Article Text

Abstract
Introduction Chronic lower extremity angiopathy is a peripheral vascular disease that can result in disability and death. The tibial transverse transport (TTT) technique has been used to treat this disease in recent years. TTT’s effect remains unclear owing to the lack of large samples and high-quality evidence. Therefore, this study aims to assess TTT’s effectiveness and safety in chronic lower extremity angiopathy treatment.
Methods and analysis Relevant studies were acquired by searching the following databases: Cochrane Library, Embase, PubMed, Web of Science, China National Knowledge Infrastructure (CNKI), China Science Technology Journal Database (VIP), Wanfang Data and Chinese Biomedical Literature Service System (CBM) until 20 September 2021. All randomised controlled trials and cohort studies on TTT for chronic lower extremity angiopathy will be included in this review. The primary outcomes will include the healing time and healing rate. The additional outcomes will include the Ankle Brachial Index, amputation rate, ankle skin temperature, Visual Analogue Scale, hospitalisation time, vascular endothelial growth factor, effective rate and complications. We will use Stata V.16.0 software and Review Manager V.5.3 software for meta-analysis. Subgroup and sensitivity analyses will be conducted, if necessary.
Ethics and dissemination This study was based on previous data. The medical ethics committee of Inner Mongolia People’s Hospital, located in China waived the need for formal approval of this research, as this study did not fall under the principles of the Declaration of Helsinki. The results will be disseminated through peer-reviewed journals or relevant conferences.
PROSPERO registration number CRD42021281124.
- diabetic foot
- wound management
- foot & ankle
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Our reviewers will independently implement the steps regarding study selection, data extraction, study quality assessment, data analyses, heterogeneity analyses, subgroup analyses and sensitivity analyses.
All cohort studies and randomised controlled trials will be included to provide adequate statistical power.
A study limitation was that we only searched articles reported in English or Chinese.
Subgroup analyses will be implemented to identify underlying heterogeneity causes if there is considerable heterogeneity and sufficient data.
Introduction
Chronic lower extremity angiopathy is caused by arterial stenosis or lower extremity occlusion, including diabetic foot, arteriosclerosis obliterans and thromboangiitis obliterans.1 2 These diseases have common pathological changes, such as distal tissue hypoxia, degeneration and necrosis.3 The clinical manifestations of these diseases include lower limb numbness, intermittent claudication, rest pain, ischaemic ulcers or gangrene and amputation.4–6 Recently, there has been an increased chronic lower extremity angiopathy incidence, accounting for approximately 50% of peripheral vascular diseases, which are the leading causes of foot ulcers and can easily interfere with ulcer healing.7 The treatment is mainly based on the stages and grades of diseases depending on which the corresponding treatment measures are adopted. Presently, conventional treatment for lower extremity angiopathy includes drug therapy, local debridement, free skin flap grafting, vascular bypass and interventional therapy.8–10 The mild cases are usually conservatively managed with drugs. In contrast, surgical intervention is usually required for severe cases due to poor drug effects.11 Interventional therapy and other surgical methods can recanalise part of the large and medium vessels; however, they cannot reconstruct the microcirculation system involved in the tissue survival and repair, resulting in patients who are exposed to high amputation risks.12 Therefore, it is important to explore novel methods for treating such diseases. Recently, significant progress has been made using the tibial transverse transport (TTT) technique in microcirculation reconstruction. Moreover, good outcomes have been achieved in its chronic lower extremity angiopathy treatment. The TTT technique can not only improve ischaemia and relieve pain but also promote refractory ulcer wound healing.13 14
In the 1980s, Ilizarov proposed the ‘tension-stress rule,’ in which tissue was repaired under slow, sustained and stable traction stimulation,15 16 The Ilizarov technology was developed on this basis. Bone regeneration can be achieved through distraction osteogenesis using Ilizarov’s external fixators. It was mainly used to treat congenital limb malformations, extended bone defects, bone nonunion and other diseases in the early stages.17 The traditional distraction osteogenesis concept was expanded in both theory and practice with the wide application of Ilizarov technology. TTT technology based on the ‘tension-stress rule’ was proposed. TTT technology first intercepts a movable bone flap from the affected limb, and then the bone flap is transversely transported with an external fixator. As a novel treatment, the TTT method is advantageous owing to its short operation time, simple technique and high-limb saving rate.5 18 TTT technology can accelerate the microcirculation system reconstruction, promote nerve recovery and repair refractory ulcers through continuous stimulation of movable tibia flap.19 20 This technique focuses on local tissue regeneration and not bone formation. Rauch et al confirmed that sustaining stress stimulation would regenerate the vascular network in the traction area and promote wound healing through traction experiments on rabbit bone tissue.21 In 1997, Shevtsov and Shurov first applied TTT technique in thromboangiitis obliterans therapy.22 Qu et al also used TTT technology to treat chronic lower extremity angiopathy, develop surgical instruments and improve the surgical protocol.23 Hua et al applied TTT technology to treat moderate and severe diabetic foot; all diabetic foot ulcers healed after surgery with an average healing time of 10–15 weeks. The lower extremity arteries’ CT showed that collateral circulation was open, some of the blood vessels were newly born or recanalised, and blood flow was accelerated.24 After decades of clinical practice and exploration, TTT technology has achieved a limb-saving rate of 97% for diseases requiring amputation at the terminal stage.20
The TTT technique is a complex intervention. Although its effectiveness in treating chronic lower extremity angiopathy has been confirmed in a few clinical trials, its exact effectiveness remains to be further verified. In addition, there have been no meta-analyses in this area. We hypothesised that for patients with chronic lower extremity angiopathy, TTT technology would be more beneficial in increasing the wound healing rate, avoiding amputation, relieving pain, reducing complications and improving the quality of life compared with conventional treatment. Therefore, we proposed a novel and comprehensive meta-analysis to verify TTT’s effectiveness in chronic lower extremity angiopathy patients.
Methods and analysis
Study registration
The protocol will be performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Protocols guidelines (online supplemental table 1).25
Supplemental material
Eligibility criteria
Study types
All cohort studies and randomised controlled trials (RCTs) on TTT for chronic lower extremity angiopathy will be included in this review. All included articles will be reported in Chinese or English. Articles on experimental animal studies, narrative reviews, case reports and conference articles will be excluded.
Participant types
Patients with chronic lower extremity angiopathy will be included. There is no restriction on race, age, gender, educational background and geographical location.
Intervention types
The patients in the experimental group underwent TTT with conventional therapy or TTT alone. There were no external fixation time, surgical time or bone transport method restrictions. Patients in the control group underwent conventional treatment, including debridement, vacuum-sealing drainage, flap reconstruction, revascularisation and drug therapy.
Types of outcome measures
The primary outcomes were the healing time and rate. The additional outcomes were Ankle Brachial Index (ABI), amputation rate, ankle skin temperature, Visual Analogue Scale (VAS), hospitalisation time, vascular endothelial growth factor (VEGF), effective rate and complications. Complications include pin tract and incision infection, tibial shaft fracture and osteomyelitis.
Search strategy
Electronic searches
Relevant studies were acquired by searching the following databases: Cochrane Library, Embase, PubMed, Web of Science, China National Knowledge Infrastructure (CNKI), China Science Technology Journal Database (VIP), Wanfang Data and Chinese Biomedical Literature Service System (CBM) until 20 September 2021. We searched the aforementioned databases and websites by combining Medical Subject Headings and keywords to avoid missing literature. The following search terms were used: (1) tibial transverse transport, transverse tibial bone transport, proximal tibial cortex transverse distraction, Ilizarov technique, Ilizarov technology, Ilizarov; (2) lower extremity angiopathy, lower extremity vascular disease; (3) diabetic foot, diabetic feet, diabetic angiopathies, foot ulcer; (4) arteriosclerosis obliterans, obliterans, arteriosclerosis, thromboangiitis obliterans and (5) Buerger’s disease. The search strategy for PubMed is presented in online supplemental table 2. We also searched the Chinese databases using the same search strategy.
Supplemental material
Other search methods
Two reviewers (HB and YZ) searched the ClinicalTrials.gov, Chinese Clinical Trial Registry, dissertations and grey literature to identify eligible studies. Additionally, meta-analyses involving TTT’s effects were searched for potentially missed eligible studies. The reference lists of included studies were examined to determine potentially eligible studies. The corresponding authors were contacted for any incomplete information.
Data collection and analysis
Studies selection
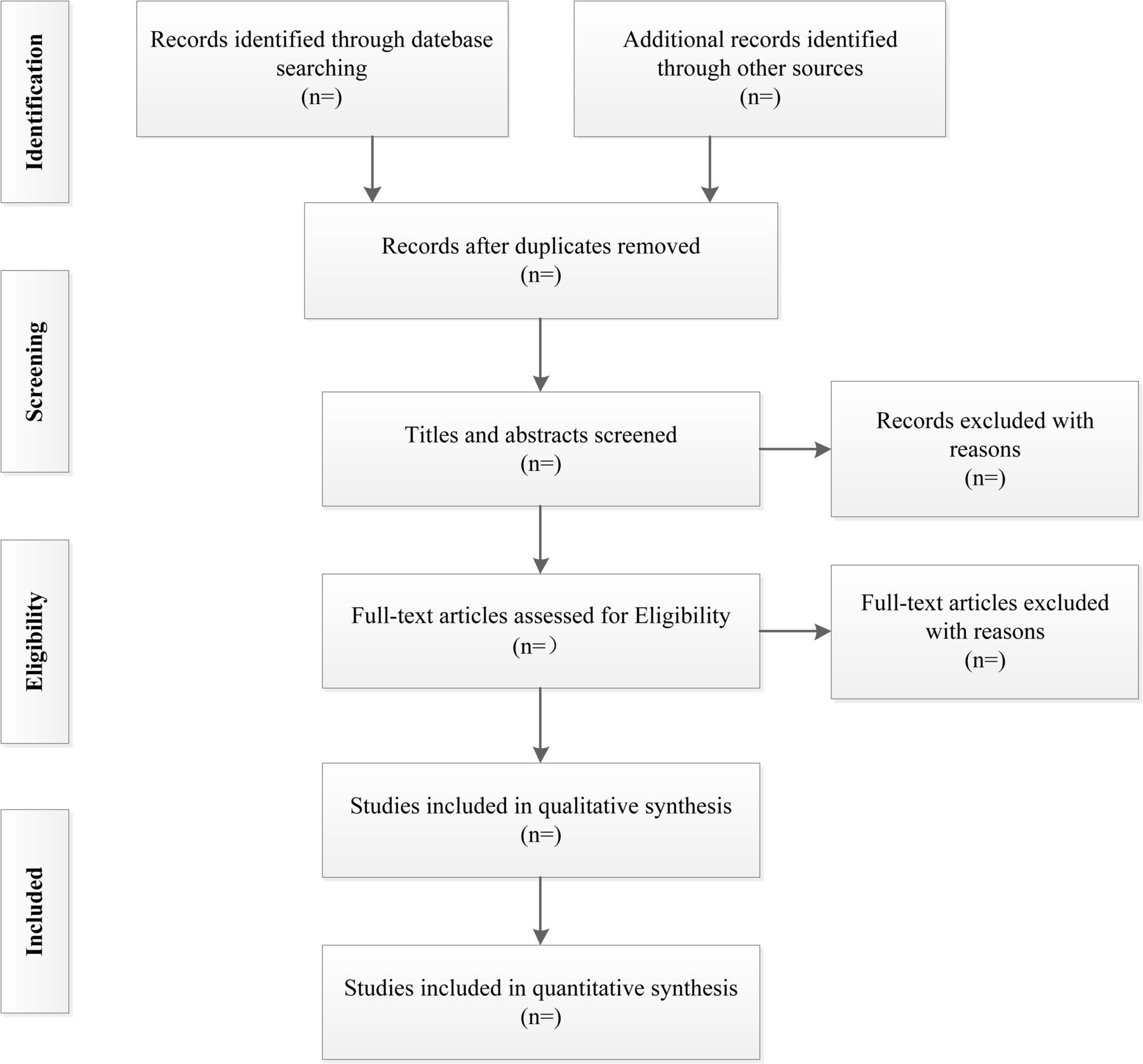
Endnote V.X9 software will be used to screen the studies searched in electronic databases and websites. First, two reviewers (HB and YZ) will reject all duplicate studies according to the inclusion and exclusion criteria. Next, they will preliminarily screen the titles and abstracts of the searched studies to remove ineligible ones. Finally, they will read the complete text independently to evaluate whether the studies meet the inclusion criteria. A third author (Lideer) will decide if there is any disagreement during this process. The study selection process is presented in figure 1 according to the PRISMA flow chart.
{kind=link}
Flow diagram of the study selection process.
Data extraction
Based on the inclusion criteria, two reviewers (HB and XN) will extract valuable information from the included studies: study details (title, first author, publication year, and study method), participant’s details (sample size, sex, age, and type, duration, and severity of disease), therapy method (TTT type, conventional treatment type), primary outcomes (healing time and rate) and additional outcomes (ABI, VAS, VEGF, amputation rate, ankle skin temperature, hospitalisation time, effective rate and complications). A third author (Lideer) will decide if there is any disagreement during this process.
Assessment of study quality
Two independent reviewers (Huhe and XN) will adopt the Cochrane risk-of-bias assessment tool to assess RCTs quality,26 including the following aspects: (1) selection bias, (2) performance bias, (3) detection bias, (4) attrition bias, (5) reporting bias and(6) other potential biases. Each quality item will be classified into three levels: high risk, unclear risk or low risk. It is difficult to maintain blinding of the patients and clinicians in these trials, which will have a limited impact on the trial outcomes. Therefore, the reviewers judged that the trial outcomes were not likely affected even without double-blinding, and trials will be seen as low risk. A bias risk diagram will be produced graphically using Review Manager V.5.3. The risk of bias for cohort studies will be evaluated using the Newcastle-Ottawa Scale (NOS).27 The NOS comprises three parts: selection, exposure and comparability. Cohort studies with scores ≥7 will be considered to have high quality. A third author (Lideer) will decide if there is any disagreement during this process.
Statistical analyses and data analyses
Two reviewers (XN and YZ) will use Stata V.16.0 software and Review Manager V.5.3 software to implement the statistical analyses. They will analyse ORs with 95% CIs for dichotomous outcomes; they will analyse the mean difference or standardised mean difference with 95% CI for continuous outcomes, depending on whether the different scales of the same outcome measure were used. We consider a p<0.05 is statistically significant.
Heterogeneity analyses
Statistical heterogeneity among the included studies will be assessed using the χ2 and I2 tests. I2 >0.5 or p<0.1 will indicate the presence of significant heterogeneity among the studies.28 Later, we will analyse the heterogeneity source and adopt the random effect model. Otherwise, a fixed-effect model will be selected.
Subgroup and sensitivity analyses
If there is considerable heterogeneity and sufficient data, subgroup analyses will be performed to identify the underlying heterogeneity causes. The criteria for subgroup analysis potentially included diseases, age and follow-up time. However, we will perform subgroup analyses between traditional and minimally invasive surgery due to the different degrees of trauma among surgical methods. We will also perform subgroup analyses on TTT protocol when the data are sufficient.
The meta-analysis result stability will be assessed using sensitivity analysis. We will compare the before and after results by removing each study individually. A descriptive summary will be conducted when a meta-analysis is unfeasible due to significant statistical heterogeneity.
Publication bias assessment
Funnel plots will be used to examine publication bias when the number of eligible studies is ≥10. Additionally, Egger and Begg test will be quantitatively performed to examine publication bias using Stata V.16.0 software.29 30
Evaluating the quality of evidence
The overall evidence quality will be evaluated under the Grading of Recommendations Assessment, Development and Evaluation guidance, classified into four categories: high, moderate, low and very low.31
Amendments
The amendments to the protocol will be explained in the final systematic review and meta-analysis section.
Patient and public involvement
Patients and the public will not be involved in this research’s design, implementation, reporting or dissemination.
Ethics and dissemination
This study was based on previous data. The medical ethics committee of Inner Mongolia People’s Hospital, located in China waived the need for formal approval of this research, as this study did not fall under the principles of the Declaration of Helsinki. The results will be disseminated through peer-reviewed journals or relevant conferences.
Discussion
Several meta-analyses have been conducted to assess TTT’s effect on diabetic foot.32–34 These previous reviews found that the TTT technique is highly safe and has significant advantages over conventional diabetic foot treatments. However, these studies only compared partial outcome indicators for diabetic foot treatment with TTT, and did not conduct statistical analysis of various postoperative complications. Similarly, these studies did not perform a subgroup analysis of conventional treatment methods, which may reduce the conclusions’ credibility. Our proposed system evaluation method has several advantages. First, we included different chronic lower extremity angiopathy types in the overall review, and the results were more practical and general. Second, the outcome indicators of TTT in chronic lower extremity angiopathy treatment are relatively comprehensive. Third, if the data are sufficient, a series of subgroup analyses will be conducted to improve the conclusions’ credibility.
However, this study has some limitations. First, it is unclear whether uncontrolled or unmeasured confounding factors might cause confounding bias. Second, it is also unclear whether all patients strictly followed the treatment options, which may lead to selection bias.
In conclusion, this study aims to assess the efficacy and safety of TTT in chronic lower extremity angiopathy treatment. TTT may be a good choice for treating these diseases if significant efficacy is observed.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank professor Guanwen Sun and Editage for English language editing.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
JG and YZ are joint first authors.
Contributors JG, HB, YZ and GS initiated the idea and led the development of this protocol. All authors formulated the search strategy which was implemented by HB and YZ. HB, XN and YZ will participate in the work of studies selection, data extraction and data synthesis. Huhe and XN will carry out the assessment of study quality and bias. Lideer will make the final decision if there is any disagreement during all processes. All authors authorised the publication of this protocol.
Funding This study was funded by the doctoral research start-up fund of Inner Mongolia People’s Hospital (2020BS01).
Disclaimer The funder had no role in the study design, data analysis and writing the manuscript.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.