Article Text

Abstract
Introduction Acute variceal haemorrhage (AVH) in patients with cirrhosis remains a topic of great interest. Although several guidelines recommend endoscopy within 24 hours after AVH, there is no consensus on the most appropriate time to perform this intervention. The purpose of this study is to identify whether urgent endoscopy (within 6 hours after gastroenterological consultation) is superior to non-urgent endoscopy (between 6 hours and 24 hours after gastroenterological consultation) in reducing the rebleeding rate of these patients.
Methods and analysis This is a single-centred, prospective, randomised clinical trial. Between March 2021 and December 2023, an estimated 400 patients will be randomised in a 1:1 ratio to receive endoscopic intervention either within 6 hours or between 6 and 24 hours after gastroenterological consultation. Randomisation will be conducted by permuted block randomisation, with stratification by age, systolic blood pressure and pulse rate. The primary efficacy endpoint is rebleeding within 42 days after control of AVH. The secondary efficacy endpoints mainly include all-cause mortality within 42 days after randomisation, persistent bleeding, length of hospitalisation, etc.
Ethics and dissemination The study protocol was approved by the Ethical Committees of Jinling Hospital (authorised ethics no. DZQH-KYLL-21-01). This trial will provide valuable insights into the timing of endoscopic intervention for AVH in patients with cirrhosis. Furthermore, the trial results and conclusions could provide high-quality evidence to guide clinical research and treatment.
Trial registration number NCT04786743.
- Endoscopy
- Hepatobiliary disease
- Hepatology
- Oesophageal disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This prospective trial will strictly group patients following the randomisation principle of the study protocol; it will reduce the effect of confounding factors and selection bias, which means that the conclusion is authentic and believable.
Due to the high efficiency of the emergency green channel, the interval before gastroenterological consultation will be controlled within 10 min after admission to the emergency department, which could greatly increase the possibility of patient survival.
In this randomised controlled trial (RCT), we attempt to further validate the efficacy of predicting the prognosis of patients with cirrhosis with acute variceal haemorrhage by the scores mentioned in the manuscript. The results will provide an important reference for clinical treatment.
One limitation is that it will be implemented at a single centre only, so the evidence may be lower than that of a multicentre RCT.
Another limitation is that we will exclude patients with haemodynamic instability occurring before or after the initial fluid resuscitation. Therefore, the conclusion may not be generalisable for patients with the aforementioned status who undergo emergency treatment.
Introduction
In China, chronic liver disease (CLD) is a primary cause of morbidity and mortality. Its aetiologies mainly include chronic hepatitis B or C virus infection, alcoholism and autoimmune liver disease. Approximately 400 million people suffer from CLD, and 25% of them are carriers of hepatitis B surface antigen.1 2 Cirrhosis is the end stage of CLD. Acute oesophagogastric variceal haemorrhage, also abbreviated as ‘acute variceal haemorrhage’ (AVH), is a primary and severe complication of cirrhosis. For patients with AVH undergoing standard therapy (band ligation, vasoactive drugs and antibiotics), mortality during AVH could be as high as 16%.3 With the development of minimally invasive techniques, early endoscopic intervention has been increasingly considered as the first-line treatment for patients with AVH.4 5
Several guidelines recommend endoscopy within 24 hours after AVH,6–8 but there is no consensus on the most appropriate time to perform endoscopic intervention during this period. Two observational studies9 10 and one systematic review11 reported no difference in mortality between patients subjected to endoscopy within 12 hours and after 12 hours. Nevertheless, one study showed that performing endoscopy more than 12 hours after admission could significantly decrease mortality and rebleeding.12 Furthermore, some reliable studies demonstrated that performing endoscopy more than 12 hours after admission could significantly increase rebleeding and mortality rates in patients with AVH13–15; one recent meta-analysis also concluded that endoscopy within 12 hours might improve the survival of patients with AVH, but it seemed to have no obvious efficacy on rebleeding.16 However, few relevant studies have explored the differences in efficacy between urgent endoscopy (<6 hours after gastroenterological consultation) and non-urgent endoscopy (6–24 hours after gastroenterological consultation) for patients with cirrhosis with AVH.
Recently, a prospective randomised controlled trial (RCT) conducted by a team from the Chinese University of Hong Kong showed that for patients with acute upper gastrointestinal haemorrhage (AUGIH) and a Glasgow-Blatchford score (GBS) of 12 or higher, there was no significant difference in mortality or further bleeding between the groups on <6-hour urgent endoscopy and non-urgent endoscopy 6–24 hours after gastroenterological consultation.17 For patients with AUGIH, a GBS of 12 or higher is indicative of a higher risk of further bleeding or mortality.17 Although this study included a range of aetiologies, including peptic ulcers, gastro-oesophageal varicosity, malignant upper gastrointestinal tumours and other diseases that could cause AUGIH, only 9.7% (25 cases) and 7.4% (19 cases) of patients included in the group <6 hours and the group 6–24 hours, respectively, were patients with cirrhosis with AVH. Therefore, the results are not generalisable enough to describe the effectiveness of endoscopy within 24 hours for these patients after gastroenterological consultation.
Based on the studies mentioned above, we made the bold assumption that patients with cirrhosis with AVH undergoing non-urgent endoscopy (6–24 hours) would have higher rebleeding rates than those undergoing urgent endoscopy (<6 hours) after gastroenterological consultation. The purpose of this study was to conduct an RCT to further define the role of urgent endoscopy and non-urgent endoscopy in patients with cirrhosis with AVH.
We present the following article in accordance with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) reporting checklist (online supplemental material 1).
Supplemental material
Methods and analysis
Study design
This investigator-initiated study is designed as a single-centred, randomised clinical superiority trial with two parallel groups and a primary efficacy endpoint of rebleeding within 42 days after control of AVH. The study protocol will strictly adhere to the 2013 SPIRIT guidelines.18 19 We intend to compare the effectiveness of improving the rebleeding rates of patients with cirrhosis with AVH between the urgent endoscopy and non-urgent endoscopy groups. The Department of Gastroenterology and Hepatology, Affiliated Jinling Hospital, Medical School of Nanjing University will take full responsibility for this trial, including recruitment of patients, endoscopic intervention, admission education, in-hospital nursing and subsequent follow-up work. This trial has been registered at ClinicalTrials.gov (ID: NCT04786743).
Data processing
Two investigators in our department are responsible for the data collection and storage. One investigator will inspect the data collected by the other investigator. After completing the inspection, the data, which are open to the analysts, will be kept in secret and input into the offline database constructed by the investigators. As soon as they complete all the data storage, the two investigators will conduct a double inspection. The collected data will be used for data analysis. The investigators will strictly follow the study protocol to inspect, collect, record and preserve the data in a timely manner to minimise the occurrence of missing data. If missing data occur in a small percentage of patients, we will handle it with multiple imputation. We will perform source data verification by comparing them with authentic medical records to assess the accuracy, completeness and representativeness of registry data.
Patient enrolment
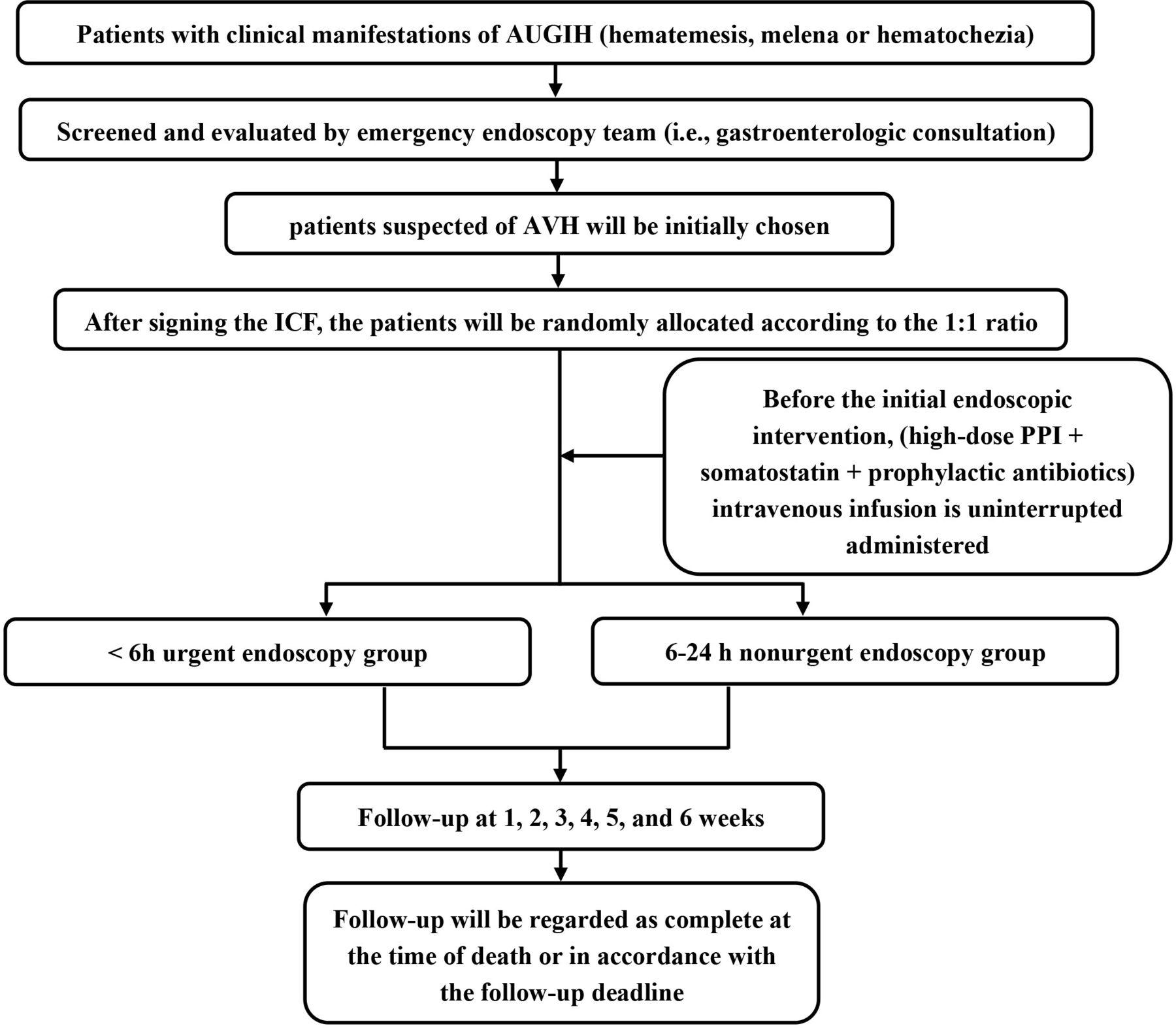
An estimated 400 patients will be consecutively included in the study between March 2021 and December 2023. Patients or their statutory agents must provide written informed consent before participating in any of the study procedures. The model for end-stage liver disease (MELD) score,20 Child-Pugh score, cirrhosis acute gastrointestinal bleeding (CAGIB) score21 and original GBS, instead of the modified version,22 will be used to evaluate the condition of each patient. The flow chart and the experimental record of this trial are shown in table 1 and figure 1, respectively. Although the informed consent form and case report form in this article are provided in English, they will be provided to the patients in Chinese during the trial.
{kind=link}
Flow chart of the trial protocol. AUGIH, acute upper gastrointestinal haemorrhage; AVH, acute variceal haemorrhage; ICF, informed consent form; PPI, proton pump inhibitor.
The scheme for patient enrolment, assessment and follow-up in the trial
Inclusion criteria
Patients eligible for the trial must comply with all the following criteria at randomisation: (1) patients who have pathological or clinical and imaging evidence indicating a diagnosis of cirrhosis; (2) patients with clinical symptoms associated with AVH (haematemesis, melaena or haematochezia) before admission or during hospitalisation; and (3) patients who are haemodynamically stable before or after initial fluid resuscitation.
Exclusion criteria
The exclusion criteria are as follows: (1) pregnancy; (2) lactation; (3) age under 18 years; and (4) patients with a history of taking anticoagulant or antiplatelet drugs within 2 weeks.
Sample size
According to a study by Ardevol et al,23 among 646 patients with cirrhosis with AVH who underwent endoscopy within 6 hours after admission, the 45-day rebleeding rate was 26%, which was similar to that in another study by Chen et al,14 who reported that the overall 6-week rebleeding rate was 25.7%. Regarding the experience at our centre, it is difficult for emergency endoscopy team members to identify the bleeding site of the AVH by endoscopy for some patients who are assigned to the group 6–24 hours; we attribute this to the efficacy of the combination of proton pump inhibitors (PPIs) and somatostatin. If the bleeding site is undetectable, the endoscopic haemostatic procedure cannot be completed. Although conservative treatment could contribute to temporary control of AVH, the risk of rebleeding could greatly increase over the following days; additionally, patients assigned to the group 6–24 hours would have a higher volume of fluid infused, which could contribute to the rebleeding and restoration of portal venous pressure. Thus, we speculated that the rebleeding rate of the group 6–24 hours might be statistically significantly higher than that of the group 6 hours. To the best of our knowledge, there are no high-quality, large-sample RCT data on endoscopic treatment for AVH within 6–24 hours and within 6 hours after gastroenterological consultation. Considering the resource limitations of a single centre, we assumed a clinically significant difference of 14% to implement this exploratory trial and provide support for further confirmatory trials. Next, we calculated that having at least 189 patients in each group would reveal differences (26% vs 40%), with a statistical power of 80% and a two-sided α level of 5%. Considering withdrawal and loss to follow-up, the sample size was increased to 200 patients per group.
Randomisation and time set
Eligible patients will be randomly assigned in a 1:1 ratio to receive endoscopic intervention either within 6 hours or between 6 and 24 hours after gastroenterological consultation. Randomisation will be conducted by permuted block randomisation stratified by age (≥60 years or <60 years), systolic blood pressure (SBP) (≥90 mm Hg or <90 mm Hg) and pulse rate (≥100 beats/min or <100 beats/min). The purpose of using stratified randomisation is to reduce the imbalance of covariates because they are strongly correlated with the outcome indicators between groups, and to further control bias. The block size is prespecified, but physicians and investigators will not be notified of this fact during the study. The randomisation sequence generation and allocation concealment will be implemented by the mobile client randomisation tool ‘Randomization Allocation Tool’. There are two primary sources of patients. Most of these patients are from the emergency department, and the others are patients with cirrhosis who developed AVH during hospitalisation. For patients from the emergency department, the interval between admission and receiving gastroenterological consultation will be controlled within 10 min by applying the emergency green channel in our centre. However, for patients who develop AVH during hospitalisation, the time will be recorded according to when they are evaluated by the emergency endoscopy team (ie, gastroenterological consultation). To facilitate data recording, the time will be uniformly calculated for all patients according to when the gastroenterological consultation is received. The patients will be randomly allocated to undergo urgent endoscopy within 6 hours or non-urgent endoscopy between 6 hours and 24 hours after gastroenterological consultation. The following time data will be recorded: (1) time from presenting with symptoms of AVH to admission (patients from the emergency department); (2) time from admission to gastroenterological consultation (patients from the emergency department); (3) time from presentation to gastroenterological consultation (patients who develop AVH during hospitalisation) and (4) time from gastroenterological consultation to endoscopic intervention (all of the patients).
Blinding
The outcome assessors will be blinded to the randomisation allocation and will not participate in the practical treatment and intervention; in particular, two scientific researchers specialising in gastroenterology with more than 3 years of clinical rotation experience will serve as the outcome assessors. Professional academic statisticians blinded to the group allocation will conduct all the analyses. However, the endoscopists will not participate in the outcome assessment. Furthermore, they will not need to disclose details of their interventional procedures to the outcome assessors.
Control of AVH, persistent bleeding and rebleeding
AVH under endoscopy mainly refers to blood gushing or seeping from oesophageal or gastric varices; however, if there is no blood gush or seepage detected, thrombus stigmata attached to varices together with massive haematocele of the stomach will also be regarded as one kind of AVH under endoscopy. Control of AVH refers to a lack of persistent bleeding signs within 24 hours after the initial endoscopic intervention; otherwise, the patients will be regarded as having persistent bleeding, which is defined as the occurrence of at least one of the following items: (1) vomiting of fresh blood or suction of more than 100 mL of fresh blood from the nasogastric tube; (2) occurrence of haemorrhagic shock and (3) decrease in haemoglobin level of 30 g/L in the absence of a blood transfusion. Rebleeding refers to recurrent bleeding after the control of AVH, which is defined as the occurrence of at least one of the following items: (1) haematemesis, melaena or haematochezia; (2) decrease in SBP of more than 20 mm Hg from the original level or an increase in heart rate of 20 beats/min; and (3) decrease in haemoglobin level of 30 g/L in the absence of a blood transfusion. Patients with persistent bleeding or rebleeding will immediately undergo a secondary endoscopic intervention or be transferred for other salvage treatment (surgery, percutaneous transhepatic variceal embolisation or transjugular intrahepatic portosystemic stent shunt (TIPSS)) according to their condition and wishes. Although the vast majority of acute haemorrhage and rebleeding is caused by oesophagogastric varices in this trial, acute haemorrhage and rebleeding caused by non-variceal factors will also be recorded and included in the statistical analysis.
Treatment
Before endoscopic intervention: all patients will receive uninterrupted intravenous administration of high-dose PPIs (8 mg/hour) and somatostatin (250 µg/hour) and antibiotic prophylaxis.
Initial endoscopic intervention: patients who have non-variceal bleeding under endoscopy will not be excluded from this trial; as patients are screened strictly according to the inclusion and exclusion criteria, there will theoretically not be many of these patients. Moreover, professional academic statisticians will conduct intent-to-treat analysis and per-protocol analysis, which are described in detail in the following statistical analysis. For patients meeting the criteria for AVH, numerous methods could be applied, including histoacryl injection, sclerotherapy, variceal ligation, a covered stent or combinations of these. The patient’s position will be chosen to expose the best field of view under endoscopy, and an external cannula for endoscopy could be used to prevent asphyxiation. Furthermore, initial endoscopic intervention will be aimed solely at the bleeding site. After endoscopic intervention, we will transfer the patient to the general ward or intensive care unit (ICU) according to the patient’s condition.
After the initial endoscopic intervention, all the patients will be treated with continuous high-dose PPIs (8 mg/hour) and intravenous infusion of somatostatin (250 µg/hour) for 72 hours, together with the preventive administration of antibiotics for no more than 120 hours; during the follow-up, oral propranolol and ultrasound-guided histoacryl injection could be used as secondary preventive measures according to the patient’s condition.
The emergency endoscopy team consists of three experienced endoscopists, each with more than 10 years of experience in endoscopy and over 500 cases of variceal haemostasis experience under endoscopy. Furthermore, several seasoned endoscopic nurses who are proficient in applying endoscopic treatment instruments and cooperating with endoscopists will also be included.
Endpoint setting
The primary efficacy endpoint refers to rebleeding within 42 days after the control of AVH. The secondary efficacy endpoints mainly include: (1) all-cause mortality within 42 days after randomisation; (2) persistent bleeding; (3) length of hospitalisation; (4) transfer to the ICU; (5) secondary endoscopic intervention because of rebleeding or persistent bleeding; (6) blood transfusion therapy; (7) in-hospital costs during the first admission; (8) any adverse events that occur between randomisation and the end of follow-up; (9) transfer to undergo TIPSS; (10) transfer to undergo surgery; (11) concurrent infection; (12) the patient’s position during endoscopy; (13) application of an external cannula for endoscopy; and (14) secondary prophylaxis such as endoscopic intervention, TIPSS and surgery.
Follow-up time
After randomisation, follow-up work will begin. All the patients included will be followed up for no less than 42 days after controlling for AVH. When the patients' conditions are stable, further treatment of varices will be determined according to their wishes and statutory agents. Patients with good compliance will be administered standard endoscopic secondary prophylaxis after 5 days of AVH control, and the follow-up time should be once a week. Patients who decline to accept further endoscopic intervention will undergo only weekly follow-up. Follow-up could be in the form of a telephone or outpatient review. Follow-up will be regarded as complete at the time of death or in accordance with the follow-up deadline.
Adverse events
Any adverse events, defined as any functional or organic lesion caused by the trial, fever, chest pain, dysphagia, perforation of the oesophagus or pulmonary embolism, will be documented. If any adverse event occurs, the physicians will treat the patients immediately, and the study protocol will be changed or terminated according to their wishes. The emergency endoscopy team member on duty will instantly inform the primary investigator and ethics committee of the severe adverse events to decide whether the patient should be withdrawn from the trial and unblinded.
Statistical analysis
Primary analyses for the primary efficacy endpoint between the urgent endoscopy and non-urgent endoscopy groups will be performed in the intention-to-treat population, which will include all patients who are randomised to a study therapy group, regardless of whether they receive the endoscopic intervention. Multiple imputations with the Markov chain Monte Carlo method will be applied to impute the missing endpoints. Secondary analyses will be based on the per-protocol population, which will include all patients who receive the intended endoscopic intervention without a major protocol violation or loss to follow-up.
Descriptive statistics will be used to compare patients randomised to the urgent endoscopy and non-urgent endoscopy groups with respect to baseline variables. Continuous variables will be expressed as the means and SDs (normally distributed) or medians and IQRs (non-normally distributed). Assessments of normality for continuous variables will be performed using the Shapiro-Wilk test. Categorical variables will be calculated as frequencies and percentages.
For the primary analyses, the rebleeding rates within 42 days will be compared between the two groups using the Χ2 tests and the Cochran-Mantel-Haenszel tests, and their differences and corresponding 95% CIs will be calculated. Additionally, the rebleeding rates will be estimated using the Kaplan-Meier method. The log-rank test will be used to compare the difference in rebleeding rates between the two groups. A Cox proportional hazards regression model will be used to estimate the HR and its 95% CI. The proportional hazards assumption will be assessed using the Schoenfeld residual test. Furthermore, the Cox regression model will be performed to assess the consistency of the endoscopy regarding the primary efficacy endpoint, taking the randomisation stratification factor into consideration. Except for age, SBP and pulse rate, the subgroup analysis also included sex, CAGIB score, the severity of liver disease, etc. For these subgroup analyses, HRs and 95% CIs for the primary efficacy endpoint will be calculated for each subgroup, and subgroup differences will be assessed based on the test for the interaction of the treatment group by subgroup in the model. Additionally, the Cox regression model will also be performed as a sensitivity analysis to assess the effect of endoscopy on the primary efficacy endpoint while accounting for a priori clinically important baseline characteristics (eg, age, sex, CAGIB score, Child-Pugh score, MELD score, etc). Two-tailed p values will be used, and a p value of <0.05 will be indicative of statistical significance.
The secondary efficacy endpoints will be assessed in the per-protocol population and compared between the two groups with Χ2 test for differences in proportions and with Student’s t-test and Wilcoxon’s rank-sum test for normally distributed and non-normally distributed data, respectively. The results for secondary efficacy endpoints will also be presented with 95% CIs. As they will not be adjusted for multiplicity, findings for the analysis of secondary efficacy endpoints should be interpreted as exploratory. All analyses will be performed using SAS software (V.9.4; SAS Institute).
Interim analysis and monitoring
No interim analysis is planned.
Patient and public involvement
Patients or the public will not be involved in the design, conduct, reporting or dissemination plans of our research.
Ethics and dissemination
We intend to publish the results of the TEACH trial in a major journal.
Discussion
This trial will proceed strictly based on the Consolidated Standards of Reporting Trials.24
Although the performance of endoscopic intervention for patients with cirrhosis within 24 hours after AVH has achieved international recognition and research on the timing of endoscopic intervention for AVH has progressed, there is still much controversy regarding the efficacy of earlier endoscopic intervention (<6 hours or 12 hours after gastroenterological consultation). Several studies have reported the 6-week rebleeding and mortality rates for patients with cirrhosis with AVH after endoscopy within 12 hours after admission. For instance, Huh et al12 reported a 34.4% rate of 6-week composite endpoints (a combination of mortality and rebleeding rates) for patients with cirrhosis with AVH who underwent endoscopic intervention within 12 hours after admission, and Chen et al14 and Yoo et al9 reported high 6-week rebleeding rates (18.9%) and mortality rates (ranging from 22.5% to 27%), respectively. In a more recent systematic review with meta-analysis, Bai et al reported that performing endoscopy within 12 hours might have no obvious efficacy on the prevention of rebleeding.16 After performing endoscopy within 6 hours after admission, Ardevol et al23 found that the 6-week rebleeding rate was 26%. Furthermore, there have been no definitive prospective data on the impact of non-urgent endoscopy (between 6 and 24 hours after admission or gastroenterological consultation) on mortality and rebleeding rates of these patients. The efficacy of non-urgent endoscopy has long been controversial. To our knowledge, there are no high-quality, large-sample prospective studies that provide authentic data to verify whether endoscopic intervention is better as early as possible, or whether urgent endoscopy is truly beneficial to patients with cirrhosis with AVH (eg, reducing the rebleeding and mortality rates, reducing the length and cost of hospitalisation, etc), so we designed this RCT after carefully assessing the advantages and disadvantages of previous related studies. By strictly implementing our randomisation scheme, the patients can be evenly assigned to the two groups, which makes it possible to draw accurate, credible results and conclusions. The strict randomisation principle, which was not enforced in previous retrospective studies, can greatly improve the reliability of the article conclusions.
In China, many patients with cirrhosis present with AVH every year. Therefore, it is necessary to investigate the efficacy of urgent endoscopy (<6 hours after gastroenterological consultation) and non-urgent endoscopy (between 6 and 24 hours after gastroenterological consultation) with prospective, large-sample data. This trial is intended to provide a relatively idealised random environment that could assist us in observing differences in the efficacy between urgent endoscopy and non-urgent endoscopy in patients with cirrhosis with AVH.
As described above, randomisation will be conducted by permuted block randomisation stratified by age, SBP and pulse rate. The three indices used to stratify are also easier to obtain and grouping is less time-consuming. Moreover, we regard the randomisation only as a preliminary grouping basis. If the patient is assigned to the group on non-urgent endoscopy 6–24 hours by randomisation and has severe liver disease, persistent haematemesis, melaena or haematochezia and a deteriorated condition, then we will immediately perform endoscopic intervention regardless of the randomisation. As we are including only haemodynamically stable patients, only a very small number of them are expected to experience sudden deterioration of their condition. Some patients and their statutory agents will be confused about the grouping when the RCT is implemented. Hence, it is very important to have effective communication and establish trust between the doctors and patients, Patients will never be forced to comply with the procedures, and everything is based on their wishes and that of their statutory agents.
Theoretically, the best option is to perform emergency endoscopy first; then, after the patient is diagnosed with AVH under endoscopy, the patient will be randomly assigned, which could prevent the interference of other AUGIH-related diseases, such as peptic ulcers and gastrointestinal carcinoma. However, it is clearly unethical to do so in practical clinical work. As the assignment of patients will be randomised, the probability of error is equal in the two groups; accordingly, assigning patients before endoscopy according to our protocol could also avert confounding by other AUGIH-related diseases.
The Baveno VI Consensus Workshop recommended that 6-week mortality should be the primary efficacy endpoint for AVH studies.25 However, according to data from our centre, very few patients died within 6 weeks after controlling for AVH; in some cases, a proportion of patients are readmitted for rebleeding, and rebleeding is indeed an important indicator of prognosis in patients with cirrhosis with AVH. Therefore, after considering the actual situation at our centre, we chose rebleeding within 42 days after achieving AVH control as the primary efficacy endpoint for this RCT. Nevertheless, we will continue to focus on mortality and regard it as one of the secondary efficacy endpoints.
While endoscopic intervention is central to the research in this trial, some other interventions we attempt to perform during this trial may affect the outcome. First, it has been proven that timely application of antibiotics for gram-negative bacteria could positively improve overall survival, prevent early rebleeding and reduce the risk of bacterial infection, so short-term antibiotic application is recommended for all patients with cirrhosis with AVH, regardless of the presence of confirmed infection.8 26 Therefore, we chose to use prophylactic antibiotics for all the included patients in our trial. Second, it was reported that in a review of 15 studies, salvage TIPSS could achieve control of AVH in 90%–100% of patients and result in rebleeding in 6%–16%.8 27 In this trial, patients with persistent bleeding or rebleeding that could not be controlled by endoscopic intervention could be transferred to undergo salvage TIPSS. Clearly, salvage TIPSS could greatly benefit these patients. We will follow up with these patients carefully, evaluate the efficacy of TIPSS in our centre and provide a better treatment choice for them. Third, there is substantial evidence showing that the application of non-selective beta-blockers (NSBBs) increases the mortality rate of Child-Pugh grade C patients.28 In our trial, we did not exclude patients with Child-Pugh grade C. Consequently, considering clinical safety, we did not plan to use NSBBs as the essential treatment for patients with Child-Pugh grade C included in this trial. Furthermore, NSBBs have been reported to increase the risk of portal vein thrombosis in patients with cirrhosis with esophagogastric varices29–31; at the same time, out-of-hospital application of NSBBs poses a great risk for patients with poor compliance; thus, we do not choose to routinely apply NSBBs. However, if the patients need a combination of NSBBs for secondary prophylaxis, we will administer NSBBs to them.
Overall, it is certain that the results of this trial could provide reliable evidence for the management of patients with cirrhosis with AVH; moreover, through subgroup analysis, more meaningful conclusions will be drawn to guide future treatment and improve the quality of life and prognosis of the patients. At present, COVID-19 is rampant worldwide, and urgent endoscopy in our centre has also been greatly affected by the virus. Nevertheless, we will try our best to do epidemic prevention and continue our RCT to advance the treatment of patients with cirrhosis with AVH.
Trial status
Protocol trial version: 1.2; date: 4 May 2022.
Recruitment start date: April 2021.
Recruitment estimated end date: February 2024.
Recruiting.
Registry
The project is registered at the ClinicalTrials.gov database (https://clinicaltrials.gov/ct2/show/record/NCT04786743).
Dissemination policy
All the authors are committed and agree to publish the full results of the research regardless of the final results.
Data monitoring committee
The data monitoring committee comprises three clinical doctors, who are not involved in our study. The committee will meet at least once a year, monitor data and provide appropriate documentation.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors ZY contributed to the design, draft and revision of the manuscript. JX, FY, YQ, MY, HX, MJ, SS, ML, HS, KJ and HT contributed to the design of the manuscript. YL and FW contributed greatly to the design and revision of the manuscript. ZY, JX, and FY contributed equally to this work. All authors read and approved the final protocol.
Funding The trial is supported by the National Natural Science Foundation of China (Nos. 81873559 and 82170574), Youth Fund of National Natural Science Foundation of China (82100621), and Youth funding projects of Jiangsu Provincial Natural Science Foundation (BK20210147). All authors are very appreciative of the financial support.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.