Article Text

Abstract
Introduction Alcohol-related cues trigger relapse in patients with alcohol use disorders (AUDs). These cues may automatically activate motivational approach tendencies. Through computerised cognitive bias modification (CBM), the tendencies of patients with AUD to approach alcohol can be reduced. The present protocol describes a training intervention with approach bias modification (ApBM) incorporating religion-related stimuli as an alternative to alcohol to improve the effectiveness of CBM in a religion-based rehabilitation centre. AUD is often related to patients’ religious attitudes in this treatment context. The religion-adapted ApBM, therefore, combines training in avoidance of alcohol-related motivational cues and an approach to religion-based motivational cues. This combination’s effectiveness will be compared with a standard ApBM and to a sham ApBM.
Methods and analysis Using a double-blind multiarm parallel randomised controlled trial procedure (ratio 1:1:1), 120 patients with AUD will be randomised into 1 of 3 conditions (religion-adapted ApBM, standard ApBM or sham ApBM) with personalised stimuli. The interventions are delivered over 4 consecutive days during an inpatient detoxification programme in addition to treatment as usual. Assessments occur before the start of the training and after the fourth training session, with follow-up assessments after 1 and 4 months. A multivariate analysis of variance will be used with the primary outcomes, the percentage of days abstinent and meaning in life 4-month follow-up. Secondary outcomes include differences in reported training satisfaction and symptoms of AUD.
Ethics and dissemination This study has been reviewed and approved by the Medical Research Ethics Committee Academic Medical Center Amsterdam (Reference number: 2020_251). Further, study results will be published in peer-reviewed journals and presented at international conferences.
Trial registration number NL75499.018.20.
- Substance misuse
- Impulse control disorders
- Clinical trials
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This randomised controlled trial examines the potential for therapeutic interventions in alcohol use disorder early on by including patients during detoxification.
With the extended follow-up of 4 months, the study design allows for the examination of the unprecedented long-term effects of approach bias modification by implicit bias change.
This study has several implicit measures in addition to questionnaires, which are less constrained to more accurate introspectively available information measuring the severity of the addiction.
Although primary and secondary outcomes will be administered by phone in follow-up in case participants cannot be directly contacted, additional variables can only be assessed at the research location.
Participants will be recruited from a Christian Mental Health Clinic, which limits generalisability due to the predominantly Christian patients.
Introduction
Worldwide, three million deaths per year can be traced to the harmful use of alcohol,1 leading to economic costs of US$223.5 billion in the USA2 and €2.6 billion in the Netherlands,3 where this study takes place. These alcohol use disorders (AUDs) costs represent one of the most significant avoidable risk factors for global burden worldwide.4 5 Current treatment practices for AUD are moderately effective, at least in the short term. One year after treatment, patients’ alcohol use has decreased by 87%,6 but despite intentions to refrain from use, patients struggle to do so, with relapse rates around 50%.7 However, compared with untreated AUD, the effects of treated AUD are small, suggesting that patients’ characteristics need to be involved in recovery instead of treatment components alone.8 Religiosity may provide a promising patient characteristic to address in recovery in addition to a specific treatment component.9 10
Possible relations between religion and recovery
Previous research has indicated that religion can be essential in AUD and recovery.11 12 However, the underlying mechanisms remain unclear. One study found that the benefits of religion on AUD were not mediated by social support or mental health.13 In contrast, other potential mechanisms show more promise. First, self-control is a potential mediator of the religion–AUD relationship. Most religions encourage the exercise of self-control to stop selfish impulses.14 Self-control as a mediator in the relationship between religiousness and alcohol use has been demonstrated in different cultures.15 Second, meaning in life may function as a mediator because religion provides a framework for purposeful activities, reducing activities’ time and incentivising salience related to AUD. AUD involves investing time and effort to obtain, use and recover. Such an alcohol-focused life prevents the pursuit of activities for long-term personal goals. Religion facilitates non-alcohol-focused activities and inhibits alcohol-focused activities. For instance, prayer as a religious activity inhibits alcohol-focused activities, supporting the recovery of AUD.16 Research shows that the relationship between religion and reduced alcohol use is mediated by meaning in life, operationalised as purpose in life.17–19 Third, self-forgiveness is a potential mediator in the relationship of religion–AUD. In general, self-forgiveness is associated with the recovery of AUD.20 However, religion emphasises a moral framework, which conflicts with uncontrolled and alcohol-focused behaviour of AUD, leading to religious struggles such as feeling abandoned by a supernatural agent (God/higher power) or having interpersonal conflicts in a religious context as a mediator for alcohol use.21–23 Evidence suggests that religion relates to reduced alcohol consumption if religious struggles are solved and individuals with AUD experience (self-)forgiveness.18 24 These aspects are confirmed by 1 study following 364 patients with AUD, indicating that growth in religiosity, more purpose in life, and more self-forgiveness with less religious struggles predicted reductions in alcohol use.25
Over the past decades, different religious recovery programmes in treating patients with AUD have included aims to increase self-control, meaning in life and self-forgiveness by focusing on surrender concerning a supernatural agent.26 27 Surrender to God has been defined as a distinctive religious coping strategy in which individuals have an internal motivation to act in obedience, increasing acceptance of one’s limitations and recognition of God’s presence.28 Although the process of surrender in religious programmes is frequently discussed and reported by patients with AUD,29–31 less is known about the working mechanism. Most studies with individuals are related to the inverse relationship with anxiety32 and worry,33 suggesting that surrender to God can be an effective coping mechanism in times of crisis. Regarding self-control, patients report by ‘letting go’, as part of surrender, a paradoxical feeling of increased control over the situation.34 Likewise, there is some evidence that surrender to God increases meaning in life by reporting more purpose, satisfaction and understanding of life.35 Further, as an aspect of self-forgiveness, the feeling of forgiveness by God due to surrender seems to be a protective factor regarding suicide.36
An intervention with religious cues to change alcohol approach tendencies
Uncontrolled alcohol use entails automatically activated mental processes.37 In fact, as a consequence of learning experiences regarding the reinforcing effects of alcohol, alcohol cues automatically activate an appetitive motivation response that includes approach tendencies.38 Given that treatment has only modest effects on relapse6 8 and little effects on implicit alcohol-related cognitions,39 cognitive bias modification (CBM) has been developed to address these automatically activated cognitive and motivational processes directly. As a form of CBM, alcohol approach bias modification (ApBM) aims to change the automatically activated tendency to approach alcohol.40 Previous research has shown that relapse rates decrease by around 10% 1 year after treatment discharge when at least four ApBM training sessions of 15 min are added to regular treatment.41–43 Likewise, another study demonstrated lower relapse rates regarding ApBM during detoxification of patients with AUD,44 a finding recently replicated.45 ApBM is expected to change the dominant behavioural tendency to approach alcohol cues by repeatedly pairing alcohol cues with an alternative category. In alcohol ApBM, the alternative category to which patients are typically trained concerns non-alcohol-containing drinks.41–43 46 However, recent research has indicated that including personally relevant behaviours may be promising,47 48 especially in other addictions where there is no obvious alternative to the addictive substance (ie, what is not smoking?). Religion can provide a framework of personally relevant and alternative behaviour. In this study, we compare the efficacy of training toward religion-related alternative cues with standard ApBM, in which patients are trained toward non-alcohol-containing drinks. The religion-adapted ApBM uses religion as a framework for goals conflicting with alcohol use, which is not limited by treatment context but experienced as urgent for the patient in the broader real-life context.
As a result of its flexibility, the ApBM can be adapted to train cues related to surrender to God as automatic religious approach motivation in addition to training of an automatic avoidance of alcohol cues. It could improve the training effectiveness in the context of religion-based treatment. Pictures related to surrender presented during religion-adapted ApBM can support religious-relevant alternative behaviour. For example, during cue activation (eg, experiencing stress) by pairing the alcohol-related cue with personal-relevant consequences (religious behaviour is helpful), which can be transferred in a real-life context (during daily religious rituals). Research suggests that the personal value of cues influences the automatic appetitive response related to self-control,49 which includes cues related to religious attitudes and behaviour,50 providing the basis for the religion-adapted ApBM. In theory, in the context of a religious rehabilitation programme, activating automatic appetitive processes related to surrendering to God could increase responsiveness to religious activities and thus indirectly be associated with meaning in life. Consequently, this could decrease the activation of automatic appetitive processes related to AUD.
Religion-adapted ApBM as an experimental add-on in treatment
This protocol tests this hypothesis in an experimental add-on intervention to change automatic approach tendencies to alcohol and influence automatic mental processes related to surrender to God in AUD patients in a religious treatment setting. The main goal of this randomised controlled trial (RCT) is to test the efficacy of a religion-adapted ApBM training compared with standard ApBM and sham ApBM training. The primary outcome percentage of days abstinent at 4-month follow-up is expected to be higher in both training interventions compared with the sham ApBM with religion-adapted ApBM having the most considerable effect size in this comparison. The same group differences are expected for the second primary outcome because meaning in life is improved by stopping AUD behaviour. Further, the religion-adapted ApBM could also facilitate more personally meaningful religious activities. Secondary outcome variables are training satisfaction and symptoms of AUD. We expect that the religion-adapted ApBM will lead to more training satisfaction after the last training session and fewer AUD symptoms 4 months later than the other interventions. An additional explorative analysis will explore the usefulness of different measures—that is, self-control, meaning in life, self-forgiveness and actual bias change—for selecting the training intervention in which patients could benefit more.
Methods
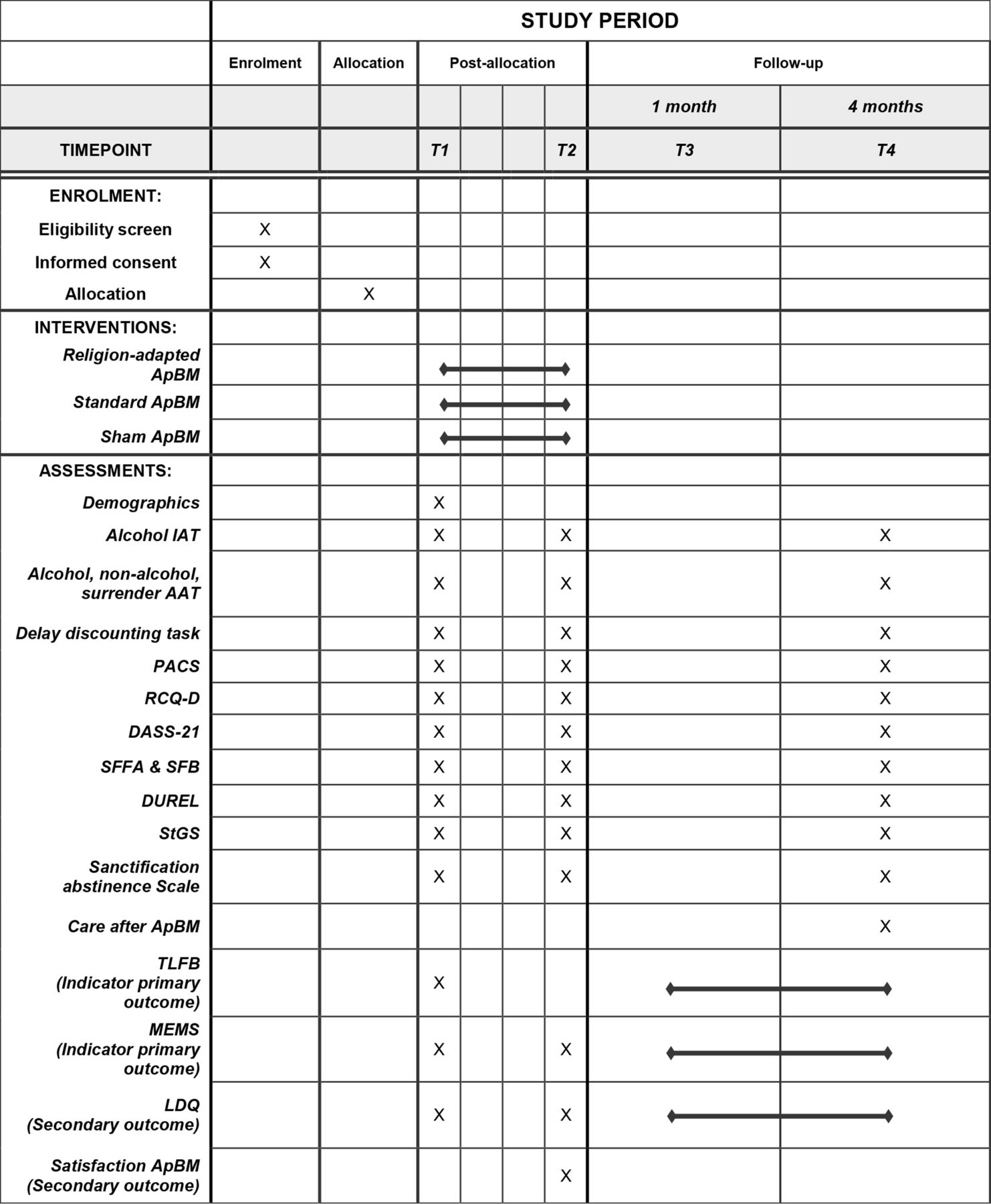
The present study is a double-blind, multiarm parallel, superiority RCT with three conditions, each consisting of four sessions of either religion-adapted, standard or sham training (ratio 1:1:1) in addition to treatment as usual (TAU) (figure 1). Patients complete a baseline assessment (T1), four sessions of training, a post-training assessment (T2), and two follow-ups during their stay in the detoxification clinic. One month later (T3), patients are contacted by phone during the first follow-up. Four months after the post-training assessment, the second follow-up (T4) will be done at the clinic with a more extensive assessment.

Participant flowchart. ApBM, approach bias modification; TAU, treatment as usual.
Participants and procedure
The study will run between 1 September 2021 and 1 May 2024 in a Christian mental healthcare clinic and addiction centre in the Netherlands. The clinic works disorder specific, primarily according to cognitive–behavioural therapy for AUD and schema therapy, if needed, with a comorbid personality disorder. In addition, pharmacotherapy and trauma therapy is provided if necessary. In all treatments, special attention to the patient’s faith experience is given. Patients from all religious and philosophical backgrounds can participate. However, it is expected, due to the treatment context, that most patients in this study describe themselves as Christians. The targeted number of 120 participants will consist of patients between 18 and 70 years with a diagnosis of AUD following the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders. Patients with severe neurological disorders (such as Korsakoff syndrome), acute psychotic symptoms, visual or hand-motoric handicaps or difficulties with the Dutch language are excluded.
During the second day of the detoxification programme, the patients receive a folder with study information, informed consent and contact information regarding the current study. On day 3, patients are free to participate in the baseline assessment (T1) after at least 24 hours for consideration. The baseline assessment is followed by a daily training session (figure 2). After the fourth session on day 7, patients run through the post-training assessment (T2). One month later, the first follow-up (T3) by phone will be enrolled, followed by a more extensive follow-up in the fourth month (T4) at the clinic. This follow-up gives results of at least 30 days without clinical care because some patients will have 3 months of a clinical programme after detoxification as TAU. Patients can withdraw from the study at any time without consequences for their treatment plan. If patients leave the detoxification programme earlier for unexpected reasons, they will still be approached for follow-up measures unless they indicate a desire to withdraw from the study. By default, already collected data will still be used for analytical purposes but not if patients explicitly reverse the permission to keep the data. This information about the data collection is provided before the start of the study.

{kind=link}
{kind=link}
Standard Protocol Items: Recommendations for Interventional Trials diagram. Time schedule of measurements and interventions. Care after ApBM: Did you have clinical care after detoxification? (Yes/no). AAT, approach–avoidance task; ApBM, approach bias modification; RCQ-D, Readiness to Change Questionnaire—Dutch version; DASS-21, Depression Anxiety Stress Scales 21; DUREL, Duke University Religion Index; IAT, Implicit Association Test; LDQ, Leeds Dependence Questionnaire; MEMS, Multidimensional Existential Meaning Scale; PACS, Penn Alcohol Craving Scale; SFFA & SFB, State Self-forgiveness Scale; StGS, Surrender to God Scale; TLFB, Timeline Followback.
Patient and public involvement
Before planning the RCT, 10 patients in the Christian mental healthcare clinic were approached through a semistructured interview to find out whether surrender to God also plays a role within the target group of the study (see online supplemental file 1). Most (n=9) described surrender to God as joy, happiness, finding identity, self-worth, peace and disgust towards sin (such as alcohol addiction), and one patient described surrender to God as struggling. In addition, all patients indicated that, according to them, without surrender to God, the consequences could lead to relapse, loneliness and death. Because of this reported importance, a religion-adapted ApBM, focusing on surrender to God, is selected for this RCT. Apart from this, patients were not involved in the planning of the RCT.
Supplemental material
Religion-adapted ApBM and standard ApBM
Patients select personally relevant religious pictures on the computer screen about surrender and pictures about alcohol and non-alcohol beverages that will be used to assess approach bias and training with ApBM. No action by the research staff is necessary to select pictures because they are automatically integrated into the instruments. In all three ApBM interventions, the training protocol of Wiers et al43 is used with the instruction to react by pulling or pushing the joystick depending on a right-tilt picture format or left-tilt picture format (indirect instructions). A zoom-effect supports the experience of pushing or pulling the picture (zoom-in on pulling, zoom-out on pushing). The scaling of the picture corresponds with the joystick until the maximal movement is performed. Each ApBM training session starts with a brief assessment block presenting all picture categories (surrender, alcoholic and non-alcoholic beverages, presented an equal number of times), equally often in a right-tilt format or left-tilt format. In the next block, stimuli are presented in the to-be-pulled or pushed format depending on the experimental condition: In the religion-adapted ApBM, alcoholic beverages are avoided/pushed and surrender pictures are approached/pulled; in the standard ApBM, alcoholic beverages are avoided/pushed, and non-alcoholic beverages are approached/pulled, and in the ApBM sham-control condition, all categories are pulled and pushed equally often (continued assessment, no training effects expected42 43). In other words, the difference between the religion-adapted ApBM and the standard ApBM is not in the avoided category (alcoholic beverages) but the to-be-approached category: religious pictures of surrender in the religion-adapted ApBM and non-alcoholic beverages in the standard ApBM.
Measures
Demographics
At baseline, patients’ age, gender, education level, employment status, relationship status, religious background, housing, age of onset of use, psychiatric diagnoses, medication and use of other substances are assessed. Further, the history of neurological disorders, acute psychotic symptoms and visual or hand-motoric handicaps are checked by medical staff and documented in the electronic health record. Finally, during the last follow-up assessment, patients responded whether there was clinical instead of ambulatory treatment after the ApBM training (yes or no) to check for the actual implementation of the treatment plan.
Self-report measurements
Primary outcomes
At baseline and follow-up of one and 4 month(s), the Timeline Followback (TLFB) is assessed to estimate the percentage of days abstinent51 52 for the first primary outcome. The research assistant collects TLFB data with a 30-day retrospective calendar-based measure of daily alcohol use. The research assistant will calculate the standard drinks and ask patients to use their calendars to respond. The percentage of days abstinent is a frequent outcome in AUD research.6 8 The experience of meaning in life (second primary outcome) is measured with the Multidimensional Existential Meaning Scale.53
Secondary outcomes
Additionally, the symptoms of AUD are measured with the Leeds Dependence Questionnaire.54 Furthermore, patients also report training satisfaction (second secondary outcome) on a 9-point Likert scale ranging from ‘strongly agree’ to ‘strongly disagree’.
Additional self-report variables
Other self-report measures examine craving with the Penn Alcohol Craving Scale,55 56 negative emotional states with the Depression Anxiety Stress Scales 21,57 58 motivation with the Readiness to Change Questionnaire59 and self-forgiveness with the State Self-forgiveness Scale.60 Religiosity is examined due to intrinsic religiosity with the Duke University Religion Index61 62 and the Surrender to God Scale.28 Abstinence as a sanctified religious goal is assessed with the sanctification scale.63 During post assessment, patients also report training satisfaction on a 9-point Likert scale ranging from ‘strongly agree’ to ‘strongly disagree’.
Behavioural (implicit) measurements
Automatically activated alcohol associations will be assessed with the Implicit Association Test (IAT)43 64 65 using words related to alcoholic beverages (such as beer, wine, etc) and non-alcoholic beverages (such as coke, water, etc) for the target categories. Further, words related to approach (such as advance, closer, etc) or avoid (such as away, escape, etc) will be used for the attribute categories. The automatically activated religious and alcohol approach tendencies are measured by a modified approach–avoidance task (AAT)66 with self-selected pictures related to surrender and alcoholic and non-alcoholic beverages. Using the IAT and AAT at baseline, post-training assessment and follow-up, the effectiveness of the training interventions can be checked by an actual change in alcohol and religious approach association.38 Also, the relative preference for short-term over long-term rewards is assessed by the five-trial delay discounting task.67 It examines a possible explanation of the effectiveness of the religion-adapted ApBM in terms of self-control related to stronger delayed gratification capacity,68 69 which has been associated with a reduction in alcohol use.70
Statistics for primary and secondary outcomes
Following the intention to treat method, a multivariate analysis of variance will be used with primary outcomes with all randomised patients regardless of completing all the assessment and training sessions. The percentage of days abstinent and meaning in life at 4-month follow-up will serve as dependent variables to measure recovery. Transformed scores will be used to normalise the data to meet the statistical test’s assumption. The secondary outcomes will be used in a second analysis.
The feasibility of a sample size of 120 patients completing the study is estimated with data from 2018 and 2019 about the inflow of 207 unique patients with AUD at the four detoxification departments. In the estimation, it is assumed that 85% of the patients are willing to participate in the study during 33 months of data collection containing a 32% chance of non-response at the 4-month follow-up (207 (inflow)–31 (15% not participate)–56 (32% no follow-up)=120). An analysis with G*Power V.3.1.571 leads to the conclusion that sufficient power (0.8) is met with 2 primary outcome variables, the estimated sample size of 120 participants, alpha of 0.05 and estimated small effect size (f²=0.05) in such interventions.42
Exploratory analyses
Additionally, in a moderator analysis, multiple regression with the primary and secondary outcomes tests the different additional variables concerning bias change, self-control, religious growth (difference in religious measures between baseline and 4-month follow-up), purpose and (self-)forgiveness for exploratory purposes examining relevant patient characteristics related to training effectiveness. Finally, the associations of these variables concerning the percentage of days abstinent regardless of the intervention will be analysed to confirm previous results in the literature.
Randomisation
Before the data collection, a computer-based, random number generator72 is used for blocked random assignment by a researcher who is not involved in the study’s data collection. For stratification of gender and clinical programme after detoxification (yes/no), four randomisation schemes will be formed. Although the estimation exists of approaching 207 patients with AUD, randomisation will define 4 schemes with 255 unique numbers (3 numbers per set in 85 sets) as a precaution to consider that more patients can be approached during the actual data collection. The four randomisation schemes will be used to randomly select patients in the three experimental interventions (religion-adapted ApBM, standard ApBM and sham ApBM).
According to the generated number 255, folders for the four randomisation schemes for all expected patients are programmed on the computer in the laboratory, including the corresponding training intervention by a different researcher who is not involved in generating the random allocation sequence and data collection. To ensure the blinding procedure, the research staff only fill out the information for stratification. Then the programmed randomisation procedure independently starts the appropriate condition for the patient. Allocation concealment will be ensured until finishing data collection, which takes place 4 months after the last training session of the last patient who will participate. The folders on the computer look the same to ensure that research assistants who are only involved in data collection do not know the specific training intervention of a patient. Clinical staff will be informed about the study’s general process but receive no information about the training intervention of the patient.
Ethics and dissemination
Ethical approval has been granted through the Medical Research Ethics Committee Academic Medical Center Amsterdam (Reference number: 2020_251). All participants provide written consent to participate after receiving a full written and verbal explanation of the study’s aims, procedures and risks. It is registered in Netherlands Trial Register (reference number: NL9014) and Central Committee on Research Involving Human Subjects (reference number: NL75499.018.20). The aim is to publish the findings in peer-reviewed international journals. In addition, therapists, physicians and other care providers working with AUD will be informed through national and international conference meetings.
This protocol describes a double-blind, RCT comparing the effectiveness of a standard ApBM with sham ApBM and a religion-adapted ApBM with self-selected valued stimuli related to surrender to God during detoxification in the context of a religious rehabilitation programme. Residential detoxification is associated with costly investments of time and medical staff providing medical interventions but is often limited concerning psychological interventions aimed at recovery. ApBM could be a convenient way for patients with AUD in this early recovery stage to participate in psychological interventions increasing treatment effectiveness. Although data collection with patients with AUD will be implemented according to the protocol, unexpected changes (eg, patients’ length of stay, day-to-day well-being) during the detoxification programme are not always avoidable, leading to non-completion. In some cases, two ApBM sessions will be done in 1 day (morning and afternoon) to prevent non-completion. The ApBM programme will record the individual training sessions’ date and time to control how many patients receive more than once a day.
Furthermore, the 1-month follow-up can contribute to maintaining patient compliance for the 4-month follow-up. However, because the assessment procedure is the same in all conditions, we expect that possible positive effects of the reminder can still be attributed to the specific condition and not the assessment procedure. Besides, suppose patients cannot come in person for the 4-month follow-up, despite travel allowance, due to unexpected reasons. In that case, the primary and secondary outcomes will be assessed by phone. In addition, some patients may experience craving or distress because of the use of alcohol pictures in the ApBM. Therefore, before and after the ApBM craving will be monitored to minimise the consequences by providing information on a cognitive–behavioural coping technique if patients experience intense cravings.
Personalised approaches seem more effective in assessing automatic mental processes.73 74 However, to our knowledge, the effect of self-selected meaningful stimuli contrasting alcohol stimuli during ApBM has not yet been studied. If the religion-adapted ApBM affects recovery by personal relevance, it will align with the effort to use personalised stimuli in CBM.47 48 Different self-selected meaningful stimuli depending on the patient’s characteristics could be effective for recovery. For example, individuals with AUD who have parenting goals could improve recovery by using pictures of their child during ApBM to increase their approach motivation to parenthood and paring it with avoidance movement to alcohol.
To the best of our knowledge, this will be the first RCT to integrate religious aspects in CBM to improve the treatment of patients with AUD. Even though religious approaches in treatment can be helpful,75 76 it is unclear how a patient with AUD in the context of a religious rehabilitation programme can benefit from religious interventions. The present protocol provides a design to integrate a promising intervention in treatment for AUD adding data on explanations of how religion can be helpful during recovery. The interest in religion and spirituality in mental health is growing, but few studies are conducted on religious traditions in relatively secular countries. Although the generalizability of the data will be limited to a Christian sample, the results can reveal a personalised treatment approach that can be helpful for individuals of other religious minorities. Particularly in religious minorities, the unintentional hesitation by health professionals to discuss religious needs during treatment77 may contribute to less treatment commitment and satisfaction, which personalised religion-adapted ApBM could address.
As CBM has only small effects on the targeted automatic processes,42 more data on possible workings mechanisms for selecting the most efficient CBM are necessary. The religion-adapted ApBM that will be used consists of a low-effort method to support the potential religious coping of patients with AUD. If supported by the data, integrating religious coping in treatment could offer benefits for recovery78 and moderate craving in patients during detoxification.22 This proposal measures the growth of surrender to God as religious coping, exploring another possible working mechanism between the relation of religion and alcohol use. Next to automatic mental processes related to alcohol and religion and religious coping, the study also assesses the potential role of several variables, including changes in delayed gratification, intrinsic religiosity, meaning in life, negative emotions, motivation and craving, thereby providing information that may enrich future studies with novel recovery-related theoretical models.
Ethics statements
Patient consent for publication
Acknowledgments
We are very grateful to Dr Wubbo Scholte for the opportunity to plan the study at an early stage. We also wish to thank Dr Raoul Grasman for his statistical advice and Dr Cis Vrijmoeth for his comments on the first draft. We would like to extent our gratitude to the staff of De Hoop ggz, Dordrecht, for their enormous patience and assistance—especially Irene Blom, Jan Jaap de Jonge, Jan-Kees Obbink, Rick Millarson and Bram Schep—and to the researchers Christel Hartkoorn, Jeanette van Schaik, Simone Heemskerk, Inge van Ast and Heiltje van de Minkelis-Brak for their efforts in managing this protocol.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors H-JS conceived of the study. H-JS, HS-J, BO and RWW initiated the study design. HS-J, BO and RWW provided (statistical) expertise in clinical trial design. JCL programmed the Approach Bias Modification intervention. H-JS drafted the manuscript. All authors contributed to the refinement of the study protocol and approved the final manuscript.
Funding This project is funded by Stichting tot Steun Vereniging tot Christelijke Verzorging van Geestes- en Zenuwzieken project grant 282. Stichting tot Steun Vereniging tot Christelijke Verzorging van Geestes- en Zenuwzieken played no role in the preparation of the protocol reported herein or this manuscript.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.