Article Text

Abstract
Objective To map the recommendations for hospitalised patient safety in the context of the COVID-19 pandemic.
Design Scoping review using the method recommended by the Joanna Briggs Institute.
Data sources Databases: Medline, SCOPUS, EMBASE, ScienceDirect, LILACS, CINAHL and IBECS; grey literature platform: Google Scholar; and 11 official websites of leading healthcare institutions were searched on 27 April 2021 and updated on 11 April 2022.
Eligibility criteria We included documents that present recommendations for the safety of hospitalised patients in the context of the COVID-19 pandemic, published in any language, from 2020 onwards.
Data extraction and synthesis Data extraction was performed in pairs with consensus rounds. A descriptive analysis was carried out to present the main characteristics of the articles. Qualitative data from the extraction of recommendations were analysed through content analysis.
Results One hundred and twenty-five documents were included. Most papers were identified as expert consensus (n=56, 44.8%). Forty-six recommendations were identified for the safety of hospitalised patients: 17 relating to the reorganisation of health services related to the flow of patients, the management of human and material resources and the reorganisation of the hospital environment; 11 on the approach to the airways and the prevention of the spread of aerosols; 11 related to sanitary and hygiene issues; 4 about proper use of personal protective equipment and 3 for effective communication.
Conclusions The recommendations mapped in this scoping review present the best practices produced so far and serve as a basis for planning and implementing good practices to ensure safe hospital care, during and after COVID-19. The engagement of everyone involved in the care of hospitalised patients is essential to consolidate the mapped recommendations and provide dignified, safe and quality care.
- COVID-19
- health & safety
- quality in health care
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The extensive search made by the review, involving scientific databases, grey literature and official documents from reference health institutions, together with the rigorously applied method, corroborate the reliability of the data presented.
The review process was performed independently by peer reviewers, and the research team was trained to conduct scoping reviews and developed a prior research protocol, which gave greater reliability.
The primary weakness of this review is that most studies are those of the expert consensus type.
Nevertheless, as the context is that of a pandemic, both clinical practice guidelines and expert opinion are the best available evidence.
The grouping and analysis of results followed methodological rigour for qualitative data and the experience and diversity of the research team increased reliability.
Background
COVID-19 is an infectious disease caused by a highly transmissible virus, the new SARS-CoV-2, which may develop into a severe clinical state of respiratory failure.1–3 In March 2020, the disease was declared a global pandemic, imposing an extra burden on structures, equipment, inputs and human resources of health services, and this substantially challenged the health systems of several countries.4 5
The rapid and drastic changes in the care models imposed by the COVID-19 pandemic increased the workload, causing the relocation of staff and the cancellation of elective services, in addition to the treatment of a new disease. These challenging conditions impacted the performance of health teams to provide safe and quality healthcare. Studies indicate that increased pressure at work, inadequate staff and worker fatigue are factors that contribute to poor safety. In the COVID-19 pandemic, there was evidence of change in the perception of patient safety, risks in different professional categories and a reduction in notifications of incidents6–8
This context highlighted the need to develop strategies and recommendations to face the pandemic. Some institutions such as WHO, the International Society for Quality in Health Care (ISQua) and the Centers for Disease Control and Prevention (CDC) have provided daily updated information, protocols and recommendations to ensure the standardisation of safe and quality care.6 In addition to institutional publications, the scientific community has committed itself to disseminating experiences, practices and research related to hospitalised patient care in the context of the pandemic, resulting in a high number of publications on the subject. In this context, it has become important to organise the recommendations regarding patient safety. This scoping review seeks to map the recommendations for the safety of hospitalised patients in the context of the COVID-19 pandemic.
Method
Study design
This is a scoping review whose aims, inclusion criteria and methods were specified in advance and which had a registered protocol.9 It was prepared using the method recommended by the Joanna Briggs Institute,10 consisting of an exploratory review.11
Eligibility criteria
The research question of this study was elaborated according to the PCC mnemonic combination12 (P: population—hospitalised patient; C: concept—recommendations for patient safety; C: context—COVID-19 pandemic), with the following guiding question:
What are the recommendations for the safety of hospitalised patients in the context of the COVID-19 pandemic?
The refinement of the articles found was based on pre-established eligibility criteria, which were: documents that present recommendations for the safety of hospitalised patients in the context of the COVID-19 pandemic, published in any language, from 2020 onwards, of all age groups and hospital units. The practices described in the documents as imperative to ensure patient safety were considered as recommendations.
Exclusion criteria: studies that did not meet the aim or answer the question, full text unavailable in electronic media, websites/electronic portals with restricted access and research projects.
Electronic search
The search strategy was developed by the researchers with the support of a librarian with extensive experience in carrying out reviews and followed the definition of each database/portal or directory, taking place from 1 to 27 April 2021 and updated on 11 April 2022. The descriptors and keywords used were ‘patient safety’, ‘COVID-19’, ‘hospitalisation’, ‘recommendation’ and their variations. The Boolean operator AND and OR was used. The search terms and strategy are detailed in the online supplemental appendix A.
Supplemental material
The searches from the beginning took place in the following databases: Medline Complete (PubMed), SCOPUS (Elsevier), EMBASE (Elsevier), ScienceDirect (Elsevier), LILACS (Bireme), CINAHL Complete (EBSCO), IBECS (Bireme); grey literature: Google Scholar and official websites: WHO, CDC Institute for Healthcare Improvement, ISQua, Agency for Healthcare Research and Quality, National Health Services (NHS Improvement), National Institute for Health and Care Excellence, Ministry of Health, National Health Surveillance Agency, Brazilian Society for Quality of Care and Patient Safety and Collaborating Centre for the Quality of Care and Patient Safety.
Data charting process
The exploratory reading of titles and abstracts was performed independently by peer reviewers, classifying the studies that were related to the research question and met the inclusion criteria. Disagreements were resolved by consensus between peers or by the assessment of a third reviewer if the disagreement continued. The preselected studies were then read in full to evaluate the content as to their contribution to the understanding of the studied phenomenon and subsequent data synthesis. The reference lists of articles were then consulted to discover additional studies. All research, decisions and stages were documented and archived by the lead reviewer.
In the data extraction stage, a standardised data abstraction form (online supplemental appendix B) was used. This provided the identification of the essential elements of the studies such as database, author(s), title, DOI/access link, year of publication, country, collection period, study site/institution, aims, methods (type of research, age/age group, sample size, data analysis) and results (hospital sector, patient safety recommendations). Data extraction was performed in pairs with consensus rounds.
Supplemental material
Data analysis and synthesis of results
A descriptive analysis was performed to present the main characteristics of the articles. Qualitative data from the extraction of recommendations were analysed through content analysis, according to the framework of Bardin,13 covering the pre-analysis, material exploration, data processing, inference and interpretation steps. The units of analysis were grouped by theme and then reviewed in pairs and consensus rounds. After the interpretations, the categories of recommendations, subcategories and the details of each recommendation were defined, through a reflective process, seeking rigour in terms of the references of the studies.
All analyses were conducted in pairs and discussed in consensus rounds with the review group. A synoptic table with the main characteristics of the studies was elaborated for the compilation and communication of the results, aiming to present an overview of all the material. The recommendations found in the literature were categorised and illustrated.
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Results
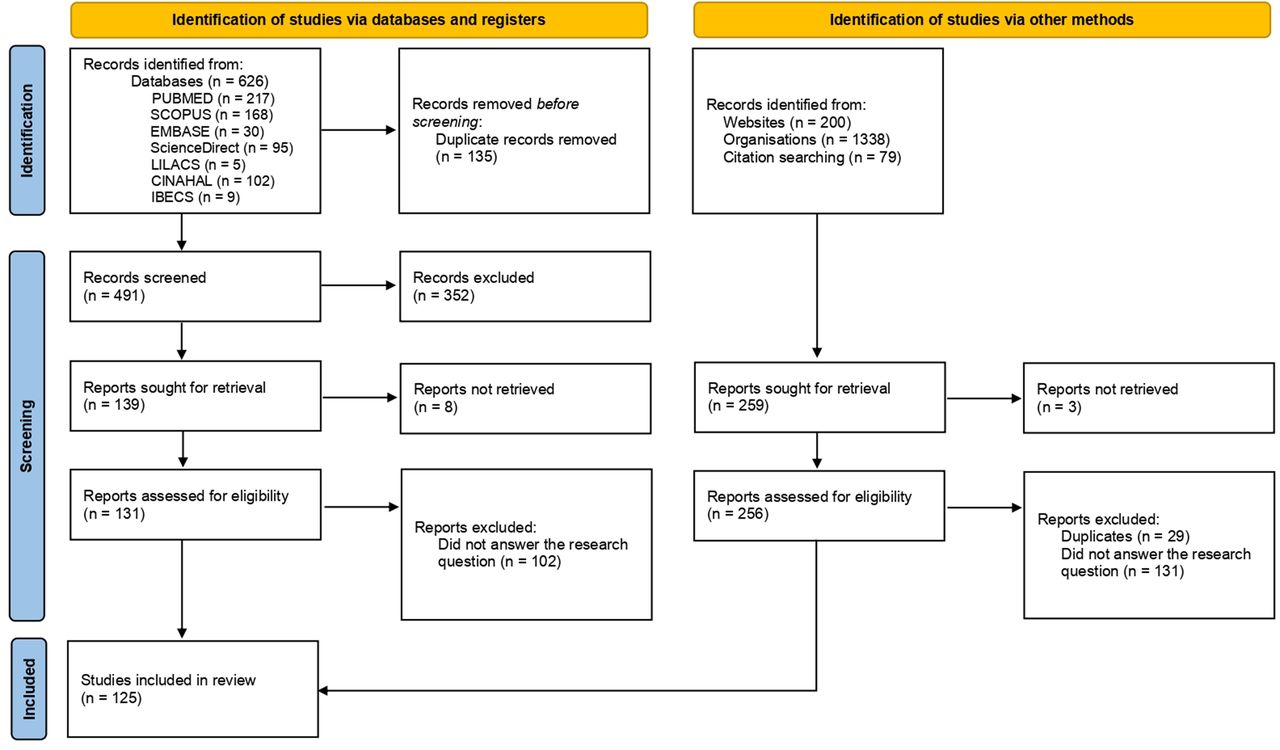
One hundred and twenty-five documents were included (figure 1).14 The online supplemental appendix C presents a summary, including the main author, year of publication, study origin, objective, method, setting, country and main recommendations presented. Most papers were identified as expert consensus (n=56, 44.8%), followed by literature review (n=35, 28.0%). Many articles described specific recommendations for performing intubation15–19 or for certain areas, such as psychiatric services,20–22 orthopaedics,23 haemodynamic,24 intrahospital transport,25 oncology,26 27 field hospitals,28 29 paediatrics,30–34 diagnostic centres,35–37 inpatient units,38–43 endoscopy and gastroenterology centres,44–48 gynaecology and obstetrics,40 49–55 emergency units,56–60 intensive care unit40 41 56 61–68 and the most common was the surgical centres.48 61 69–99 Other articles made recommendations for the hospital service as a whole.19 58 64 100–138 Most documents are from the USA (n=34, 27.2%), followed by Brazil (n=21, 16.8%) and multicentre studies (n=17, 13.6%). The documents were published in 2020 (n=76, 60.8%), 2021 (n=39, 31.2%) and 2022 (n=10, 8.0%). Table 1 summarises the main features of the items included.
Supplemental material

Preferred Reporting Items for Systematic Reviews and Meta-Analyses study selection flow diagram.
Main characteristics of included papers
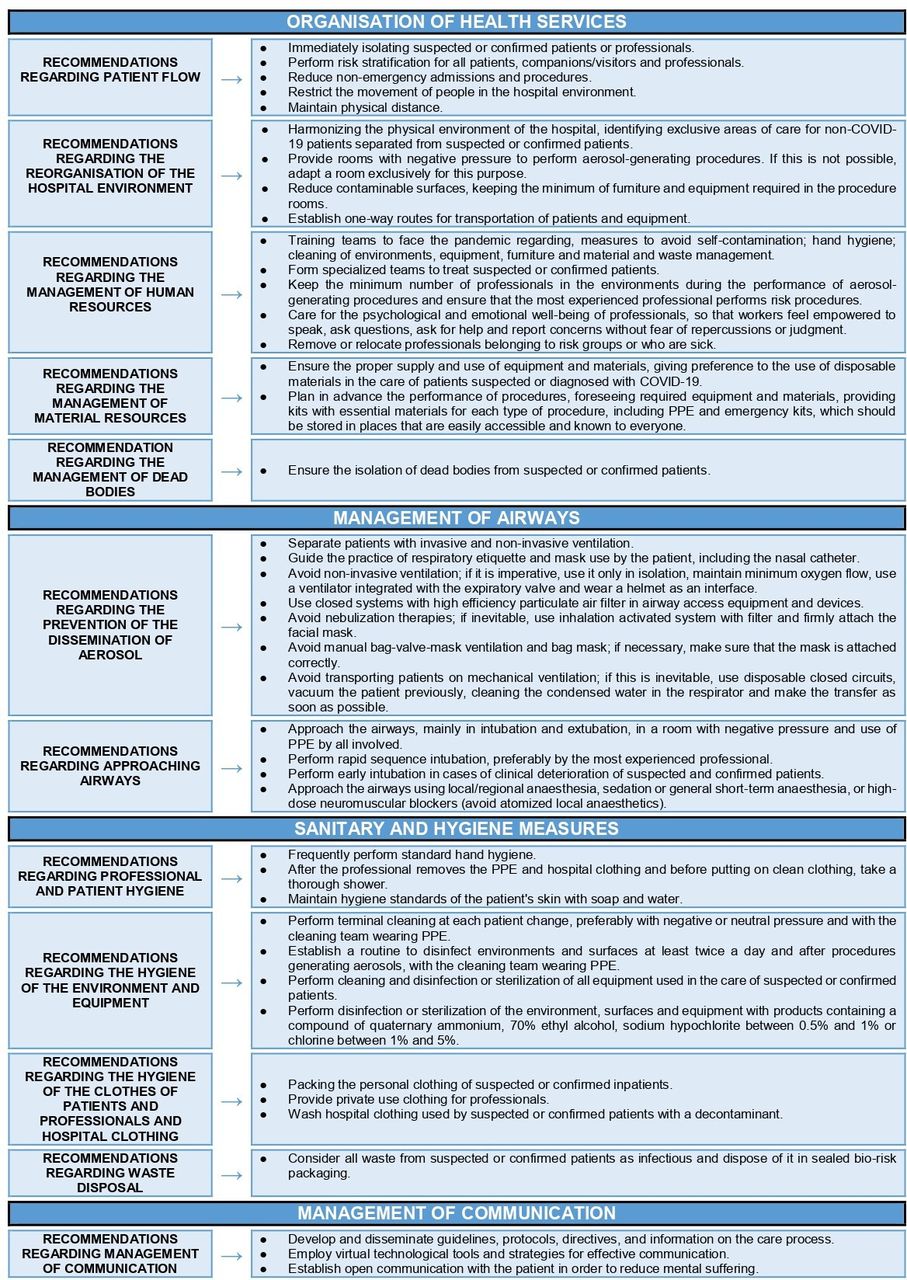
Analysis of the documents revealed specific recommendations, which were later grouped into categories and subcategories. Each recommendation was built from the examined literature, and the online supplemental appendix D presents in detail the basis for the construction of each recommendation, as well as all related references. The data enabled the construction of 46 recommendations for the safety of hospitalised patients, 17 relating to the reorganisation of health services, 11 for airway management, 11 for sanitary and hygiene measures and 3 for communication management (figure 2).
Supplemental material

{kind=link}
{kind=link}
Recommendations for the safety of hospitalised patients.
The four recommendations related to personal protective equipment (PPE) have greater specificity and detail and for better visualisation are presented box 1.
Personal protective equipment (PPE) management recommendations
Manage forecast and provision of PPE.
Train the team, patients and family members to wear PPE.
Management of PPE by professionals:
Correct use of PPE, following institutional and regulatory agency guidelines:
Masks;
Respiratory protection mask (particulate respirator), tested for fit, with a minimum efficiency in the filtration of 95% of particles up to 0.3 µm must be worn during surgeries, transport and in the execution of aerosol-generating procedures in suspected or confirmed patients;
Surgical mask must be routinely worn in the hospital environment;
Disposable head protector must be worn for performing aerosol-generating procedures and during transport and surgery of suspected or confirmed patients;
Long gowns and coveralls, with long waterproof sleeves routinely worn in the care of the suspected or confirmed patient are strongly recommended in the performance of surgeries, aerosol-generating procedures and cardiopulmonary resuscitation;
Disposable gloves must be routinely worn in the direct care of hospitalised patients;
Face shields routinely worn in the care of suspected or confirmed patients are strongly recommended in aerosol-generating procedures, transport and in the operating room;
Eye protection/protection goggles routinely worn in the care of suspected or confirmed patients are strongly recommended in aerosol-generating procedures, transport and in the operating room;
Shoes, boots or overshoes resistant to fluids and easy to routinely decontaminate in the care of suspected or confirmed patients are strongly recommended in procedures that generate aerosols, transport and in the operating room.
Follow the PPE wearing process, under the supervision of an experienced professional, in the following order: disposable hair cover, N95 respirator tested for adjustment, fluid-resistant gown, two layers of gloves, protection goggles and face shield, fluid-resistant shoe covers.
Remove PPE in the following order: sanitise hands and remove face shield, protection goggles, fluid-resistant apron, outer gloves, shoe covers and inner gloves; then sanitise hands again and remove the N95 mask and hair cover under the supervision of an experienced professional. Dispose of everything in the recommended place.
Perform the management of PPE by patients and visitors/companions:
Provide PPE to patients and visitors/companions and instruct them on its correct use.
All patients (not COVID-19, suspected and confirmed) must wear a surgical mask over the face, tracheostomy tube, ventilation face mask, nasal catheter and prongs.
Suspected and confirmed patients must wear N95 mask or similar.
Visitors of patients with COVID-19 should wear a surgical mask, disposable gowns and coveralls and gloves.
Reorganisation of the health services
The reorganisation of the health services category addresses 17 recommendations related to the flow of patients, the management of human and material resources and the reorganisation of the hospital environment in order to prevent the transmission of COVID-19. It is recommended that all patients are considered suspects47 70 80 90 91 101 128 and undergo risk stratification20 21 23 24 27 31 32 36 39 43–47 49 53 66 70 72–74 76 81 85 91 93 100–102 108 110 119 125 126 133 135 139 with a history of clinical and epidemiological data20 22–24 39 45–47 49 72 81 92 93 95 96 101 124–126 133–135 and a test20 22 23 26 30 39 48–51 53 61 65 68 72 73 81 84 90 92 96 102 110 119 124 133 of RT-PCR,23 36 47 69 72 81 87 88 91 96 119 125 126 133 134 ELISA23 47 or nasal swab84 95 101 at admission screening,21 22 36 39 49–51 53 69 95 108 133 in the preoperative period,23 26 47 48 61 69 72 87 90 95 102 124 in referrals31 84 and before non-emergency procedures involving airway approaches.66 79 95
Suspected and confirmed patients should be isolated,20 21 23 30 32 38 40 42 43 50–54 59 60 66 69 76 78 91 96 100–102 104 108 110 119 124 126 129 133 134 139 preferably in single rooms with negative pressure.65 67 76 79 112 117 120 123 134 If this is not possible, a minimum distance of 1 m should be maintained between beds in collective isolation.20 32 38 40 53 120 123 128 131 139 Preference should be given to the use of disposable materials in the care of health workers40 47 70 76 107 129 and a one-way, short and direct route for transport should be used, avoiding contact with patients without COVID-19.23 31 32 35 38 47 56 60 69 78 89 98 115 134 In case of death, the body must be wrapped in a sheet soaked in a disinfectant solution and placed in the coffin.101 128
Aerosol-generating surgeries and procedures must be performed in rooms with negative pressure.18 19 30 44 46–48 53 62 66 67 69 70 75–77 79 84 87 89 91–94 98 120 128 131 137 139 If this is not possible, for procedures it is recommended to adapt a room that has natural ventilation with open windows with bars,18 35 56 100 110 120 137 139 high efficiency particulate air filter44 47 73 84 89 98 112 120 137 139 and doors to other environments must be kept closed.47 67 70 89 91 100 120 139
Health professionals must undergo daily risk stratification20 23 36 39 46 67 93 100 101 124–126 133 and be tested periodically.19–21 23 34 39 73 87 91 100 125–127 133 Those who are suspected or confirmed must be removed immediately.20 23 103 118–121 127 139
To reduce the movement of people, hospitalisations and elective procedures should be suspended,20 23 26 36 37 40 46 48 51 52 69 72 75 76 84 91 95 96 98 100 101 108 110 124 125 134 the number of professionals in the areas of patients with COVID-19 should be kept to a minimum15 17 18 23 26 27 33 36 37 46–48 53 60 65 66 70 75 76 78 83–85 90 94 97–100 102 104 139 and family visits to patients should also be restricted.20–22 32 38 40 46 48 49 52–55 68 81 96 100 101 104 108 119 129 130 135 139
The teams must be trained18 25 27 49 54 85 107 125 126 128 regarding: measures to avoid self-contamination21 23 46 101 120; hand hygiene17 20 29 46 101 102 126 128; cleaning of environments,29 35 126 equipment,29 35 65 126 furniture and materials29 35 and waste management.18 29
Contaminated equipment and materials must be transported along a one-way route.25 45 60 66 67 85 101 128
Airway management
Eleven recommendations were created regarding the approach to the airways and the prevention of the spread of aerosols. Airway management should be performed early in clinically deteriorating patients,25 31 40 58 64 67 76 111 117 avoiding emergency procedures.15 18 31 67 111 Intubation must be carried out soon after,16 31 94 107 111 118 and airway and upper trunk interventions (thoracotomy, endoscopy) must be performed by the most experienced professional.15–18 31 40 58 63 65 66 83 84 89 94 97 118 124 129 135
To prevent the spread of aerosols, it is recommended to avoid manual ventilation with the airway maintenance breathing unit,16 65 80 94 nebulisation therapies56 101 and non-invasive ventilation.16 70 91 107 129 As some of these procedures are essential, closed systems,31 65 91 111 117 123 disposable47 70 and with filter17 23 31 56 87 92 98 110 118 120 must be used, and are only performed in an environment with negative pressure.18 48 58 69 71 75 84 85 97 98 100 118 The patient must be sedated for intubation, bronchoscopy and tracheostomy placement.17 47 56 65 84 85 94 97 114 118 124 Extubation and aspiration should be conducted with strategies to minimise coughing.47 76 77 80 91 110 117 118
Sanitary and hygiene measures
The 11 recommendations related to sanitary and hygiene issues propose that professionals keep their nails short, avoid wearing rings, bracelets, watches and other adornments37 40 44 58 102 127 137 139; wear private clothing in the hospital environment93 110 and take a complete shower after removing the PPE and before putting on clean clothing.47 70 93 110 111 Patients should clean their skin with soap and water102 110 and pack their personal clothes in sealed bags.47 70 102 Everyone (patients, accompanying persons and professionals) must wash their hands frequently, with standard technique, using alcohol products when they are visibly clean or soap and water when they are dirty.16 20 22 24 28 32–34 38–40 44 47 48 51 55 56 58 59 63 65 73 74 78 80 94 96 99–102 104 105 107 109 112 115 119–124 129–132 135 138 139
It is recommended that the environment and surfaces are disinfected twice a day and after each aerosol-generating procedure,21–23 54–56 59 76 77 96 105 107 117 121–123 129 131–134 138 139 and terminal cleaning at each patient rotation.35 44 51 54 89 98 126 128 137 139 Equipment must be cleaned after each use35 40 46 52 74 76 77 105 107 129 132 134 139 and disinfected or sterilised between one patient and another, in the case of shared equipment.52 69 99 100 123 126 128 To clean and disinfect the environment and equipment, use soap and water40 or disinfectants containing a quaternary ammonium compound,49 139 70% ethyl alcohol,15 18 20 28 30 31 37 39 40 44 47 49 51 56 57 78 89 97 100 104 105 108 110 118 129 132 134 139 sodium hypochlorite between 0.5% and 1%15 18 28 30 31 39 40 44 47 51 55 57 78 89 97 100 104 108 110 118 132 134 139 or chlorine between 1% and 5%20 137; and sterilise N95 respirators with hydrogen peroxide or ultraviolet-C.82 100 Hospital clothing should be washed with hot water (60°C–90°C) and soap or a textile decontaminant.102
Personal protective equipment management
Four recommendations related to PPE were created, but each one of them has specific consequences. Health professionals should use PPE properly, following institutional and regulatory agency guidelines.15–18 20–23 25 26 30–33 35 36 38 41 42 44–48 50–53 56–58 60–69 71 72 74–79 82–92 94 96–98 100–102 104–112 115 117 118 120–125 127–129 131–137 139 Forecasting and provision must be made for the supply of sufficient quantity and to avoid shortages.21 24 25 39 42 67 72 99 101 108 112 115 119 125
All workers must wear a surgical mask in the hospital environment.23 30 32–34 51–55 57 60 64 69 72–76 80 81 86 89 93 96 102 107 108 112 115 120–124 127–129 133 135–137 139 In the care of suspected or confirmed patients, health professionals must be properly dressed with: respiratory protection masks with a minimum efficiency of 95% in the filtration of particles up to 0.3 µm15–17 22 23 25 30–33 43 44 46 47 50–53 55–58 61 64 65 69 71–74 76 78 80 82–87 89–91 93 96 97 99 100 102 105 107 108 111 115 118 124–129 134–137 139; powered air purifying respirator15 16 25 43 45 58 61 64 65 69 71 74 76 80 84 85 89 90 102 111 115; disposable head protector16 17 31 44 47 56 72 76 78 80 87 91 97 100 102 108 112 115 118 125 126 129 139; long gowns and coveralls, with long, waterproof sleeves15–17 22 23 30–33 43 44 47 51–53 56 58 60 65 69 71 72 74 78 80 82 84 86 87 91 93 94 96 97 100 102 107 111 112 115 118 121–126 128 129 132 133 135 136 139; disposable gloves16–18 22 23 30–33 44 47 51–53 56 60 61 69 71 74 76 82 84 86 87 91 93 96 100 102 107 108 111 112 115 118 120–126 128 129 132 133 136 139; double gloves15 16 18 31 43 47 58 61 65 69 74 78 80 84 87 94 97 102 112 118 124 135; face shield15–17 31 32 44 46 47 52 53 56 64 69 73 78 83 84 86 87 97 100 102 107 111 115 118 129 135 139; goggles/eye protection15 16 22 23 30–33 43 44 46 47 51–53 56 64 71–74 76 78 80 82 84 86 87 89 91 93 96 97 100 102 107 111 112 115 118 120–126 128 129 136; waterproof shoes, boots or wellies31 33 79 91 113–116 134 and disposable and waterproof protector for shoes,16 31 43 47 56 70 72 86 111 in aerosol-generating procedures,15 17 18 22 23 26 32 35 36 41 44–48 50 51 53 56 58 61 64–66 69 71 73–75 77–80 83–87 89 90 92 97–99 101 102 104–111 115 117 118 120–123 126 129 135 136 transport17 18 20 25 35 44 45 47 78 80 84 87 89 101 106 109 115 117 133 and in operating rooms.15 18 26 32 45–48 50–53 61 69 75 77 78 80 83 84 87 97–99 104 105 110 112 115 117 134 Professionals must be trained in the proper management of PPE,17 18 21 24 25 28 29 31 32 34–38 40 42 44 46 49 51 54 69 76 78 96 100–102 107 108 119 124 132–134 139 including placement and removal in the proper sequence.17 18 21 38 47 58 59 65 67 70–72 78 94 96 99 118
Patients and accompanying persons should be instructed in the proper use of PPE.19 20 24 25 30–32 34–36 44–46 49 51–53 56 64 71 73–75 78 84 87–91 96 100–102 108 115 124 134 139 All patients (patients without COVID-19, and those who are suspected and confirmed for COVID-19) must wear a surgical mask over the face, tracheostomy tube, ventilation face mask, nasal catheter and prongs.19–25 30–32 34–36 44–46 51–53 56 64 66 71–75 78 84 87 89–91 93 96 97 100–102 108 115 119 124 127 130 134 135 137 139
Communication management
For effective communication, three recommendations were made. Guidelines and information on care processes20 28 46 87 101 128 131 should be developed and disseminated through effective communication strategies15 17 20 22 26 28 35 49 51 69–71 75 92 103 108 114 116 134 and virtual technological tools.20 26 30 37 39 58 85 90 101 103 106 116 134 Open communication must be guaranteed to alleviate mental suffering for patients and workers.101
Discussion
Overall, studies have shown that to ensure hospitalised patient safety in the context of the COVID-19 pandemic, it is recommended that hospitals reorganise the hospital environment and patient flow and replan the management of human and material resources and of dead bodies. The approach and management of the airways must be carried out in a way so as to prevent the spread of aerosols. Intubation must be performed in rapid sequence, preferably by the most experienced professional, and patients with invasive and non-invasive ventilation must be separated. Sanitary and hygiene measures must be taken by patients, accompanying persons, professionals and institutions, and the main measure is the correct and frequent washing of hands. Forecast, provision and management of PPE is necessary, and the team, patients and family members must be trained in its use. Finally, guidelines and protocols with information on fighting the pandemic, with effective strategies for patients and professionals must be developed and disseminated.
The global presence of COVID-19 and the way in which it is transmitted highlight the need for the involvement and rapid responses of individuals and communities in the prevention and control of the pandemic.140 It is clear that efforts have been made to involve patients and accompanying persons in order to achieve safe care, and this has been seen as one of the factors with the greatest positive impact on the patient’s experience. This positive experience, in turn, results in increased patient safety and improves their perception of quality in healthcare.141 142
To ensure safe patient care during the pandemic, institutions and frontline professionals needed to quickly adjust to the sudden increase in the number of critically ill patients and the shortage of skilled labour.143 At the beginning of the pandemic, there was also a shortage of PPE due to high demand, and administrative improvements were highlighted as essential to ensure the supply, distribution and training of health professionals and patients.24 25 39 101 108 131 A study carried out in Ecuador, Brazil and Colombia identified serious deficiencies in PPE, insufficient training in relation to the prevention of infections and use of PPE and a lack of isolation protocols for health professionals.144
To meet the demand, health professionals endured unprecedented pressure. In addition to undergoing long working hours and many hours of training, they faced the fear of becoming infected and/or bringing infection to their families, concern about their own skills and patient safety and the loss of professional colleagues.143 145 146
Currently, even with demand regulated and vaccination reaching all continents, the efficient management of the pandemic is still essential. To face similar contexts, hospitals need to devise strategies to increase their capacity for care and, quickly adapt human resources.147
The recommendations presented in this review summarise the best practices produced up until now. The thorough search made by the review, involving scientific databases, grey literature and official documents from reference health institutions, together with the rigorously applied method, corroborate the reliability of the data presented and the applicability of the recommendations in the intrahospital context, in the COVID-19 pandemic and in any respiratory epidemic. The review process was performed independently by peer reviewers, and the research team was trained to conduct scoping reviews and developed a prior research protocol.
The primary weakness of this review is that most studies are those of the expert consensus type. Nevertheless, as the context is that of a pandemic, both clinical practice guidelines and expert opinion are the best available evidence. Many studies describing practices and procedures emerged in the research but were excluded because the research question sought recommendations for patient safety. As the qualitative grouping of the data analysis is a subjective process, there may have been some suppression of information. The predominance of documents of the expert consensus type, analysed in this scoping review, demonstrates the emerging nature of the issue as it is essential to act urgently in order to control the COVID-19 pandemic.148 This scoping review is the initial step in mapping out recommendations for hospitalised patient safety, and there is a need for further research and an assessment of the effectiveness of these recommendations.
Given the possibility that we will be living together with SARS-CoV-2 and its variants, there is a need to carry out risk management, maintaining the recommendations of safe practices both for reducing transmission to patients and for the protection of health professionals. In this sense, the recommendations mapped in this scoping review serve as a basis for planning and implementing good practices to ensure safe hospital care, during and after COVID-19.
Conclusion
Forty-six recommendations for the provision of safe care to hospitalised patients, with regard to the scenario of the current pandemic have been described in this scoping review. Strategies for change in the organisation of health services to assist infected people have been highlighted, mainly focusing on the proper use of PPE and airway management, practices that have been consolidated throughout the pandemic and which will be reflected in other possible similar future situations. The engagement of everyone involved in the care of hospitalised patients is essential to consolidate the mapped recommendations and provide dignified, safe and quality care.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We would like to thank Juliana Takahashi, member of the core staff at The Brazilian Centre for Evidence-based Healthcare, for her assistance and feedback with the development of the search strategy for the scoping review.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Marisantini, @RafaelPimenteel
Contributors MSM oversaw the development of all stages of the study and is responsible for the overall content as guarantor. MSM, DCdAL, RRdSP, JMO, LTdCNM, RCM, MSdSS and MJdS contributed to all aspects of the study throughout the research cycle. MJdS critically reviewed the final version to be approved. MSM and DCdAL developed the first draft of the manuscript and all authors reviewed and approved the final manuscript.
Funding This work was supported by Pro-Rectory of Research, University of São Paulo, as part of the Programme of Support for Recently Admitted Lecturers, Ordinance PRP no. 775/2020.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.