal College of Surgeons of England.25
Studies were assessed by the review team for methodological rigour. All studies were included in the review regardless of quality. Study quality was determined using the CASP26 Quality checklists (see online supplemental file 3 and 4).
Patient and public involvement
There was no patient or public involvement.
Results
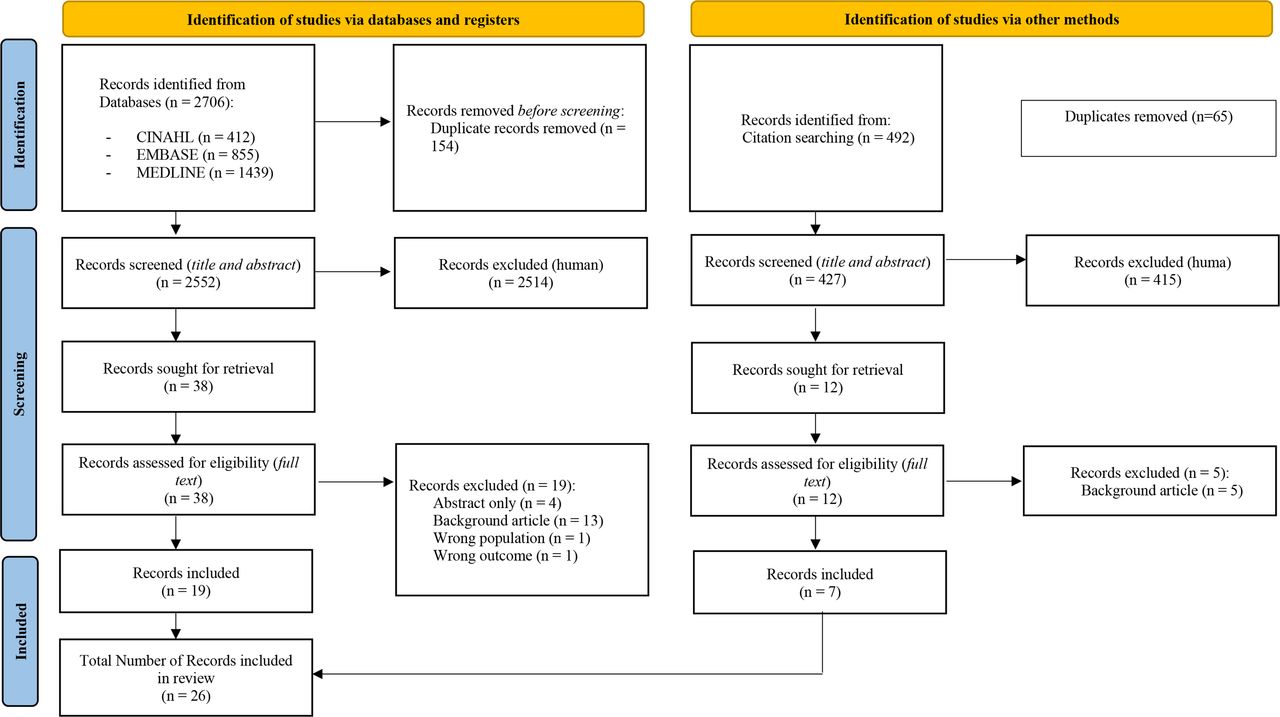
A total of 2706 articles were identified from searching the databases of which 154 were duplicates. Following the screening process 19 articles were included. From these articles, forward and backward searching of the reference lists identified an additional 427 articles. Following the same screening process, 7 articles were included (figure 2) resulting in a total of 26 articles included for analysis.
{kind=link}
{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram.
Of the 26 included articles, the majority (n=15/26) used a cross-sectional design, 7 used a cohort design, 2 were case–control, 1 used a case report method and 1 was descriptive. Overall, 92% (n=24/26) of studies were conducted in the USA and Canada, 1 was conducted in Ireland and 1 conducted in Australia and New Zealand. Quantitative data was the predominant method of data collection (n=23/26).
Three articles27–29 report separate findings from one study evaluating the ‘Trauma Resilience and Recovery Program’ (TRRP) and similarly two articles30 31 reported separate findings from one study evaluating the ‘Trauma Collaborative Care’ (TCC) programme (see online supplemental file 5).
Structure
The domain of structure refers to the context in which care is delivered20 including the physical facility, equipment and resources including staff and level of staff training (organisational). Table 1 outlines the structure elements from the included articles. Further information on the trauma centre accreditation levels can be found in online supplemental file 6.
Structure: context in which care is delivered
Physical facility
The follow-up services were provided at accredited trauma centres with the majority of the centres (n=22/23, 97%) described as level I.32
Equipment and resources
The resources required to provide follow-up included physical clinic space, phone and text messaging capability and telehealth equipment; seven articles reported using a mixture of resources.27–31 33 34
To deliver follow-up care, the resources reported included the use of a script to deliver a phone call34–36 or a scripted algorithm incorporating specific topic related questions pertaining to general well-being, pain control and complications.6 37 Protocols and guidelines were followed to deliver the care to patients38 39 although no description of the content of these were provided. In one study, a newsletter was sent to patients and families although the content and frequency of distribution was not made explicit. Seven articles report engagement with specific follow-up programmes.27–31 39 40
Only one study reported the use of equipment which was specialised to assist with the delivery of telehealth.41 This included a close-up camera with zoom capabilities for skin examinations and a digital stethoscope, both of which were reported being used 14 (64%) and 20 (91%) times respectively from 22 appointments.
Staff
Across the included studies there was diversity in the number and type of health professionals involved in delivering follow-up service with just over half (n=14/22, 64%) describing a multidisciplinary team (MDT) approach comprised of nurses, physicians and allied health professionals. Follow-up by a single healthcare professional was described by eight studies (n=8/22, 36%) of which most were delivered by allied health professionals including physiotherapists, social workers, psychologists, occupational therapists, speech and language therapists or dieticians. One study described follow-up being delivered by the trauma team but did not specify the health professionals involved.42
The experience and educational levels of staff involved in delivering follow-up was described in detail by two studies27 34 with staff described as having a ‘Masters’ level qualification34 or a bachelor’s or predoctoral.27 In both studies the advanced qualifications were specific to the psychologists involved in the team. In relation to the nursing roles, studies described educational levels in terms of the position title or experience: nurses were described as experienced35 having additional qualifications such as a nurse practitioner38 43 44 or advanced practice nurse.37
Process
The process domain relates to how the care is delivered within the context of the structure20 and focused on care delivery and quality of the interaction.
Care delivery
All but three of the included articles45–47 outlined how the process of care was delivered in relation to the follow-up, the details of which are provided in table 2. Ten studies outlined inclusion/exclusion criteria to determine their follow-up group6 29 33 37 39 40 43 48–50 this included age limitations, specific mechanisms of injury (ie, motorcycle accidents) and injury types (head, orthopaedic).
Process: how the care is delivered
The timing of the follow-up varied widely in the studies which reported this information (n=19/23, 83%). In some studies, the follow-up occurred within the first 7 days following discharge33 34 36 37 39 while for others the follow-up was 4 weeks (n=5/23, 22%) or more following hospital discharge.27 28 30 31 43 In a survey of practicing trauma surgeons from the Eastern Association for the Surgery of Trauma, 61% reported that their follow-up was scheduled for 2 weeks following discharge; others reported that there was no set timeline for follow-up or that follow-up varied depending on the injuries sustained by the patients.47
For patients who required multiple follow-up encounters, these were largely in relation to ongoing emotional or psychological support or therapy.27–31 40 43 Four studies reported multiple appointments to manage ongoing care in relation to injuries36 39 44 50 although from these, two reported that the majority of patients (between 65% and 84%) only required single visits.36 44
The patient perspective on attendance to follow-up services was reported in two studies.34 38 Both studies reported that the ongoing health needs of patients was a motivating factor in reasons to attend follow-up, especially in relation to pain and emotional support. Reasons why patients did not attend follow-up included transportation issues (47%) or that they had recovered from their injuries (55%).38
Quality of interaction
Patient assessment of the quality of the follow-up service was reported in five studies37–39 41 44; however, it was unclear who was responsible for the collection of this survey data or if the surveys used a validated tool as no studies included a copy of the survey.
Outcomes
The outcomes domain relates to the results of the healthcare delivery.20 The outcomes can be categorised into patient and family/caregiver, staff and organisational.
Patient and family
Only one study reported on clinical outcomes of the patient and the relationship with the follow-up service.49 Patients who engaged with the follow-up programme, ‘Trauma Survivors Network’ (TSN), reported a perceived increased chance of recovery and return to daily activities compared with patients who did not use the programme.
Several studies reported new, or ongoing physical or psychological health issues identified through the process of follow-up. The physical impact of trauma was identified during follow-up where the incidence of complications after discharge was reported to be up to 17%,6 mostly owing to pain6 30; although other complications included missed injuries, infection and thrombotic events. New or unexpected symptoms were also found in a quarter of all patients attending follow-up.36
Emotional recovery of patients and their family was also identified. Ridings28 reported on the initial 2 years of their follow-up intervention, TRRP, and found just over a third (33.5%) exceeded the clinical threshold for depression and/or PTSD at 30 days following injury. In the subsequent study by Ruggiero et al29 they reported a small increase on this finding to 35.9%. Similar results were reported by Hendrickson et al34 who found 30% of trauma patients engaged in follow-up wanted ongoing emotional support.
Several studies reported on the complexity of the period of time following hospital discharge where adult patients and families required clarification around appointments, discharge and injury care plans and medication instructions.34 36 37 These challenges have also been observed in the paediatric context.35 However, this finding was not consistent with up to 92% of adult patients with trauma reporting that they had booked additional appointments, obtained prescriptions and received equipment.37 Almost half of paediatric trauma patients reported no difficulties in accessing ongoing services, but this was due to established structured follow-up support based on their injuries (ie, TBI).35
The majority of patients were satisfied with the follow-up service provided with one study reporting 90% of patients surveyed found the follow-up appointment helpful.44 For patients who used telehealth to access follow-up care, 100% stated they thought this delivery method made it easier to access care.41
Staff
Improved staff performance and confidence in making appropriate referrals for trauma patients was reported in three studies.30 40 45 This confidence was linked to the training provided to staff that accompanied the implementation of the follow-up programmes such as the TSN or TCC. One study reported results of a staff survey in highlighting the barriers of implementing the programme such as financial support and lack of engagement by hospital administrations.45 In studies that did not use ‘formal’ follow-up programmes there was no provision of information relating to staff outcomes.
Organisational
Seven studies focused predominately on patient attendance rates to follow-up services15 34 38 43 48 50 51 with attendance rates ranging from 31% to 88% overall. When follow-up attendance was reviewed in terms of delivery method, face to face rated higher in compliance (31%–88%) compared with phone (33%–66.9%). Factors such as appointments not being booked, or inadequate documentation were reported to impact attendance.36 51
Four studies reported on the characteristics of the patients who attended follow-up compared with those who did not,34 38 43 50 characteristics such as insurance status, smoking status and distance to the trauma centre from the patient’s residential address were reported to be indicators of non-attendance.50 However, these characteristics were not consistent findings across all studies.34 43 Two studies report a trend towards patients with moderate to severe injuries being more likely to comply with follow-up.33 38 DeMario et al33 found that patients who attended follow-up engaged more consistently with other healthcare activities such as planned admissions or other outpatient encounters.
In terms of representations to the ED or readmissions to hospital, Dalton et al42 found that attending the follow-up clinic was not a significant predictor of ED use. One study who reported on two follow-up clinics as part of the same health organisation, found a reduction in both the presentations (from 6.4% to 5.1%) and readmission rates (from 7.1% to 6.5%).44
The economic impact of follow-up following traumatic injury has not been well described; only two studies included economic evaluations. O’Reilly et al39 provided a crude economic assessment of delivering follow-up where a comparison was made between the phone telehealth clinic to traditional face-to-face clinic. A reduction from €348 816 (face to face) to €75 175 (telehealth) was stated. DeMario et al33 reviewed aggregated charges for patients who attended follow-up and reported that patient engagement in follow-up increased costs for the health organisation statistically significantly more than patients who did not engage, although ED representation costs were lower in this group.
Discussion
In this scoping review, how follow-up services are delivered to patients with major trauma after hospital discharge were explored. A wide variety of follow-up services were identified, ranging from delivering ‘routine’ follow-up care (maintaining contact and/or re-examination of patients following hospital treatment)52 to purpose designed programmes, such as the TSN, to support patients and their families through the long-term recovery process. Many of the follow-up services were delivered by trauma specialists, with several incorporating an MDT approach. When sought, patients reported satisfaction with both the follow-up services provided and the delivery methods used.49
The review highlights a gap within the literature on how and why follow-up services are established for patients who have experienced traumatic injury. Detail on the systematic approach of developing and establishing a follow-up service was lacking; the exception being the purpose designed programmes such as the TSN or TCC.30 49 Development of any service within healthcare should be patient centric, consider equity of access, support efficient use of resources, be based on the best available evidence and provide safe, quality care.53 Several countries have published nationally accredited evidence-based trauma standards32 54–57 to provide guidance to institutions on the standard of care required to provide high quality care to trauma patients. Only the standards from Australia and Germany55 57 include recommendations on the provision of trauma follow-up service for patients. Despite this guidance, no literature published from these countries could be identified for this review.
From the review of this literature, it is unclear the extent to which trauma follow-up services are available worldwide. How these follow-up services are delivered is also highly variable and may focus on physical recovery, psychological recovery or both. The way in which follow-up services were delivered also varies in terms of how, when and to whom the services were delivered,47 such that patients and families who are affected by trauma are not always guaranteed to be able to access follow-up by a trauma specialist after hospital discharge. The impact of this inconsistent service delivery approach on patient outcomes is currently unknown.
Evaluating trauma follow-up is essential to determine the efficacy, effectiveness and impact on both organisational and importantly patient/family outcomes.53 The inconsistent approach to follow-up makes it difficult to compare the outcomes of the services. Some studies attempted summative evaluations to identify patients who were more likely to attend follow-up by reviewing variables such as discharge dispositions and hospital length of stay15 38 51; however, the results were not consistent and focused on organisational rather than patient outcomes.
Despite the lack of a formal evaluation, the literature identified that patients who participated in follow-up, report satisfaction with the services provided and importantly, found that the act of participation positively influenced their own perception of their recovery.49 Patient participation in a trauma follow-up service can facilitate understanding about individual injuries and recovery trajectories.58 Using a collaborative approach between the healthcare providers and patient to promote patient participation, forms a central component in the purpose designed follow-up programmes (TSN, TRRP).31
The afore-mentioned programmes also included the trauma patient’s family members as part of the trauma recovery journey. Engaging with families has been found to improve trauma patient outcomes.58 Family members are frequently the informal caregiver to the patient and report feeling overwhelmed and anxious during the recovery journey.35 Targeted follow-up programmes which focus on improving engagement with trauma patients and their families may improve follow-up attendance and provide a platform to provide ongoing support and care that trauma patients require.
All trauma follow-up services described in the studies included in this scoping review were conducted pre COVID-19 and it is likely that the delivery methods have been modified as a result of public health regulations or local health service priorities. Since the start of pandemic many health systems have eliminated in person routine follow-up visits where possible with video-based telehealth or telephone-based delivery for routine follow-up where possible.59 Before the COVID-19 pandemic, telehealth was established as a safe and effective method of providing follow-up following minor to moderate trauma; however, this approach may not be adequate for complex patients with major traumatic injury.59 Furthermore, patients from low socioeconomic backgrounds and/or rural and remote areas may not have the technology required to access these services thus preventing them from engaging with this platform of care delivery.60 It is currently unknown what effect, if any COVID-19 may have had on trauma follow-up services.
Although the search strategy was robustly developed it did not include grey literature. The inclusion of grey literature was initially considered but owing to limited description and outdated information we made the decision not to proceed with the inclusion of grey literature.
While the presence of trauma follow-up services is encouraging, the provision of principles to guide the delivery of follow-up services requires further work. While accreditation standards provided by professional organisations (RACS) in delivering trauma care contain reference to ongoing follow-up care, the principles in how to achieve this is lacking. Future work should focus on the development of trauma follow-up care guidance in partnership with trauma patients and their families; and incorporate frameworks to ensure follow-services can be robustly evaluated in terms of patient and organisational outcomes.
Conclusion
An examination of the literature in relation to the follow-up care provide to major trauma patients post discharge has highlighted a wide variation in relation to the services provided dependent on geographical location.
The current literature lacks robust evaluation in relation to follow-up care and trauma patient and family outcomes. While a more systematic and high-quality evaluation of trauma is required to determine the influence on outcomes, attention should also be directed at patient selection, the frequency and timing of follow-up care delivered, and the components of care provided. In addition, the paucity of economic analysis data adds to the question of whether follow-up care is of value both patients and to healthcare organisations.
These elements require further examination to assist trauma patients and their families and health authorities to assess the need and benefits of follow-up.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We express gratitude to Sarah Thorning (research and training librarian) for search strategy support and was responsible for the acquisition of data.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @lizrahilly1
Contributors EW was responsible for the conception and design of the study. EW, APM and JR were responsible for the acquisition of data. EW, APM and JR were responsible for the interpretation of the data. EW (guarantor) was responsible for the drafting of the manuscript and all authors contributed to the revision of the manuscript and approval of the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.