Article Text

Abstract
Objectives To improve continence care in the Netherlands, a new framework has been developed in which a shift has been made from incontinence severity as the sole criterion for selecting incontinence products to a focus on patient need for daily life activities. The impact of the framework on daily care has not been assessed. We aimed to compare treatment effectiveness and costs between participants who did and did not undergo re-evaluation according to the new framework.
Design Cohort study
Setting Twelve pharmacies in the Netherlands
Participants Existing users of absorbent incontinence materials for urinary incontinence.
Interventions Participants were offered the option to have their incontinence products re-evaluated within the new framework at their pharmacy.
Primary and secondary outcome measures Effectiveness and cost outcomes were assessed at 3 and 6 months through questionnaires. These questionnaires included the International Consultation on Incontinence Questionnaire (ICIQ) Lower Urinary Tract Symptoms Quality of Life Module, ICIQ Urinary Incontinence Short Form, ICIQ Absorbent Pads, questions about satisfaction and the iPCQ and iMCQ.
Results 303 users consented and 279 completed the baseline questionnaire. Of these participants, 72 agreed to a re-evaluation of their incontinence materials. There was a small improvement at 3 months in the re-evaluation group compared with the other group on most outcomes. However, these improvements were not clinically relevant. Moreover, these differences did not change much from 3 to 6 months. Small differences were also observed in the changes in costs, but with very wide CIs on both sides of zero (€99.38; 95% CI −633.48 to 832.23).
Conclusions The current study showed no clinically relevant effect of a newly implemented framework for selecting incontinence materials in pharmacies when compared with an existing method. Given that the study also showed no differences in effectiveness and costs, introducing the new framework in pharmacies may not lead to better incontinence care.
- Urinary incontinences
- Health policy
- Health economics
Data availability statement
Data are available upon reasonable request. https://dataverse.nl/dataset.xhtml?persistentId=doi:10.34894/OVPONP.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
We gathered information on a range of outcomes that are patient and clinically important and that can be used by policymakers.
As the study was performed in prevalent cases, we cannot draw conclusions regarding the effectiveness of the new framework in incident cases.
The use of an observational study design may have introduced bias because participants who opted for re-evaluation had more symptoms and were less satisfied with their current materials.
Introduction
About 28% of women and 9% of men aged 60 years or over report involuntary urine loss at least two times a month,1 which can affect quality of life (QoL) and lead to social isolation and problems with intimacy.2 3 A considerable proportion of people in this group use absorbent incontinence products, which in the Netherlands, are reimbursed if prescribed by a physician for incontinence that has a large impact on life and persists for more than 2 months. In 2020, over 400 000 people used reimbursed products, bringing substantial costs of 100–150 million euros per year.4 Prescriptions by doctors are usually non-specific, giving pharmacies or online providers the freedom to select products based on patient need and applicable reimbursement policies. Most health insurers reimburse a standard amount per day depending on the severity of incontinence.
To improve continence care in the Netherlands, the Ministry of Health, Welfare and Sport initiated the development of a new framework in 2018 with support from the National Health Care Institute and input from patient advocates, healthcare professionals, suppliers and insurers.5 Central to this framework, there has been a shift in focus from incontinence severity as the sole criterion for selecting incontinence products to a focus on patient need for daily life activities. Highly specific goals regarding function must also be formulated before selecting products. All relevant stakeholders engaged in developing the framework, and its use is now considered obligatory for all providers of continence products. Nevertheless, its impact on daily care has not been assessed.
We aimed to compare treatment effectiveness and costs between participants who did and did not undergo re-evaluation according to the new framework, including a subgroup analysis comparing re-evaluated participants who did and did not require a change in materials.
Methods
Study design
Twelve pharmacies participated in this cohort study of existing absorbent incontinence product users and identified eligible patients. To facilitate the inclusion of incontinence product users, we excluded new users of continence products (incident cases); instead, we only applied the framework to existing users of incontinence products and re-evaluated their products. This made it possible to invite all users at a single point. People with urinary incontinence, aged 18 years or older, and having received incontinence products for more than 3 months were eligible for the study, but we excluded users with terminal illnesses.
Eligible patients received an invitation letter for the study. Non-responders then received a second invitation after 3–5 months that included an opt-out questionnaire in which they could indicate that they did not want to participate in the cohort study and select a reason from a prespecified list. The study was conducted according to the principles of the Declaration of Helsinki. All participants gave written informed consent. The study was approved by the Medical Ethical Committee of the University Medical Center Groningen (no. 2018/551).
Intervention
In each participating pharmacy, one or more employees who were actively involved and experienced in continence care were invited for training to familiarise them with the new framework. The framework has seven steps: (1) identify the problem, (2) formulate care demand, (3) draft care plan, (4) select, try and decide, (5) deliver and instruct, (6) use and (7) evaluate. During re-evaluation, we used a standard form that was developed alongside the new framework.
After providing consent, participants completed a baseline questionnaire (paper or digital, depending on their preference), in which they were offered the option to have their incontinence products re-evaluated within the new framework at their pharmacy. Those who reported an interest were invited by appointment to visit the pharmacy for re-evaluation.
Outcome measures
At baseline, we digitally collected information about demographics and comorbidity. Pharmacy employees collected information about the re-evaluation on a case report form. This included data on whether the existing product was in line with the new framework, together with any changes that had been made following the re-evaluation. We also assessed patient-reported outcomes at baseline by questionnaire and collected relevant information needed to assess effectiveness and costs. The patient-reported outcome questionnaires and the collection of effectiveness and costs data were repeated after 3 and 6 months. Specifically, the following instruments were used to assess outcomes in this study.
The International Consultation on Incontinence Questionnaire (ICIQ) Lower Urinary Tract Symptoms Quality of Life Module (ICIQ-LUTSqol) was used to measure QoL.6 This questionnaire includes 20 questions, giving an overall score of 19–76, with higher values indicating increased impact on QoL. The approximate minimum clinically important difference for the ICIQ-LUTSqol in women with stress incontinence has been reported to be 3.7 points in one study and 5–6 points in another.7 8
The ICIQ Urinary Incontinence Short Form (ICIQ-UI-SF) was used to assess the frequency, severity and impact on QoL, of urinary incontinence.9 The ICIQ-UI-SF consists of four questions and gives a total score of 0–21, with lower scores indicating less severe incontinence. The minimum clinically important difference for the ICIQ-UI-SF in women with stress incontinence has been reported to be around 2.5 points in one study and around 4 points in another.7 8
The ICIQ Absorbent Pads (ICIQ-PadPROM) was linguistically validated in Dutch and used to assess the treatment effect of absorbent incontinence products on QoL.10 It has 26 questions and 4 subdomains: pad design and physical effect (seven questions, score 0–31), psychological effects (four questions, score 0–16), social effects (three questions, score 0–12) and pad leakage and burden of pad use (three questions, score 0–12). A lower score indicates a better QoL.
Satisfaction with incontinence care and incontinence products were each measured with three specifically developed questions answered with 5-point Likert scales ranging from very unsatisfied (0 points) to very satisfied (4 points) and giving total scores ranging from 0 to 12 points (online supplemental file 1).
Supplemental material
Information on incontinence-related healthcare use over the last 3 months was collected using relevant questions from the iMTA Medical Consumption Questionnaire, and information about productivity loss due to incontinence in the last 4 weeks was collected using the iMTA Productivity Cost Questionnaire.11 12 Information about all urinary incontinence products and incontinence-related medication provided from 3 months before baseline to 6 months after baseline was obtained from the registries of each pharmacy.
Statistical analysis
All analyses were performed using IBM SPSS V.26.0 (IBM, Armonk, New York). Participants who underwent re-evaluation according to the new framework were compared with participants who did not have a re-evaluation. We also performed subgroup analysis among re-evaluated participants to compare those who did and did not require a change in materials, thereby mimicking an intention-to-treat analysis. Because of the clustered data, a mixed model analysis was performed on the change scores for outcome variables when assessing differences between groups. We included intervention, time and the Intervention×Time interaction as fixed effects. A random intercept at the individual level was included in all analyses and we checked whether a random intercept at the pharmacy level improved model fit, using the Akaike Information Criterion. These analyses were adjusted for age, sex and educational level to control for potential confounding.
Cost analyses
Cost analyses were performed using a societal perspective according to the guidelines for economic evaluations of the Dutch National Health Care Institute.13 Data on the amount of care and productivity loss from the iPCQ and iMCQ were multiplied with prices in the guideline to obtain the costs. The prices of incontinence products were obtained from one of the participating pharmacies and the costs for medication were taken from the pharmacotherapeutic information website of the Dutch National Health Care Institute.14 An overview of the unit costs is presented in online supplemental file 2. Costs are reported in euros based on the 2019 prices and calculated for 3 months prior to baseline and 3 months prior to last follow-up. Differences in change of costs over time between groups were calculated from baseline to compare participants who did and did not undergo re-evaluation, and a subgroup analysis was repeated among re-evaluated participants to compare those who did and did not require a change in materials. Costs were bootstrapped 5000 times to obtain 95% CIs based on the 2.5th and 97.5th centiles.
Supplemental material
To assess the generalisability of the results, we compared study participants to all invited users by sex, age and continence product costs.
Patient and public involvement statement
A patient representative (Bekkenbodem4All) was involved in the conception and design of the study and the interpretation of the results.
Results
Descriptive statistics
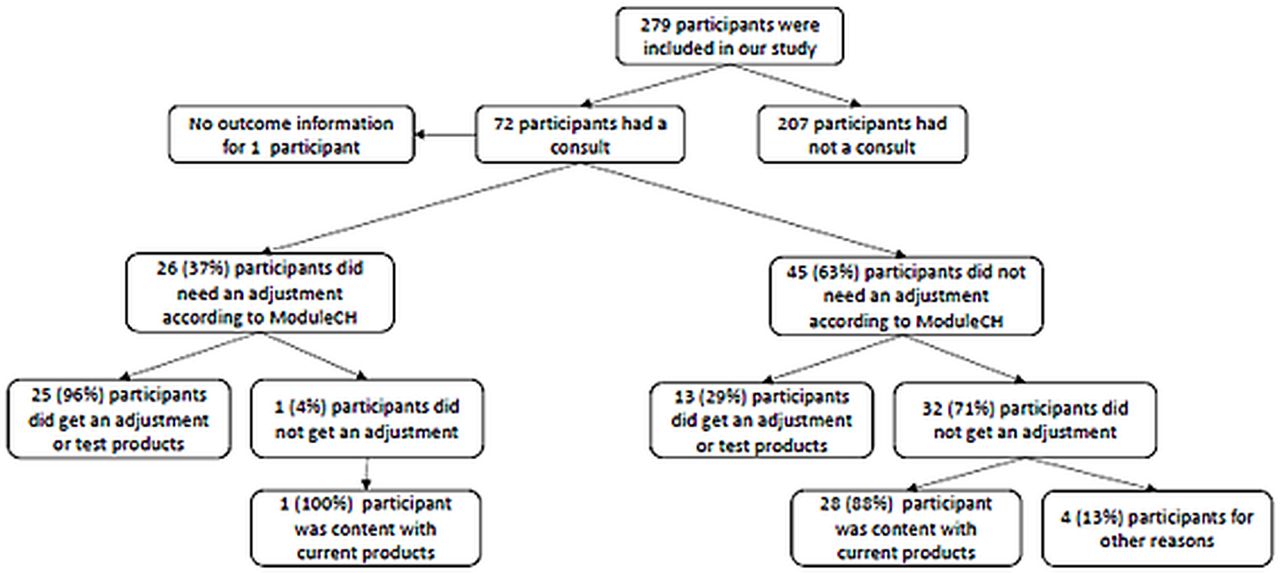
The 12 pharmacies invited 1907 users of incontinence products to participate (range 71–270 users per pharmacy). Of these, 303 (15.9%) users consented and 279 completed the baseline questionnaire (figure 1). Of those invited but not consenting, the non-responders, 404 (21.2%) completed the opt-out questionnaire. The most cited reasons for not participating were satisfaction with current products (71%), lack of interest in the research (35%) and lack of willingness to complete questions on incontinence (32%). About 25% selected ‘other reasons’ and most selected old age or the presence of an age-related disease.
{kind=link}
Flowchart of study participation.
Of the 12 participating pharmacies, 11 provided information on incontinence product users invited to the study (n=1746). Four of these provided data on incontinence products, but not on age or sex, so they were only included in the cost calculations. Based on the relevant data, 79% of the sample was women, the mean age was 75.6±12.5 years and the mean cost of incontinence product use every 3 months was €128.10 (95% CI €121.95 to €134.03).
Participant characteristics are shown in table 1. Of the 279 who completed baseline questionnaires, 72 (25.8%) agreed to a re-evaluation of their incontinence materials. Those who underwent re-evaluation were older, had lower educational levels, more often lived alone than with others, had more severe symptoms with a higher impact on their lives and were less satisfied with the existing continence care compared with those who did not undergo re-evaluation.
Descriptive characteristics of participants
Outcomes
After 3 and 6 months, the follow-up questionnaires were completed by 248 (88.9%) and 231 (82.8%) participants, respectively. Pharmacies could not provide information about incontinence products or related medication in three cases. No outcome data were available for 1 of the 72 participants who underwent re-evaluation. Of the remaining 71 participants, 26 required a change and 45 did not require a change based on the new framework. However, one participant who required a change was content with the current material and did not want to make the recommended change.
There was a small improvement at 3 months in the re-evaluation group compared with the other group on most outcomes (table 2). However, improvement did not approach the minimum clinically important difference scores of the ICIQ-LUTSqol or ICIQ-UI-SF and was small compared with the range of the scales for other outcomes. Moreover, these differences did not change much from 3 to 6 months.
Effect of re-evaluation on disease-specific outcomes and satisfaction
Subgroup analysis in participants with re-evaluation showed that those who needed a change in materials (n=26) experienced no clinically important differences in outcomes than those who did not need a change (n=45, (online supplemental file 3).
Supplemental material
Costs
We also observed small differences in both the change in total costs and the changes for all cost categories separately that favoured users who underwent re-evaluation, but with very wide CIs on both sides of zero (€99.38; 95% CI −633.48 to 832.23) (table 3).
Mean costs of the two evaluation groups per cost unit and time point
Difference in total cost changes (€606.23; 95% CI -€2062.85 to €772.60) and incontinence material costs (€6.44; 95% CI -€56.65 to €45.98) were seen in favour of participants who did not need to change material, but again, this was with wide CIs.
Discussion
We found that the new framework for incontinence products had no clinically relevant effect on the QoL, severity or satisfaction of users compared with the existing method of selecting materials. However, although there was no clear evidence, the new framework may have affected costs. Research on the effectiveness and cost-effectiveness of methods for selecting incontinence materials in the general population is scarce. Fader et al15 showed that the optimal absorbent product design varies by incontinence severity and sex.15 There is also large variability in preference, and cost-effective management requires users to be able to choose combinations of designs for different circumstances. A trial in the Netherlands showed that it was cost-effective to employ a continence nurse in general practice,16 using an intervention based on a service specification for incontinence care developed by systematic review and expert consensus.17 A key recommendations of that service specification was to take user and usage factors into account, which are both included in the new framework evaluated in the current study.
We found no evidence that the new framework affected either patient-related outcomes or costs. Given that the framework has already been put in place as the new standard, our findings should be used to improve its content and implementation. Our findings suggest that the new framework does not go far enough to produce clinically important changes. One reason may be that pharmacy employees still had to work within the constraints of health insurers, where the severity of incontinence is key for reimbursement. In interviews after study completion, pharmacy employees indicated that (1) although they supported the idea of the framework, they were unsure whether reimbursement would be possible for all patients and (2) they still had to use the old system alongside the new framework to comply with reimbursement regulations (unpublished data). Including activities of daily living in reimbursement regulations and reducing the administrative burden may increase the impact of the framework. Pharmacy employees also noted that the new framework is not dramatically different from the existing procedure for material selection. This too could have led to the failure to detect a clinically important change.
Regarding the costs, we used a societal perspective that included productivity losses, in accordance with guidelines. However, participants reported no productivity losses, probably because most were older than 65 years and only a minority were not in retirement.
Although the new framework was developed to improve incontinence care, our findings suggest that users of incontinence materials are already quite satisfied with current care, as reflected in the average baseline Likert score of 4 (satisfied) for satisfaction. Being satisfied was also the most cited reason for not participating in the study (71%). This may be another reason for the failure to detect a clinically relevant effect, with most participants having little to no room for improvement.
A limitation of our study is that it was performed among existing users of incontinence materials and excluded incident cases. It is possible that the new framework will have a greater impact on new users or that pharmacy employees and participants did the re-evaluation with the current materials in mind, which could have led to them being more conservative when changing materials. Also, long-term users may have ended up with suitable materials through trial and error, and it may be that the framework will help this to occur sooner. Nevertheless, we cannot draw conclusions regarding the effectiveness of the new framework in incident cases based on the current study.
The use of an observational study design may also have introduced bias. The main reason for choosing this design was that the new framework was about to be introduced as the new standard of care and a randomised controlled trial could not be started in time because allocation to the control condition (existing method of selecting materials) was not possible. Therefore, selection bias may have arisen because participants were free to choose their intervention. In the present study, participants who opted for re-evaluation had more symptoms and were less satisfied with their current materials. We hypothesise that this did not affect the study conclusions because the intervention likely had an even smaller effect in participants with fewer eports and higher satisfaction. We also found that participants who choose the intervention more often lived alone, which may reflect a need for social interaction (eg, with a caregiver). This could generate higher satisfaction at follow-up; but, given that we found no clinically relevant effect of the intervention, this does not appear to have had a major impact on the outcomes. However, the observational study design does not allow to make causal claims.
We encountered a low response rate, with only 16% of invitees participating in the full study. To provide insight into the reasons for non-participation, the opt-out questionnaire send to the non-responders was only returned by 21% of people. In this opt-out survey, acquiescence bias could have impacted the outcomes, with a high percentage of respondents claiming to be satisfied with the current care. To improve generalisability, we compared the characteristics of study participants against all those who were invited. This revealed that both groups were broadly comparable by age and sex, but that incontinence material costs were somewhat lower for participants, suggesting that they had less severe incontinence or that they received less absorbent materials. However, it is possible that those who did not participate and those who did participate differ on other characteristics, which might have an impact on generalisability. Another issue is that since completing this study there has been a trend for insurers to move reimbursed continence care from local pharmacies to nationwide online suppliers, which may limit the generalisability of our results to current practice.
Conclusion
The current study showed no clinically relevant effect of a newly implemented framework for selecting absorbent incontinence materials in pharmacies when compared with an existing method. Given that the study also showed no difference in effectiveness and costs, introducing the new framework in pharmacies may not lead to better incontinence care. Future research should consider the experiences of incontinence material users through qualitative research to add further information on how to improve the framework.
Data availability statement
Data are available upon reasonable request. https://dataverse.nl/dataset.xhtml?persistentId=doi:10.34894/OVPONP.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but Metc UMCG Groningen (2018/551) exempted this study. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank the participants for their time and effort and Dr Robert Sykes (www.doctored.org.uk) for providing editorial assistance. We thank Francisca Somvorde, Rianne Wijbenga and Deborah de Boer for their help with the logistics of the study and data collection.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Marco_Blanker
Contributors Study design: MCS, HvdW, BB, AGGAM, JD, KV, MHB. Acquisition of data: MCS, HvdW, MHB. Analysis and interpretation of data: MCS, HvdW, MdB, KV, MHB. Drafting of the manuscript: MCS, HvdW, MHB. Revision and approval of the final version of the manuscript to be published: all authors. Guarantor: MHB.
Funding This work was supported by a grant from ZonMw, the Dutch OrganizationOrganisation for Health Research and Development (project number: 853001105).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.