Article Text

Abstract
Objectives The burden of neurological disorders is increasing worldwide, including Asia. The purpose of this study was to determine the burden of neurological disorders between 1990 and 2019 in Asia using the Global Burden of Disease (GBD) Sociodemographic Index.
Design, setting, outcome and participants The GBD Study is updated every year and the most recent version provides the burden of diseases according to age, gender and region from 1990 to 2019. The burden of neurological disorders was evaluated as incidence, prevalence, mortality, disability-adjusted life-years (DALYs), years of life lost and years lived with disability.
Results In 2019, DALYs of neurological diseases were 64.4 million in South-East Asia (95% uncertainty interval (UI) 45.2 to 94.2) and 85.0 million in Western Pacific regions (95% UI 63.0 to 118.5). Stroke, migraine, Alzheimer’s disease and other dementias had the highest DALYs in the WHO South-East Asia and WHO Western Pacific regions in 2019. DALYs of stroke, Alzheimer’s disease and other dementias, Parkinson’s disease, brain and central nervous system cancer, multiple sclerosis, migraine and tension-type headache increased in both regions in 2019 compared with 1990. Infectious diseases such as tetanus, meningitis and encephalitis decreased in both regions. DALYs of idiopathic epilepsy and motor neuron disease increased in the WHO South-East Asia region and decreased in the WHO Western Pacific region.
Conclusions This study demonstrated the burden of neurological diseases in Asia. To reduce the burden of neurological diseases, strategies suitable for each country’s real healthcare needs and challenges are needed; this study can serve as the cornerstone of these strategies.
- epidemiology
- neurology
- dementia
- stroke
Data availability statement
Data are available in a public, open access repository. Data are publicly available at the Institute for Health Metrics and Evaluation (IHME) website (http://www.ghdx.healthdata.org/gbd-results-tool).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Our study showed the disability-adjusted life-years of 13 key neurological diseases in the Asian region in 2019 and compared the difference in disease patterns with those reported in 1990.
The Global Burden of Disease methodology offers standardised statistical approaches that are comparable across countries and time, which can reduce the challenges of trying to estimate disease burdens in terms of incidence, prevalence, mortality, years of life lost or years lived with disability, diminishing potential biases.
The quality of the information varies in the countries and there may be incomplete data.
Introduction
Neurological disorders are among the major causes of death and permanent or transient disabilities in human beings.1 Globally, the burden of neurological disorders is increasing.2 According to the 2016 Global Burden of Disease (GBD), it was the second most common cause of death and the leading cause of disability-adjusted life-years (DALYs).2 In addition, the incidence, prevalence and DALYs of neurological disorders are expected to increase with the increasing ageing population across the world. The ageing population is increasing in many countries, including the Asian countries.3 4 In Asia, the gap between the rich and the poor is also large and varies across countries.5 Notably, the prevalence and mortality of neurological diseases vary according to age and socioeconomic status6 7; and in Asia, these characteristics are likely to directly or indirectly affect the burden of neurological disorders. Moreover, different characteristics of the Asian population, including genetic, climatic, cultural and economic conditions, may present differences in the burden of neurological disorders between the Asian countries. Therefore, evaluating the burden of neurological diseases in the individual Asian countries is essential for health policymaking.
The GBD Study is a collaborative study of diseases worldwide, providing systematic information on 369 diseases in 204 countries each year.8 According to the recent GBD Study,9 10 neurological diseases are increasing worldwide including in Asia, but studies analysing each neurological disease in detail in Asia are lacking.
The purpose of this study was to determine the burden of neurological disorders, including incidence, prevalence, death, DALYs, years lived with disability (YLDs) and years of life lost (YLLs) between 1990 and 2019 in the Asian region and each Asian country using estimates from the GBD Study website.
Methods
Overview
Our data were extracted from GBD’s publicly provided website; all GBD’s research results can be freely accessed and downloaded from the GBD Compare and the Global Health Data Exchange websites (GBD Compare available at https://vizhub.healthdata.org/gbd-compare/; Global Health Data Exchange available at http://ghdx.healthdata.org/).8 The GBD 2019 methods are described in detail on the GBD website and in a previous study.9 The GBD 2019 is a worldwide multinational collaborative study. The GBD Study is updated every year and the most recent version provides the burden of diseases according to age, gender and region (369 diseases and injuries in 204 countries and territories) from 1990 to 2019. Our study data acquisition and analysis followed the methodology provided on the GBD website. Our study included 13 neurological diseases (the International Classification of Diseases (ICD) -10 codes) including stroke (I63), Alzheimer’s disease and other dementias (F01~03), Parkinson’s disease (G20), brain and central nervous system cancer (C71~72), idiopathic epilepsy (G40), motor neuron disease (G12.2), multiple sclerosis (G35), migraine (G43), tension-type headache (G44.2), meningitis (G00~03), encephalitis (G04~05), tetanus (A33~35) and other neurological disorders.
DALYs, YLDs and YLLs
The burden of each neurological disorder was separately evaluated as incidence, prevalence, death, DALYs, YLDs and YLLs.11 DALYs are defined as the sum of YLDs and YLLs. YLD is the individual sequela prevalence of each disease multiplied by disability weight, quantifying the severity of the sequela as a number between 0 (indicating full health) and 1 (indicating death).12 YLL is the number of deaths multiplied by the standard life expectancy at the time of death. Standard life expectancy is obtained from the lowest observed age-specific mortality rate among a world population of over 5 million.11 Disability weights were estimated from nine US population surveys and an open internet survey that asked respondents to choose the healthier option among random pairs of health conditions provided with brief descriptions of key characteristics.12
Detailed methods for obtaining non-fatal estimates and death information have been described in a previous research study.9 Considering DALYs, YLDs and YLLs, the neurological disorder estimates were acquired from disease surveillance systems, registries, survey microdata, health claims data and systematic reviews of reports.9 These datasets are repositioned to the Global Health Data Exchange, and data of different characteristics are analysed using DisMod-MR V.2.1, a Bayesian meta-regression tool.13 14 Age-standardised rate, which is a weighted average of the age-specific rates, was calculated to remove the confounding effect of age (standard age structure: a population structure used in the GBD Study to provide a constant distribution of covariates). Data were described using 95% uncertainty intervals (UIs) and changes from 1990 to 2019 as a percentage (95% UIs) provided by the GBD website.
Asian countries
In our study, the Asian region was analysed by dividing it into WHO South-East Asia region (11 countries) and WHO Western Pacific region (31 countries) according to the range of locations provided by GBD, and the burden of diseases calculated as an age-standardised rate per 100 000 was converted and compared with global data. Age-standardised rate of incidence, prevalence, death, DALYs, YLDs and YLLs, the total number for 1990 and 2019 and changes between 1990 and 2019 were investigated in WHO South-East Asia region and WHO Western Pacific Region. The WHO South-East Asia region countries were Bangladesh, Bhutan, Democratic People’s Republic of Korea, India, Indonesia, Maldives, Myanmar, Nepal, Sri Lanka, Thailand and Timor-Leste. The WHO Western Pacific region countries were American Samoa, Australia, Brunei Darussalam, Cambodia, China, Cook Islands, Fiji, Guam, Japan, Kiribati, Lao People’s Democratic Republic, Malaysia, Marshall Islands, Micronesia, Federated States of Mongolia, Nauru, New Zealand, Niue, Northern Mariana Islands, Palau, Papua New Guinea, Philippines, Republic of Korea, Samoa, Singapore, Solomon Islands, Tokelau, Tonga, Tuvalu, Vanuatu and Viet Nam (online supplemental figure 1).
Supplemental material
In Asia, the GBD Study separates high-income regions (Australasia: Australia and New Zealand; Asia Pacific countries: Brunei Darussalam, Japan, Republic of Korea and Singapore). Because the income level of the region may have influence on the mortality and prevalence of neurological diseases,15–17 our study investigated changes in DALYs between 1990 and 2019 in neurological disorders in Australasia and high-income Asia and Pacific regions.
Sociodemographic Index
Sociodemographic Index (SDI) is an index developed by GBD researchers, which measures the degree of socioeconomic development.18 It is a composite of the ranking of incomes per capita, educational attainment and fertility rates. SDI of 0 means the lowest level of development, while SDI of 1 means the theoretical maximal level. SDI was a predictor of the health-related indexes,19 and widely used in predicting health outcomes and comparing different regions.20 21 The limitations of other GBD indicators also apply to this index, including measurement bias of different sources.22 23
Patient and public involvement
Patients and the public were not involved in our research’s design, conduct, reporting or dissemination plans.
Results
The 2019 burden of neurological diseases in Asia
The 2019 DALYs of neurological diseases in WHO South-East Asia and WHO Western Pacific regions are shown in table 1. In 2019, there were 821.8 million cases of newly diagnosed neurological diseases worldwide: 227 million in the WHO South-East Asia region and 178.6 million in the WHO Western Pacific region. The total number of DALYs of neurological diseases was 64.4 million in South-East Asia region (95% UI 45.2 to 94.2) and 85.0 million in Western Pacific region (95% UI 63.0 to 118.5). Stroke, migraine, and Alzheimer’s disease and other dementias had the highest DALYs in WHO South-East Asia and WHO Western Pacific regions. This pattern was identical to the global trend of neurological diseases. When the incidence, prevalence and mortality of each neurological disease were compared in the two regions, stroke, Alzheimer’s disease and other dementias, Parkinson’s disease, brain and central nervous system cancer and motor neuron disease were higher in the WHO Western Pacific region, while multiple sclerosis, migraine, tension-type headache, meningitis, encephalitis and tetanus were higher in the WHO South-East Asia region (online supplemental table 1).
Disability-adjusted life-years of neurological diseases, comparison of South-East Asia and Western Pacific regions
Figure 1 shows age-standardised DALYs in the WHO South-East Asia and WHO Western Pacific regions. The burden of age-standardised DALYs was highest in both regions in the order of stroke, Alzheimer’s disease and other dementias, and migraine. The age-standardised DALYs of stroke, Alzheimer’s disease and other dementias, and brain and central nervous system cancer were higher in the WHO Western Pacific region. On the other hand, DALYs of multiple sclerosis, idiopathic epilepsy, migraine, meningitis and encephalitis were higher in the WHO South-East Asia region (figure 1).

2019 Contribution of DALYs in the WHO South-East Asia and WHO Western Pacific regions. DALYs, disability-adjusted life-years.
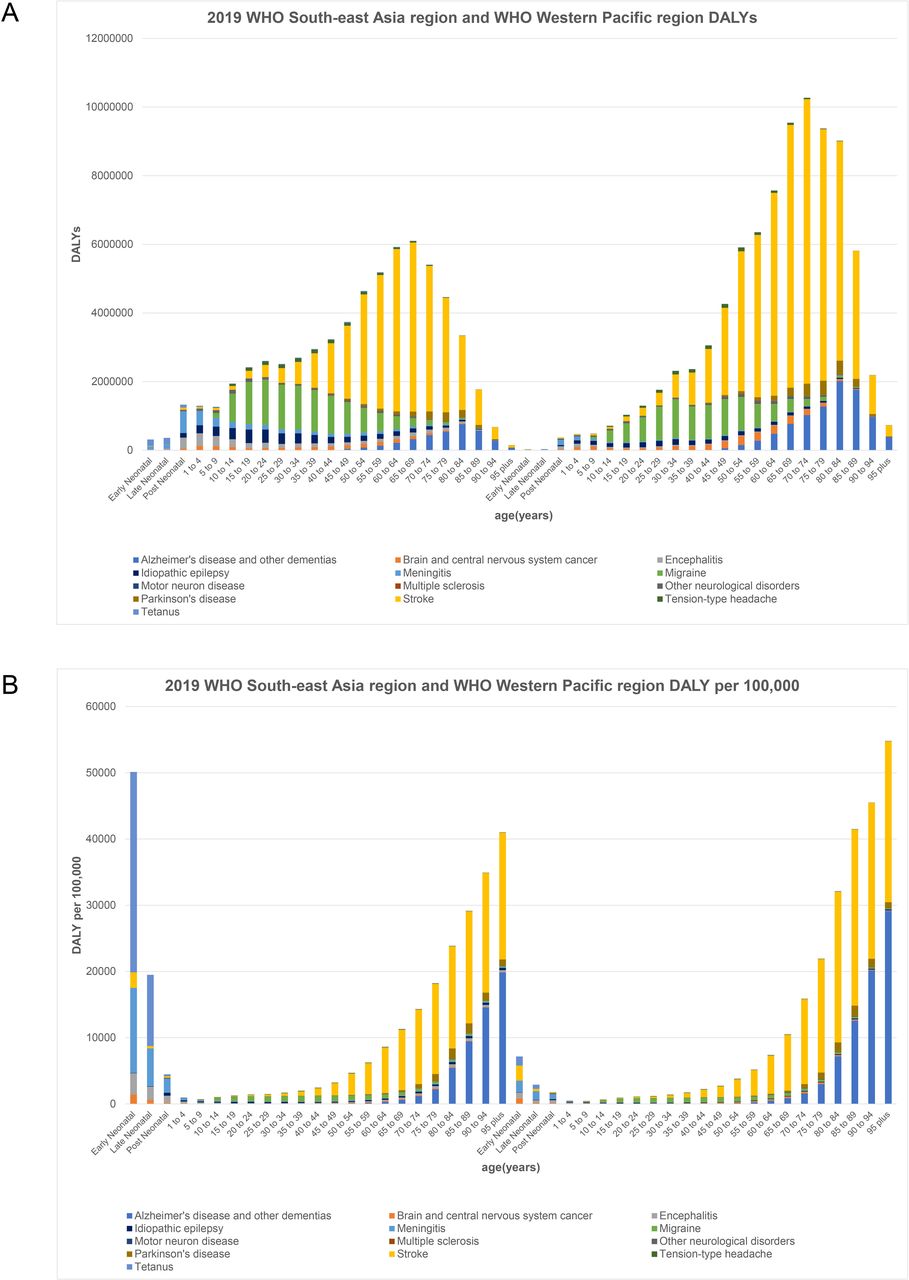
Figure 2 shows DALYs of neurological diseases in the Asian region by age. The total number of DALYs of stroke, Alzheimer’s disease and other dementias was higher in old age in both areas, and the age-standardised rate of stroke and dementia increased with age (figure 2A). However, the total number of DALYs of migraine was relatively higher in the younger generation. The highest DALYs of stroke were in the ages between 60 and 64 years in the WHO South-East Asia region and 70 and 74 years in the WHO Western Pacific region (figure 2B). When compared according to sex, the trend of DALYs in neurological diseases showed a similar pattern in the WHO South-East Asia and the WHO Western Pacific regions. The number of DALYs of stroke was higher in men, while DALYs of dementia and migraine were higher in women. DALYs according to age and sex are described in the online supplemental tables 2 and 3.

DALYs of neurological diseases in the Asian regions by age: (A) DALYs and (B) rate. DALYs, disability-adjusted life-years.
The difference of neurological diseases in Asia from 1990 to 2019
In the WHO South-East Asia region, stroke, tetanus and meningitis had the highest age-standardised DALYs in 1990, which changed to stroke, migraine, Alzheimer’s disease and other dementias in 2019. Age-standardised DALYs in the Western Pacific region showed a similar trend between 1990 and 2019, in the order of stroke, Alzheimer’s disease and other dementias, and migraine (table 2). The DALYs of stroke and Alzheimer’s disease and other dementias, Parkinson’s disease, brain and central nervous system cancer, multiple sclerosis, migraine and tension-type headache increased in both regions in 2019 compared with 1990. Infectious diseases such as tetanus, meningitis and encephalitis decreased in both regions. The number of DALYs of idiopathic epilepsy and motor neuron disease increased in the WHO South-East Asia region and decreased in the WHO Western Pacific region. The age-standardised rate of stroke incidence (−10%, 157 to 141 in South-East Asia; −12%, 211 to 186 in Western Pacific) and mortality (−30%, 135 to 95 in South-East Asia; −42%, 180 to 104 in Western Pacific) decreased markedly in both regions. The age-standardised incidence of dementia declined in South-East Asia (−3%, 71 to 69) and increased in Western Pacific regions (14%, 92 to 105). Mortality of dementia was increased in both regions. The age-standardised incidence and prevalence of migraine and tension-type headache in the WHO South-East Asia region have not changed since 1990, but these increased in the WHO Western Pacific region (online supplemental table 4).
Trends of neurological diseases in South-East Asia and Western Pacific regions between 1990 and 2019
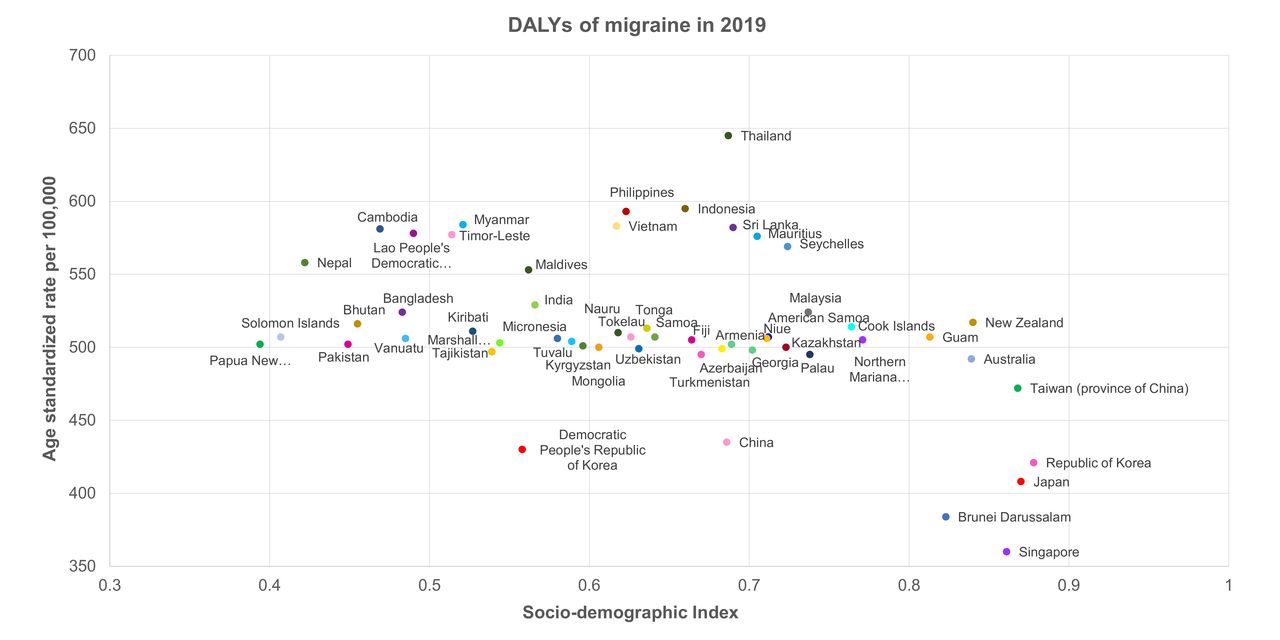
When age-standardised DALYs for each region were compared by income classification, motor neuron disease, multiple sclerosis and encephalitis increased in the Australasia region, in contrast to a decrease in the high-income Asia Pacific region. DALYs for Parkinson’s disease increased in the Australasia and the high-income Asia-Pacific regions, but DALYs for stroke, idiopathic epilepsy, meningitis and tetanus decreased (table 3). The age-standardised DALYs of stroke, Alzheimer’s disease and other dementias, and migraine according to SDI by country are presented in figures 3–5.

DALYs of stroke according to country-specific Sociodemographic Index. DALYs, disability-adjusted life-years.
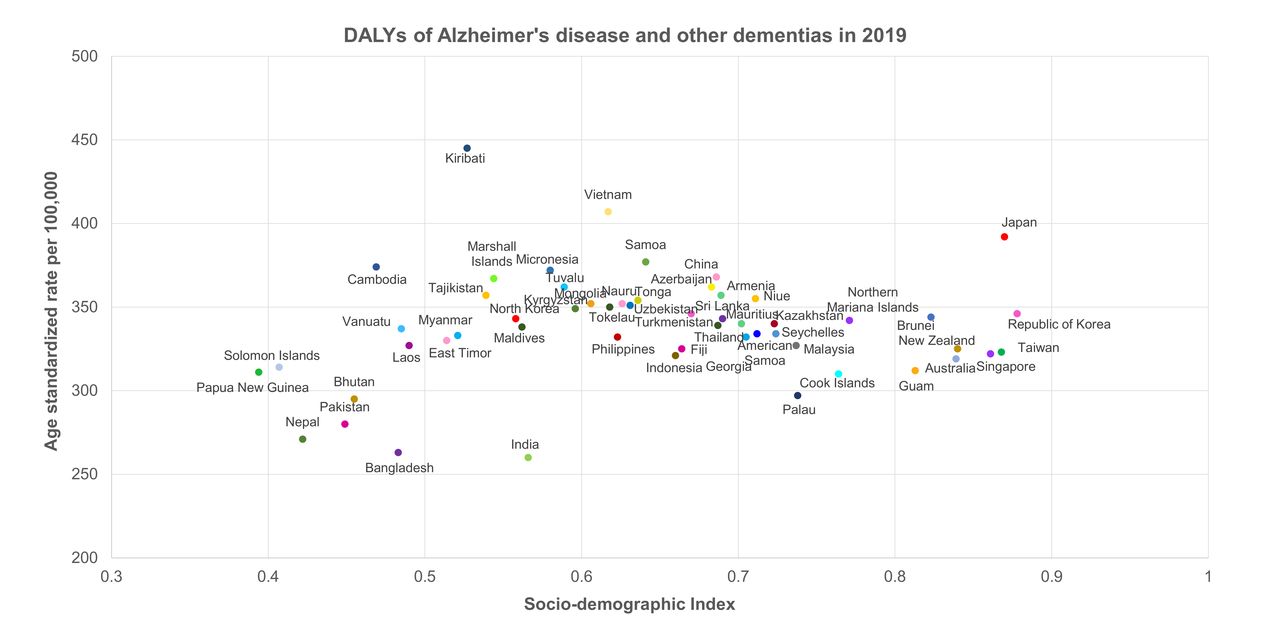
DALYs of Alzheimer’s disease and other dementias according to country-specific Sociodemographic Index. DALYs, disability-adjusted life-years.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
DALYs of migraine according to country-specific Sociodemographic Index. DALYs, disability-adjusted life-years.
Trends of neurological diseases in high-income Asia and Pacific regions between 1990 and 2019
When analysed by country, DALYs of stroke increased in China and India and decreased in Australia, Japan, the Republic of Korea and Singapore. Stroke mortality was raised in Australia, China, India and Japan, and dropped in the Republic of Korea and Singapore. Age-standardised rates of incidence, prevalence, death, DALYs, YLDs and YLLs burden by country are described in the online supplemental table 5. DALYs of Alzheimer’s disease and other dementias, and Parkinson’s disease increased in most countries, but decreased in Nauru, Niue and Tokelau. DALYs of motor neuron disease increased in Australia, Singapore and Japan, and decreased in China and the Republic of Korea. Mortality increased in Australia, China, Singapore and Japan, but decreased in the Republic of Korea. The DALYs of multiple sclerosis rose in all countries except Niue and Sri Lanka. Brain and central nervous system cancer decreased in Armenia, Niue and Tokelau, but increased in other countries. DALYs of idiopathic epilepsy increased in Australia and Singapore, and decreased in China and the Republic of Korea. Mortality decreased in Japan, the Republic of Korea and Singapore. Migraine’s DALYs increased in all the Asian countries apart from Armenia, Georgia, Niue, Northern Mariana Islands and Tokelau. DALYs of tension-type headaches increased in most countries except for Georgia, Niue and Tokelau. Meningitis decreased in all countries except Vanuatu, and mortality decreased in all countries except Guam and Vanuatu. DALYs of encephalitis increased in Australia, the Republic of Korea and Singapore, and decreased in China, Japan and India. Mortality increased in Australia, China, Japan, the Republic of Korea and Singapore. Tetanus increased in Guam, Kiribati, Papua New Guinea, Tajikistan and Vanuatu, but decreased in other countries.
Discussion
In the WHO South-East Asia and WHO Western Pacific regions, neurological diseases accounted for 3% and 5% of age-standardised DALYs in 2019.9 Among the leading causes of the global burden of disease all-age DALYs, stroke ranked 3rd and headache ranked 15th. Stroke, migraine and dementia accounted for the highest number of DALYs in the WHO South-East Asia and WHO Western Pacific regions, which did not differ significantly from the global trend. High DALYs of neurological diseases in the Asian region are thought to be due to increased life expectancy, as DALYs of neurological diseases were higher in the elderly. In particular, stroke and dementia have a higher incidence with advancing age, and the long life expectancy of these patients increases as medical technology advances. Headache frequently occurred in the young population. The increase in the burden of headaches might be due to changes in recognition of the disease and diagnostic criteria.
Stroke was the most common neurological disease in 1990 and 2019; compared with 1990, the total DALYs of stroke increased in both regions, but the age-standardised incidence and mortality rate decreased. Risk factors included hypertension, diabetes, dyslipidaemia, atrial fibrillation, smoking, alcohol, obstructive sleep apnea and other minor elements.24 25 The mortality attributed to hypertension and diabetes significantly reduced between 1990 and 2019.26 27 As awareness of the effects of these diseases on stroke has increased and the change of public health policies implemented, there is a possibility that it may have had the effect of reducing the burden. In addition, with the gradual development of medical treatment methods for each disease, the preventive effect of a stroke may have increased. Medications for hypertension, diabetes and dyslipidaemia have been continuously developed for decades, and researchers are focusing on the impact of these drugs on cardiovascular risk reduction.28–30 For atrial fibrillation, non-vitamin K antagonist oral anticoagulants, which have lower haemorrhagic complication rates than warfarin,31 are being widely used. Treatment methods for stroke have also made great strides. Intravenous thrombolytic therapy and endovascular thrombectomy are widely used and can effectively reduce mortality and disability after stroke.32 33 Furthermore, it is possible to maximise the treatment effect by educating the general public about the importance of the time window, developing a patient transport system and using stroke units. When the age-standardised DALYs according to SDI for each country were plotted, high-income countries showed lower DALYs. This suggests that there may be differences in access to medical care and preventive medicine depending on economic status. Therefore, it is necessary to develop prevention and treatment strategies for stroke in low-income countries.
DALYs of Alzheimer’s disease and other dementias were increased in both the WHO South-East Asia and WHO Western Pacific regions, which may be the consequence of an increased ageing population. However, the age-standardised rate of dementia in the WHO South-East Asia and WHO Western Pacific regions showed somewhat different patterns. In the WHO South-East Asia region, the change of dementia incidence was −3%, prevalence did not change and mortality and DALYs were increased by 10% and 7% each. In the WHO Western Pacific region, the incidence, prevalence, mortality and DALYs of dementia were increased by 14%, 25%, 7% and 9%, respectively. In the 2019 GBD report, DALYs of Alzheimer’s disease and other dementias were slightly increased from 1990.9 The exact cause of these differences is unknown, but nutrition, physical activity, genetic influence and access to healthcare may have affected the results.34 35 As for dementia, there seems to be no significant improvement compared with 1990, which could be attributed to the lack of development of new powerful preventive and therapeutic drugs.36 37 Considering the current global change into an ageing society, medical research and social support for dementia are essential.
Age-standardised incidence and prevalence of epilepsy increased, but YLL and mortality were markedly decreased, and YLD did not show significant change. It is estimated that there will be an impact from the development of various anti-epileptic drugs and advances in critical care medicine.38 The incidence of infectious diseases such as meningitis and encephalitis is decreasing worldwide,9 but that of encephalitis has increased in the Australasia region. Further investigations are needed to determine the exact cause of the increase in encephalitis in this region.
The neurological diseases show various patterns in each country, which is in line with previous reports.6 15–17 39 40 Environmental and geographical factors may have influenced these results. A rural area in Europe showed a higher prevalence of untreated hypertension, alcohol abuse, and higher incidence of stroke and cerebral haemorrhage compared with an urban area.41 A study in China also showed a geographical difference in hypertension and stroke between the north and south regions.42 Latitude gradient is reported to be influencing the prevalence of multiple sclerosis.43 In a systematic review, air pollution exposures were related to an increased risk of dementia.44 Thus, individual healthcare strategies should be applied according to the characteristics of each country.
Limitation
General limitations of the GBD Study also apply to this report. First, the quality of the information varies across the countries, and there may be incomplete data. Because we do not have access to the original dataset, we could not conduct further statistical analysis to reduce bias. Second, the definition of cause of death may vary across different medical data sources; a study in India reported that there is marked heterogeneity in reporting of deaths across states of India.45 These restrictions apply to other Asian countries as well. The results of this study should be interpreted with caution, due to limited access to original data, and most of the results are derived from the computation of a large dataset. However, the GBD Study takes these differences into account to make standard definitions and standard health indicators that can be compared among regions, countries and subnational settings. Third, the disability weights used to calculate YLD may vary across the countries. Fourth, a wide 95% UI is frequently noted, which implies the low precision of the estimate. Fifth, other neurological diseases, including peripheral neuropathy, tremor, dizziness and sleep disorders, were not included in the analysis because the GBD dataset does not have information on these diseases. Sixth, we could not suggest genetic epidemiological evidence for the Asian regions, which is a major limitation of our study. In a further study, information on the financial burden of neurological diseases will be helpful in making health policy decisions in Asia.
Conclusion
This study described the burden of neurological diseases in Asia. Although the DALYs of some neurological diseases are decreasing, it is necessary to pay attention to the diseases that are increasing. To reduce the burden of neurological disease, strategies suited to the reality of each country’s healthcare needs and challenges are needed, and this study can serve as the cornerstone of such effective strategies. Also, as COVID-19 became a pandemic in 2019, further research will help identify changes in disease burden before and after COVID-19. Due to the possible bias resulting from the limitations of the GBD research method, additional research is needed for accurate statistics for each country.
Data availability statement
Data are available in a public, open access repository. Data are publicly available at the Institute for Health Metrics and Evaluation (IHME) website (http://www.ghdx.healthdata.org/gbd-results-tool).
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Institutional Review Board at Ewha Womans University Seoul Hospital (ID: SEUMC202108006).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
SK, SE and YC are joint first authors.
SK, SE and YC contributed equally.
Contributors All authors contributed and approved the study’s protocol. YC drafted the first draft of the manuscript. SK, SE and T-JS analysed the data. AK, LJ, LS and JIS critically revised the manuscript. All authors read, edited and approved the final version of the manuscript. T-JS accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding This project was supported by a grant from the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Education (2021R1F1A1048113 to T-JS, 2021R1I1A1A01059868 to YC).
Disclaimer The funding source had no role in the design, conduct or reporting of the study.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.