Article Text

Abstract
Introduction Over 70% of the intensive care unit (ICU) survivors suffer from long-lasting physical, mental and cognitive problems after hospital discharge. Post-ICU care is recommended by international guidelines, but evidence for cost-effectiveness lacks. The aim of this study is to evaluate the clinical effectiveness and cost-effectiveness of structured, multidisciplinary and personalised post-ICU care versus usual care on physical and psychological functioning and health-related quality of life (HRQoL) of ICU survivors, 1- and 2-year post-ICU discharge.
Methods and analysis The MONITOR-IC post-ICU care study (MiCare study) is a multicentre stepped-wedge randomised controlled trial conducted in five hospitals. Adult patients at high risk for critical illness-associated morbidity post-ICU will be selected and receive post-ICU care, including an invitation to the post-ICU clinic 3 months after ICU discharge. A personalised long-term recovery plan tailored to patients’ reported outcome measures will be made. 770 (intervention) and 1480 (control) patients will be included. Outcomes are 1- and 2-year HRQoL (EuroQol Instrument (EQ-5D-5L)), physical (fatigue and new physical problems), mental (anxiety, depression and post-traumatic stress disorder), and cognitive symptoms and cost-effectiveness. Medical data will be retrieved from patient records and cost data from health insurance companies.
Ethics and dissemination Due to the lack of evidence, Dutch healthcare insurers do not reimburse post-ICU care. Therefore, evaluation of cost-effectiveness and integration in guidelines supports the evidence. Participation of several societies for physicians, nurses, paramedics, and patients and relatives in the project team increases the support for implementation of the intervention in clinical practice. Patients and relatives will be informed by the patient associations, hospitals and professional associations. Informing healthcare insurers about this project’s results is important for the consideration for inclusion of post-ICU care in Dutch standard health insurance. The study is approved by the Radboud University Medical Centre research ethics committee (2021-13125).
Trial registration number NCT05066984.
- adult intensive and critical care
- intensive and critical care
- protocols and guidelines
- primary care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The strength of this study is the multicentre stepped-wedge cluster randomised controlled trial in five hospitals.
Patients will be followed up for 2 years.
Post-ICU care is tailored to the health status of individual patients, based on patient-reported outcomes at intensive care unit (ICU) admission and at 3 months post-ICU.
Involvement of all relevant stakeholders in the codesign of the study and intervention increases the risk for carry-over effect between control and intervention group.
Implementation of a complex intervention involving several stakeholders, reaching high compliance to the study protocol is challenging.
Introduction
Annually, over 68 000 (90%) intensive care unit (ICU) patients survive in the Netherlands.1 Many ICU survivors experience long-lasting health problems, collectively labelled as post-intensive care syndrome (PICS) and described as new or worsening impairments in physical, mental and cognitive health arising after critical illness and persist beyond acute care hospitalisation.2 Data from our multicentre long-term follow-up cohort study MONITOR-IC3 showed that 50% of the ICU survivors suffer from new physical (eg, muscle weakness, lung problems), mental (eg, depression) and cognitive problems (eg, memory problems), impacting work and daily functioning as long-lasting consequences of critical illness and ICU treatment.4
Several interventions exist to prevent or reduce post-ICU problems.5 Post-ICU care is recommended by international guidelines6 but are not yet evaluated thoroughly. The number of studies is limited and evidence that post-ICU care has a positive effect on outcomes is thin.7 Post-ICU care focusing on physical therapy was associated with significantly less depression symptoms and improved mental health-related quality of life (HRQoL) scores.8 Early physical therapy and tailoring the exercise programme were most beneficial resulted in a significantly improved physical capacity, and physical and mental components of HRQoL.8 Furthermore, psychological interventions were associated with significantly less post-traumatic stress disorder (PTSD) symptoms.8 Patients were highly satisfied with the post-ICU follow-up care.
The quality of the studies, including the randomised trials, was, however, low, and sample sizes were rather small. Relevantly, none of the studies included patients with a high-risk for post-ICU problems, diluting possible effects of interventions. Furthermore, most patients were included based on the duration of mechanical ventilation and length of ICU stay. However, prediction modelling studies showed that pre-ICU health (mental and physical) status and comorbidities are the most important predictors for quality of life (QoL) after ICU admission.9
Several Dutch ICUs provide some kind of post-ICU care.5 Because of the lack of evidence, these current post-ICU clinics are pragmatically set up, without focusing on patients with a high risk for long-term sequelae, who will likely benefit the most of post-ICU care.8 Also, although some of the studies tailored their intervention, none of the studies used patient-reported outcome measures (PROMs) to tailor the post-ICU follow-up care on patients’ health problems and needs. There is more to be gained when focusing on patients with an increased risk for post-ICU problems and to measure patient-reported problems to start early and personalised care in the recovery period after ICU admission.
Despite there is a lack of evidence, post-ICU care should be further coordinated by primary care since they play a pivotal role in the support and care of ICU survivors to prevent further deterioration. The general practitioner’s (GP) role is unclear although he or she has the best overview of patients and he or she is the first point of contact after hospital discharge. This may result in fragmented and delayed patient care, worsening of health problems and higher healthcare costs and societal costs.5 Due to the COVID-19 pandemic, health professionals are more aware that critically ill patients need follow-up care, for not only their underlying disease but also due to problems after ICU admission. Therefore, several forms of follow-up appeared, despite no evidence of cost-effectiveness.
To prevent and treat health problems after ICU discharge, the MONITOR-IC follow-up care study, further mentioned as MiCare study, was set up to develop and evaluate structured, multidisciplinary and personalised post-ICU care initiated by ICU clinicians and further transferred to GPs.
Study objectives
This study has the following objectives: to evaluate the (1) clinical effectiveness and (2) cost-effectiveness of structured, multidisciplinary and personalised post-ICU care versus usual care on physical and psychological outcomes, and HRQoL of ICU survivors 1- and 2-year post-ICU.
Methods and analysis
Study design and setting
The MiCare study is a multicentre stepped-wedge cluster randomised controlled trial in ICUs of five (academic and non-academic) hospitals (figure 1). Every 4 months, an ICU starts with the intervention period, after a training and implementation period of 2 months. Until entering the intervention period, ICUs start with control data collection, added with historical control patients. The order in which ICUs enter the intervention period will be randomised. Randomisation on patient level results in contamination between control and intervention group; therefore, a cluster randomised (stepped-wedge) design is the most suitable option. The study started in February 2022 and the planned end date is November 2025.
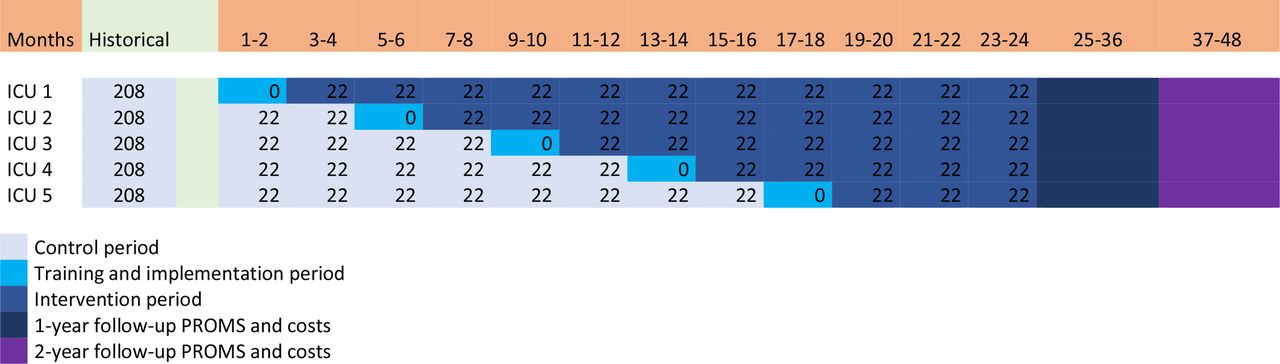
Number of patients per ICU per time frame. ICU, intensive care unit; PROMs, patient reported outcome measures.
This project is part of the ongoing, multicentre cohort study, MONITOR-IC, in which long-term outcomes of ICU survivors are studied up to 5 years after ICU admission. The MONITOR-IC database already includes PROMs data of thousands of ICU patients, which serve as historical control data.
Study population and eligible criteria
Adult ICU patients at high risk of critical illness-associated morbidity post-ICU. Prediction models for risk determination of critical illness-associated morbidity post-ICU will be developed based on historical PROM data from thousands of ICU patients from the MONITOR-IC database and patients’ medical health record. The patient’s risk for physical, mental or cognitive problems 3 months post-ICU will be determined. A threshold score for ‘high risk’ will be determined based on the historical data and the prediction model’s performance. Risk scores higher than this threshold will be referred to as high risk for critical illness-associated morbidity. Candidate predictors are several variables about pre-ICU health status and data from the first 24 hours in the ICU. Patients experiencing for example complications during ICU stay (eg, delirium or complication after surgery) which may lead to the development of PICS can be included based on clinicians’ judgement.
Sample size calculation
Importantly, outcomes within ICUs are not independent, but correlated. Therefore, this feature must be incorporated into power calculations and the trial analysis. Other assumptions for the sample size calculation are as follows:
Five participating ICUs.
A mean effect size of 0.074 (minimal clinical important difference) increase in the primary outcome measure (EQ-5D) might be expected from the literature.10
An intraclass correlation (ICC) of 0.035 was calculated with historical data of participating ICUs.11
Based on the availability of five ICUs (clusters), measuring 11 patients per ICU/per month, a total of 770 intervention and 440 active control patients, added with 1040 historical control patients, are needed, resulting in a 87% power to detect an effect of 0.074 (minimal clinical important difference) in EQ-5D (alpha=0.05, ICC=0.035, SD=0.26) and >87% power to detect an effect of 1.21 in the Hospital Anxiety and Depression Scale (HADS)12 (alpha=0.05, ICC=0.035, SD=3.89).8 10
In total, there are 12 periods of 2 months with five ICUs resulting in 60 blocks, of which 5 blocks are implementation blocks (figure 1). Data collected during implementation blocks will not be used for analysis. The first ICU starts in months 1–2 with the implementation and from month 3 till 24 this ICU is in the intervention period. The last randomised ICU starts with the implementation in months 17–18. From months 1–16, patients in this centre are control patients and from months 19–24 intervention patients will be included. In between, the other three centres will be randomised and transferred to the implementation and subsequently to the intervention period. In total, there will be 20 blocks of ICU controls (20×22=440 patients) added with 16 months (November 2018–February 2020) of historical data consisting 26 patients per 2 months per ICU (1040 historical controls; in total 1480 controls). There will be 35 blocks of ICU intervention patients (35×22=770).
Study intervention
This structured, multidisciplinary and personalised post-ICU care includes a short-term recovery plan for patients at high risk for adverse outcomes post-ICU with focus on physical recovery and if necessary early psychological or cognitive support. Furthermore, patients at high risk will be invited to the post-ICU clinic 3 months postdischarge. Here, the ICU follow-up team sets up a personalised long-term recovery plan in close cooperation with other specialists (eg, pulmonologist or geriatrician) covering the physical, mental and cognitive domains and HRQoL based on patients’ outcomes of prefilled questionnaires and patients’ needs and preferences. This treatment plan includes referrals to specialised healthcare providers (eg, rehabilitation physician, psychologist, dietician). Furthermore, ICU clinicians are sensitive for possible mental problems in relatives. There is an extensive handover to the GP for their coordinating role regarding follow-up care. The intervention protocol is summarised in online supplemental file 1.
Supplemental material
Data collection
Patients, or their relatives in case patients are not able to fill in questionnaires themselves, will be approached to complete a self-administered online questionnaire at or soon after ICU admission, after 3 months, 12 months and 24 months as part of the MONITOR-IC study (figure 2). In case patients cannot perform the questionnaire online, this will be carried out by phone. Patients’ health status prior to the ICU admission, baseline questionnaire, will be requested when the patients are asked for informed consent. This could be preoperatively for the planned admissions or shortly after acute admission to the ICU. The latter, rating is then done in retrospect. Prediction models are developed to select high-risk patients. Hereby, data from the baseline questionnaire will be used as predictors in the model. Patients discharged from ICU/hospital direct to a nursing home or to a medical or geriatric rehabilitation clinic, or patients discharged for palliative care are not eligible for inclusion. Patients with COVID-19 are eligible for inclusion if they do not participate to another rehabilitation programme simultaneously. Included patients who die in the follow-up period will be documented as ‘lost to follow-up’. Patients who will be transferred to another hospital can only be followed up if this hospital is also in the intervention period of this study. If not, patients will be marked as ‘loss to follow-up’. To study the adherence to the intervention components, key parts of the intervention protocol will be registered as completed or not for every study participant.

{kind=link}
{kind=link}
Timeline of patient inclusion and data collection. ER, emergency room; OR, operating room.
Data sources
PROM data of the participant will be collected in the MONITOR-IC database. Demographic and medical data are extracted from the National Intensive Care Evaluation1 registry in which ICU physicians register patient variables, including admission diagnosis, chronic diagnoses, admission type (classified as elective surgical, acute surgical or medical), planned admission, severity of illness score expressed in Acute Physiology and Chronic Health Evaluation IV score, mechanical ventilation days, and ICU and hospital length of stay (LOS).
Healthcare use and related costs, covered by the Dutch healthcare insurance, will be retrieved from Vektis, a Dutch organisation which collects and manages health insurance claimed data of all health insurance companies in the Netherlands.13
Outcome measures
Primary outcome is HRQoL measured by the EuroQol instrument (EQ-5D-5L),14 and anxiety and depression are measured by the HADS at 1 year after ICU discharge. The EQ-5D-5L is a validated instrument and applicable in different countries and languages and can be used for the calculation of quality-adjusted survival, an important measure of health effects for cost-effectiveness assessments.15 The HADS is the most often used questionnaire to measure symptoms of anxiety and depression in ICU survivors.16
Secondary outcomes are fatigue measured by the Checklist Individual Strength (CIS),17 frailty measured by the Clinical Frailty Scale (CFS),18 new physical problems, PTSD by the Impact of Event Scale—Revised (IES-R), cognitive functioning by the 14-item Cognitive Failure Questionnaire, social consequences, return to work and cost-effectiveness at 1 and 2 years. The CIS is used by ICU patients before.4 19 The CFS is short, simple and reliable to measure frailty. The CFS makes it possible to predict outcomes more effectively.20 The IES-R is a standardised measure of PTSD symptoms.21
Data analysis
Data will be analysed according to the ‘intention-to-treat’ principle, but in secondary analyses we will also carry out per-protocol analyses. A linear mixed-effects model analysis with ICU as random effect will account for the correlation of patients within cluster periods (2-month period within ICU), and fixed effects for time and intervention programme will estimate the time trend and intervention effect, respectively. Furthermore, subanalysis will be performed for the participating hospitals and patient selection procedure. Missing values will be handled according to manuals of questionnaires, or imputed or interpolated, depending on random or not-random missing. ‘Cost per QALY gained’ will be established by comparing patients in the intervention with the control group. Average savings per patient will be extrapolated to population level using a budget-holders perspective and medium-term time frame.
Patient and public involvement
The national foundation Family and Patient Centered Intensive Care (FCIC) and patient organisation IC Connect for ICU survivors and their family members were involved in the development of the research question and design of the study.19 Members of the FCIC were involved in the development and implementation of the intervention. Also, members of the FCIC will be involved in the analysis, interpretation and implementation of the study results. Study results will be communicated to all study participants and other ICU patients via layman information in newsletters and the website of the patient organisation.
Ethics and dissemination
Due to the lack of evidence, Dutch healthcare insurers do not reimburse post-ICU care. Therefore, evaluation of cost-effectiveness and integration in guidelines supports the evidence. Participation of several societies for physicians, nurses, paramedics, and patients and relatives in the project team increases the support for the implementation of the intervention in clinical practice. Patients and relatives will be informed by the patient associations, hospitals and professional associations. Informing healthcare insurers about this project’s results is important for consideration for inclusion of post-ICU care in Dutch standard health insurance. The study will be conducted complying with the Dutch Personal Data Protection Act. The patient information letter is available as online supplemental file 2, and the patient and legal representative informed consent form as, respectively, online supplemental files 3 and 4.
Supplemental material
Supplemental material
Supplemental material
Relevance of findings
There are no comparable RCTs conducted, planned or ongoing regarding the cost-effectiveness of structured, personalised, multidisciplinary post-ICU care for all types of ICU. Post-ICU clinics are recommended in international guidelines, but not yet evaluated.6 This lack of evidence is an important known barrier for healthcare professionals to provide post-ICU care.5 Furthermore, post-ICU care cost-effectiveness has never been evaluated in randomised studies5 22; therefore, healthcare insurers do not reimburse this care in the Netherlands. If structured, multidisciplinary and personalised post-ICU care is proven effective, this can facilitate further implementation of this approach in healthcare for future patients in need of care. Therefore, generating evidence with this study and integration of the results in guidelines is important.
Post-ICU care should be organised as multidisciplinary follow-up care since this improves outcome, and monodisciplinary (nurse-led) follow-up care did not.23 Patients with high risk for post-ICU problems will be invited to prevent dilutional effects, and regarding cost-effectiveness follow-up should be 2 years, since most healthcare costs are in the first year and costs benefit will therefore be found in the second year.24 Post-ICU care should be focused on problems that patients experience, so personalised care is important, especially since tailoring the intervention has been shown to be effective.8 Despite there is a lack of evidence, post-ICU care should be further coordinated by the GP, since they play a pivotal role in the support and care of ICU survivors to prevent further deterioration. This is confirmed by a member poll among ICU survivors and relatives by the ICU patient and family association FCIC (including patient organisation IC Connect) in September 2020 (draft results of member poll, available on request by FCIC).
The strengths of this study are the thorough and comprehensive methodological approach, involvement of the patient organisation in developing the intervention, inclusion of a large number of patients and 2-year follow-up time. Furthermore, in this study PROM and health insurance cost data will be linked on a patient level creating patient-specific results. This project is embedded in an existing ICU research infrastructure with strong collaboration with all relevant stakeholders (patients, (ICU) physicians, GPs, nurses, paramedics, etc).
There are also some limitations that need to be addressed. Involvement of all stakeholders in the design of the study and intervention increases the risk for carry-over effect between control and intervention group. Therefore, a cluster randomised (stepped-wedge) design is considered as the most suitable option. Also, the current attention for follow-up care for former ICU patients with COVID-19 could lead to some kind of contamination of the control group.25 However, baseline questions are asked retrospectively and short after ICU admission to reduce recall bias. Furthermore, a large amount of control data is already collected and dated prior to the COVID-19 pandemic. Moreover, most recent follow-up care studies include only patients with COVID-19, while the urgency to generate evidence for follow-up care for all former ICU patients is paramount. Altogether, the attention for follow-up care for former ICU patients with COVID-19 is highly appreciated and underlines the importance of follow-up care for all critically ill patients.
Ethics statements
Patient consent for publication
Acknowledgments
We gratefully acknowledge the national foundation Family and Patient Centered Intensive Care (FCIC), and patient organisation IC Connect for ICU survivors and their family members for their close cooperation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MvdB, MZ, FvdL, ST, EA, JGvdH and DvS contributed to the design of the study. DvS drafted the manuscript. MvdB, MZ, FvdL, KS, DvB, DB-B, LLAB, JK, LV, MB, ST and EA were involved in the editing of the manuscript. All authors read and approved the final manuscript.
Funding This work was supported by Zorginstituut Nederland—ZonMw grant no 2021002343 and Radboud University Medical Center, Nijmegen, The Netherlands.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, conduct, reporting or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.