Article Text

Abstract
Introduction Living with diabetes can be burdensome and lead to serious emotional distress and impaired mental health. Acceptance and commitment therapy (ACT) can support people facing the challenges of living with diabetes. This trial aims to evaluate the effectiveness and cost-effectiveness of the internet-based and mobile-based intervention (IMI) ‘ACTonDiabetes’ in reducing diabetes distress against enhanced treatment as usual (TAU+) following specialised diabetes care.
Methods and analysis A two-armed pragmatic randomised controlled trial will be conducted to evaluate the guided IMI ACTonDiabetes against TAU+. A total of 210 adults with type 1 or type 2 diabetes and elevated diabetes distress (Problem Areas in Diabetes ≥40) will be recruited at a specialised diabetes centre. The intervention begins 2–4 weeks after hospital discharge and takes about 7–10 weeks to complete. Assessments are performed at baseline and 5 and 10 weeks as well as 6 and 12 months after randomisation. The primary outcome is diabetes distress at a 10-week follow-up (T2). Secondary outcomes are depression (Patient Health Questionnaire-8), psychological well-being (WHO-5), quality of life (Assessment of Quality of Life-8 Dimension), Diabetes-related Self-Management Questionnaire, diabetes acceptance (Acceptance and Action Diabetes Questionnaire) and negative treatment effects (Inventory for the Assessment of Negative Effects of Psychotherapy). All statistical analyses will be performed based on the intention-to-treat principle with additional per-protocol analyses. Changes in outcomes will be evaluated using the general linear model. A health-economic evaluation will be conducted from a societal perspective. Reasons for drop-out will be systematically investigated.
Ethics and dissemination This clinical trial has been approved by the State Medical Chamber of Baden-Württemberg (file no. B-F-2019-010). Trial results will be submitted for publication in a peer-reviewed journal and presented at conferences.
Trial registration number DRKS00016738.
- depression & mood disorders
- general diabetes
- clinical trials
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first pragmatic randomised controlled trial investigating long-term effectiveness of a guided internet-based and mobile-based intervention for people with diabetes as aftercare intervention following inpatient diabetes care.
Cost-effectiveness analysis will inform healthcare policy about the economic value of the digital health intervention as part of diabetes inpatient aftercare.
Side effects and adverse events will be monitored.
ACTonDiabetes follows persuasive intervention design principles in order to keep intervention adherence on a high level.
Results of this monocentric trial might not be generalisable to diabetes inpatient aftercare, particularly internationally considering the varying healthcare systems.
Introduction
Living with diabetes mellitus type 1 or 2 comes along with a multitude of psychological challenges in addition to the requirements of persistent daily medical treatment and glucose management.1–4 Psychological aspects of chronic somatic diseases can have important implications for promoting coping mechanisms, the general functioning level, quality of life as well as other health outcomes.5–7 Psychological interventions can help people with diabetes to better cope with the diagnosis,7 adhere to complex treatment plans and manage their chronic condition in daily life.8–10 A growing body of evidence suggests the effectiveness of psychological interventions for diabetes distress and comorbid mental disorders such as depression and anxiety.11 12
Diabetes distress is an important psychological aspect of living with diabetes concerning mental health.4 Diabetes distress is defined as negative emotion and burden triggered by the demanding and progressive conditions of living with diabetes.13–15 It involves negative emotional reactions to specific aspects associated with diabetes.4 About 36% of people with type 2 diabetes15 and 41% of those with type 116 report elevated diabetes distress. Diabetes distress has been associated with an increased risk of developing depression.17 18 Furthermore, elevated diabetes distress is often accompanied by limited quality of life19 20 and has been associated with less optimal diabetes self-management.20 21 Clinical guidelines recommend screening and treatment of diabetes distress as integral part of routine diabetes care.22 23
Apart from the consequences of living with diabetes on the individual level, the economic consequences for society, such as in terms of lost work time and healthcare costs, are also significant.24–27 Kalsekar et al28 estimate a society-wide cost increase of 50%–90% in people with type 2 diabetes with mental comorbidities versus without. There are multiple barriers regarding access to mental healthcare such as limited mobility, time, resources as well as access to and availability of healthcare offers in the target population.29–32
People with diabetes may attend specialised diabetes education and treatment programmes offered as part of secondary or tertiary care (eg, diabetes self-management education) to update diabetes knowledge, improve their healthcare and diabetes management skills, check diabetes outcomes or to treat acute or long-term complications of diabetes.33 There is evidence that diabetes distress may improve after an inpatient hospital stay, but effects may diminish on medium term and long term.33 Psychological interventions can help to sustain treatment effects and help patients to transfer new insights, skills and routines into daily life.34–36 Such interventions can be based on different psychotherapeutic approaches like acceptance and commitment therapy (ACT).37 In comparison to the traditional cognitive–behavioural therapy (CBT) approach, ACT adds a focus on mindfulness.37 Instead of focussing strategies to reduce unfavourable thoughts and feelings (=CBT), ACT-strategies focus on experiential acceptance of unchangeable aspects of negative feelings and promotes a value-oriented search movement, which can help to accept unchangeable aspects of life.37 Thus, experiential acceptance might be particularly helpful for people with a chronic somatic disease like diabetes as it may help people cope with the ongoing treatment requirements and diabetes-associated burdens. This could reduce diabetes distress. Recent meta-analyses on ACT-based interventions report promising results. One meta-analysis reveals reductions of diabetes distress (SMD=−0.37, 95% CI −0.63 to −0.12),38 two meta-analyses report reductions in glycated haemoglobin (HbA1C) (MD=−0.35 and −0.62% points)38 39 in favour of intervention groups (IGs) when compared with treatment as usual (TAU) or enhanced TAU+. However, both meta-analyses call for further high-quality studies in the field.38 39
Internet-based and mobile-based interventions (IMIs) could be a flexible and cost-effective medium to provide aftercare following a diabetes education and treatment programme in people with diabetes. IMI can help to overcome healthcare barriers by delivering low-threshold healthcare interventions on a large scale.40 Recent meta-analyses show that IMIs may be as effective as face-to-face psychotherapy in treating comorbid mental disorders in people with chronic somatic diseases.41 IMIs have been effectively used for the supportive treatment of diabetes (eg, for improving nutrition habits42 and physical activity42 as well as fostering more consistent diabetes self-management43 and smoking cessation44) as well as for the treatment of psychosocial distress and common comorbid mental disorders of diabetes (eg, reducing anxiety,45 depression,45 46 diabetes distress45 47). However, these findings originate from studies carried out in more standardised research contexts rather than the ‘real world’. IMIs as aftercare have proven their potential in a variety of mental disorders and somatic conditions,48–50 while evidence on diabetes aftercare is missing.
Objectives
The aim of this trial is to evaluate the effectiveness and cost-effectiveness of ACTonDiabetes, an IMI based on ACT specifically developed for patients with diabetes. Primary aim is to investigate the research question:
Does ACTonDiabetes result in improved diabetes distress compared with TAU+ a psychoeducative booklet (=TAU+)?
The following secondary research questions will be investigated:
Does ACTonDiabetes result in improved secondary medical and psychosocial outcomes compared with TAU+?
Is ACTonDiabetes cost-effective compared with TAU+?
Are there side effects and adverse events associated with ACTonDiabetes?
Which variables moderate and mediate the effects of ACTonDiabetes?
Methods and analysis
Study design
A two-armed pragmatic randomised controlled trial (RCT) will be conducted comparing the effects of a guided version of ACTonDiabetes (IG) compared with a control group (CG) receiving enhanced standard care (TAU+). Primary and secondary outcomes will be assessed over a period of 12 months. Assessments will take place at baseline (T0), intermediately (4 weeks, T1), as well as 10-week and 6-month and 12-month (T2–T4) follow-up (figure 1). Data collection started in June 2019 and will end approximately in December 2022.

Flow chart of the planned study procedure. PAID, Problem Areas in Diabetes; TAU, treatment as usual.
Eligibility criteria
Patients are eligible for inclusion if they: have type 1 or type 2 diabetes mellitus, indicate elevated diabetes distress (Problem Areas in Diabetes, PAID sum score ≥40), age 18 years or older, were recently treated as an inpatient in the diabetes centre (<4 weeks), have internet access and an email address; have sufficient German language skills and provide written informed consent. Exclusion criteria are: other specific types of diabetes and cognitive impairment (eg, dementia, diagnoses according to patient records).
Recruitment
This clinical trial is carried out in collaboration with a specialised inpatient diabetes centre in Germany (Diabetes Center Mergentheim). On admission at the clinic, patients with diabetes are asked whether they would be willing to be informed about current research projects. People providing consent will be screened for inclusion and exclusion criteria within the first days of their stay by research staff. Screening will include a self-report measure of diabetes distress. Eligible patients for the present trial will be contacted by research staff and informed about the study and ACTonDiabetes. People providing written informed consent will be referred to the study centre (Ulm University) for baseline assessment and randomisation. Participating patients are asked to complete the baseline assessment (T0) within 4 weeks after discharge from the diabetes clinic.
Randomisation and blinding
The group allocation is performed by persons who are blinded towards the endpoints and study procedures and not otherwise involved in the study. After completion of the baseline assessment, participants are randomised to either the IG or the control condition (TAU+). A permuted block randomisation with 6, 9 and 12 blocksize and an allocation ratio of 1:1 will be used. Group membership is only known by the persons administering allocated treatments to participants (MM and AW). Data collectors are blinded with regard to group membership. The randomisation list is created by an automated web-based programme named ‘sealed envelope’ (https://sealedenvelope.com). Participants are informed about their group allocation via email.
Intervention
ACTonDiabetes was developed on the basis of an already evaluated IMI ‘ACTonPain’.51 52 ACTonPain was found to be effective in reducing pain interference in people with chronic pain.52 The content of the ACTonPain intervention was adapted to the population of people with diabetes and subsequently tested in a pilot trial.53 Based on the findings of the pilot trial, ACTonDiabetes was further developed. Changes concern a strengthened ACT focus, shortened text passages supplemented with more persuasive design components54 such as interactive materials and visualisations. The feasibility trial also showed that participants wanted to bring in more of their personal lives and work on their own stories. To address this finding, a therapeutic writing was incorporated. One reason for adding a writing intervention was to foster the feeling that the intervention is personalised for the individual, with space for reflections about life and living. Another reason was to support contact with positive aspects in life and inducing positive emotions following positive psychological writing approaches.55–58 Writing tasks include writings on the personal life story and benefit finding writing.
The intervention consists of seven core elements: psychoeducation, exemplary people with diabetes, ACT-based exercises, for example, mindfulness exercises, diaries to document their progress, a therapeutic writing intervention, feedback from e-coaches (trained psychologist) and optional SMS coaching. Illustrations of contents comprise video sequences and ACT-metaphors in the form of text or audio.
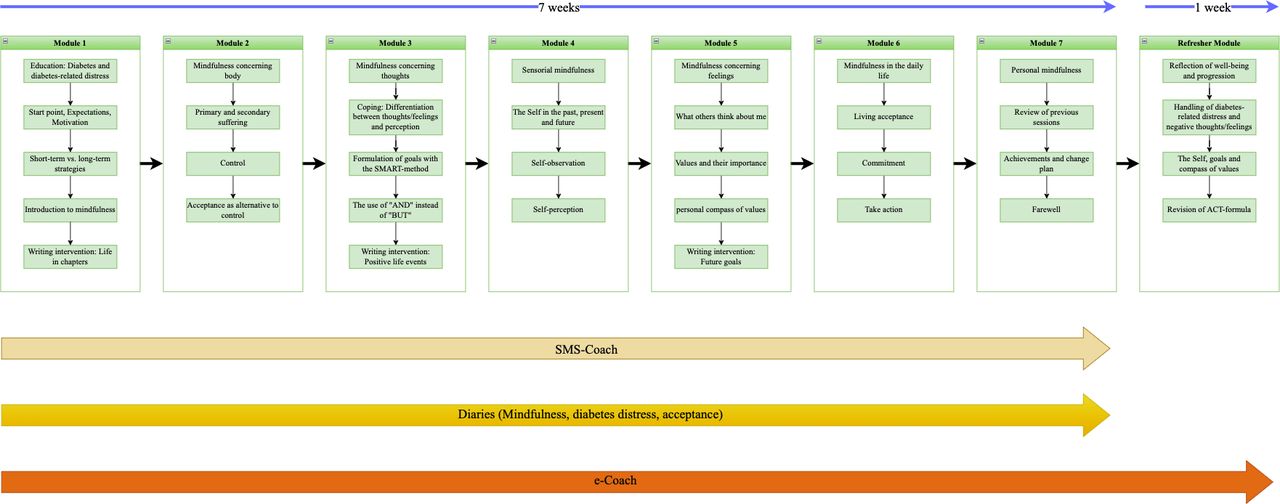
Participants are recommended and encouraged by e-coaches to complete one module per week (ie, process through the intervention within 7 weeks) and to complete the refresher module 4 weeks after the seventh module is finished. Similar to a face-to-face psychotherapy session, processing through one module is conceptualised to take approximately 45–60 min. However, there is no time limit and participants can take breaks whenever they want to and are actively encouraged to do so every 15–20 min. After completing a module, participants are encouraged to set a concrete date for the next module and to practice the newly learnt strategies in between. Participants of the IG are guided by e-coaches who are psychologists supervised by a senior e-coach (EB) and a senior psychotherapist (HB). Tasks of the e-coaches comprise a welcoming message, answering questions, giving feedback on each module as well as reminding participants to do the training if they pause without prior notice. If participants do not complete the weekly module, they are reminded by their e-coach twice to complete it. If the participants have not completed the module by then, the module is deactivated and the participants need to reactivate it by contacting the e-coach to gain access. Within 2 weekdays after finishing a module, participants receive a feedback email from their e-coach and the following module is being activated. Emails are standardised, existing templates are chosen and partly adapted to participants input. Participants can reaccess the intervention and download key content (table 1) until 1 year after randomisation. At the end of every module, a conclusion and a brief preview of the next module is presented. The intervention structure and procedures are shown in figure 2.

{kind=link}
{kind=link}
Intervention structure and procedure. ACT, acceptance and commitment therapy.
Content and techniques of the ACTonDiabetes intervention based on Hayes et al101
Participants are advised to document their mindfulness practice and write an ‘acceptance diary’ to reflect on their progress of using acceptance in stressful situations. Detailed information on intervention contents can be retrieved from online supplemental material S1.
Supplemental material
ACTonDiabetes is offered on the minddistrict platform (https://www.minddistrict.com). Access to the platform is via a unique username-password combination and is available 24/7 from all devices with internet access. However, ACTonDiabetes is optimised for PCs, notebooks and (large-screen) tablets. All transferred data are secured via www.minddistrict.com based on ISO27001:2013, ISAE 3402 type II and guidelines NEN7510, ISO14001.
Mechanisms to foster adherence
Guidance
If participants do not complete the next module 2 weekdays after their scheduled time point, participants receive three standardised reminders by their e-coach before an email about the upcoming deactivation of the account is sent. Participants receive a call before deactivation and can reactive their account anytime during the trial. Guidance aims at encouraging and motivating the participants. Total amount of time invested by an e-coach across the whole programme for one participant should be on average not exceed 60 min. Actual guidance time spent by e-coaches will be documented.
SMS coach
In module 1, participants can choose if they want to be supported by text messages for the next 7 weeks during the training. Participants selecting the SMS coach receive one SMS per week. SMS will be sent at different times (morning, noon and afternoon). These text messages are standardised and have motivating and supportive content (eg, tiny tasks and reminders to practice mindfulness).
Administrative and technical support
In case participants forget their password or have other technical issues, they can contact the study team for technical support at every point during the training.
Enhanced TAU control condition
Participants of the IG and CG both have unrestricted access to TAU. Participants of the CG receive a booklet with psychoeducation (=enhanced TAU, TAU+) on basic principles of ACT and diabetes distress. Additionally, the booklet contains information on further treatment options in primary and secondary (mental) healthcare. This means that the intervention will be tested against a control condition including a minimal intervention, resulting in a stricter, more conservative test of its effectiveness.
Assessments
Data will be collected on-site (screening) and online at baseline (T0), intermediately (5 weeks postrandomisation=T1) and 10 weeks (proxy for post-treatment=T2), 6 months (T3) and 12 months (T4) after randomisation. A flow chart of the study can be seen in figure 1. The outcomes, their measurement instrument and points of assessment are shown in table 2.
Measurement instruments, constructs and points of assessment
Screening
The German version of the PAID questionnaire59 is administered to assess diabetes distress when admitted to the diabetes clinic. Additionally, the screening includes age, sex, diabetes type and duration, long-term complications of diabetes and concomitant diseases and glycated haemoglobin (HbA1c; according to medical records/current diagnostics) as well as the assessment of sufficient knowledge of German language, internet access and preliminary release date (leaving the diabetes clinic).
Sociodemographic and medical data
Sociodemographic data (collected at T0 survey) includes information on sex, age, citizenship, federal state, marital status and education. Diabetes-related medical data (collected as part of the screening) includes diabetes type and duration in years, long-term complications of diabetes and concomitant diseases, HbA1c as well as information on illness and treatment like physical and psychological treatment, physical activity, alcohol and tobacco use and somatic risk factors (body mass index, arterial hypertension, comorbid chronic diseases).
Outcome measurements
Primary outcome
The primary outcome is the reduction of diabetes distress at T2 assessed with the German version of the ‘PAID’ scale.59 Twenty items evaluate common diabetes-related emotional burdens (eg, ‘Feeling alone with your diabetes?’). Participants can answer on a 5-point Likert scale (0 = ‘no problem’ to 4 = ‘serious problem’). The sum of raw scores is multiplied with 1.25 and produces a total score (range: 0–100). Higher scores indicate more severe diabetes distress: Values of 40 or higher indicate serious diabetes distress.60 The German version shows internal consistencies between α=0.92 and 0.95.61 62 The reduction of diabetes distress will also be evaluated at 6-month follow-up and 12-month follow-up as secondary outcome.
Secondary outcomes and covariates
Psychological well-being
Psychological well-being is measured by the ‘WHO-Five Well-being Index (WHO-5)’.63 Psychological well-being for the past 2 weeks is rated with five items (eg, ‘I have felt cheerful and in good spirits’) on a 6-point Likert scale (0 = ‘at no time’ to 5 = ‘all the time’). The raw sum score is transformed to a total score ranging from 0 to 100 (by multiplication by 4). Higher scores indicate higher well-being. Cronbach’s α in a large representative German sample is high (α=0.92).64
Depressive symptoms
Depressive symptoms are assessed by the ‘Patient Health Questionnaire-8’.65 Eight items request the defining symptoms of depression according to the DSM (eg, ‘feeling down, depressed or hopeless’). Symptom frequency is rated on a 4-point Likert scale (0 = ‘not at all’ to 3 = ‘almost every day’). There is an additional item which requests to which degree functioning in daily life is limited and/or to which degree the person suffers from the reported symptoms. A total score of 10 or more indicates likely depression.65 Cronbach’s α is high (α=0.82).65
Diabetes acceptance
Psychological flexibility towards diabetes will be measured using the ‘Acceptance and Action Diabetes Questionnaire’,66 an 11-item questionnaire with a five-point Likert response scale (1 = ‘never’ to 5 = ‘nearly always’). Items concern the acceptance of diabetes-related negative feelings and thoughts and its impact on valued action (eg, ‘I do not take care of my diabetes because it reminds me that I have diabetes’). The German version has shown an internal consistency of α=0.85.66
Psychological flexibility
The German version of the ‘Acceptance and Action Questionnaire-II’67 is a measure of psychological inflexibility consisting of 7 items. On a 7-point Likert scale, ranging from 0 = ‘never true’ to 6 = ‘always true’, a person’s willingness to experience unwanted thoughts and feelings and their ability to act despite the presence of undesirable thoughts and feelings is assessed. In this study, items were reverse coded to reflect psychological flexibility rather than inflexibility. Sum scores (range: 0–42) are computed with higher values indicating higher psychological flexibility. The questionnaire has shown good psychometric properties in a German sample.67
Diabetes-related self-management
The participants’ self-management is measured by the ‘Diabetes Self-Management Questionnaire (DSMQ)’.68 It consists of 16 items formulated as behaviour descriptions from the participant’s perspective (eg, ‘I take my diabetes medication (eg, insulin, tablets) as prescribed’). Answers are given on a 4-point Likert scale (0 = ‘does not apply to me’ to 3 = ‘applies to me very much’). The DSMQ covers five different aspects of self-management: dietary control, medication adherence, blood glucose monitoring, physically activity and physician contact. The items refer to the previous 8 weeks.69 The DSMQ shows an internal consistency of α=0.88.70
Fear of progression
The short form of the ‘Fear of Progression Questionnaire’ worries and fear of disease progression can be captured within people with chronic diseases.71 The response to twelve Items is documented on a 5-point Likert scale (1 = ‘never’ to 5 = ‘very often’). Internal consistency is good (Cronbach’s α=0.87).71
Emotion regulation
The ‘Emotion Regulation Questionnaire’72 is a 10-item questionnaire measuring positive and negative feelings as well as their regulation. Items refer to two different emotion regulation strategies: Reappraisal and suppression. Participants rate the items on a scale from 1 (‘strongly disagree’) to 7 (‘strongly agree’). Means show the preference for each strategy indicating higher preference at higher mean scores. Internal consistencies (α) are acceptable to good and differ from 0.75 to 0.82.72
Metacognition
The revised ‘Metacognitions about Symptoms Control Scale’73 assesses negative and positive metacognitions by focusing on and thinking about symptoms. A 4-point Likert scale (1 = ‘do not agree’ to 4 = ‘agree strongly’) is used to rate the eight items in the revised version. Internal consistencies for the German version for both of the factors (positive/negative) are between acceptable and good, differing from α=0.70 to α=0.80.73
Treatment expectancy
Treatment expectancy is measured with the ‘Credibility/Expectancy Questionnaire’74 with six items at T0. Four items are rated on a 9-point and two items on a 10-point Likert scale with varying descriptions. The scale can be separated in the two factors credibility and expectancy. Cronbach’s α for credibility varies from 0.79 to 0.90, for expectancy from 0.81 to 0.86 and for the total scale from 0.84 to 0.85 indicating acceptable to high internal consistency.74
Intervention satisfaction
To assess satisfaction with intervention, the ‘Client Satisfaction Questionnaire (CSQ)’75 is used at T2. In the CSQ, participants rate their satisfaction with the intervention on a 4-point Likert scale for each of the eight items. Higher scores indicate higher satisfaction. Cronbach’s α is very good (α=0.9).76 For psychosomatic populations, a mean of M=23.5 (SD=5.0) and Cronbach’s α=0.93 is reported.75 Values greater than M=23 are classified as good treatment satisfaction.75 Treatment satisfaction should at least be deemed as ‘good’ for indicating that the intervention is acceptable with regard to treatment satisfaction.
Negative side effects
Experienced negative side effects of the intervention and enhanced TAU are recorded with the Inventory for the ‘Assessment of Negative Effects of Psychotherapy’77 at T2. It consists of 22 (IG) or 18 (CG) Items. Items are partly rated on a 4-point Likert scale (0 = ‘no agreement’ to 3 = ‘total agreement’) partly on a bipolar 7-point scale. Adverse effects in social life, intrapersonal factors or work-related situations are taken into consideration. The original inventory with 32 items has an internal consistency of α=0.95.78 Additionally, as an indicator of (serious) adverse events, reliable symptom deterioration rates will be reported.
Working alliance
The short, revised version of the ‘Working Alliance Inventory (WAI-SR)’79 will be applied to measure the therapeutic alliance between client and e-coach at T2. The 12-item self-report questionnaire covers the three subscales, namely: (A) agreement on tasks, (B) agreement on goals and (3) development of an affective bond. For the German version, internal consistencies (α) between 0.81 and 0.91 were reported for the subscales and between 0.90 and 0.93 for the total score.80 Participants in IG will complete the WAI-SR at T2. Additionally, e-coaches will be requested to complete the 10-item therapist version (WAI-SRT)81 at T2. This will allow us to compare how the therapeutic relationship is experienced by client and by e-coach, to gain a comprehensive picture of the experienced working alliance. The WAI-SR and the WAI-SRT were adapted in wording for the current study investigating therapeutic alliance in guided IMI. The items were changed to refer to e-coaches instead of therapists and to online trainings instead of therapy.
Healthcare utilisation
Healthcare utilisation will be measured with the TiC-P82 to achieve a detailed description of TAU+. Cost evaluation will be based on the German version of the Dutch cost questionnaire ‘Trimbos Institute and Institute of Medical Technology Questionnaire for Costs Associated with Psychiatric Illness’ (TiC-P).82 This self-report questionnaire assesses the usage of healthcare services (eg, general practice services, intake of medications, sessions with psychotherapists or psychiatrists) and productivity loss (eg, hospital days, absenteeism and presentism). The questionnaire was specifically adapted to people with type 1 or type 2 diabetes.
Quality of life
Quality of life will be assessed using the ‘Assessment of Quality of Life Inventory-8 Dimension (AQoL-8D)’.83 Each of 35 items loads on 1 of 8 dimensions of life of quality and is rated on 4–6 point scales. For analysis, there is an algorithm which can be used for quality of life in general as well as for subdimensions (independent living, pain, senses, mental health, happiness, coping, relationships and self-worth). The total scores can range between 0 and 1. Norm values are available. Reliability of AQoL-8D is very good with a Cronbach’s α of 0.96.83
Drop-out
Reasons for participants dropping out are assessed systematically using a drop-out questionnaire with various items and open questions at the time of drop-out.84 The following are recorded in the IG: prerandomisation (potentially eligible persons who expressed an initial interest in participating but then do not participate), pretreatment (persons who were randomised but then do not start the intervention) and treatment drop-out (persons who began the treatment but do not complete it). Additionally, participants in the CG receive a questionnaire on drop-out reasons if they decide to end their participation.
Centrality of events
The ‘Centrality of Event Scale (CES)’85 is used to evaluate the paradigm of therapeutic writing. The CES measures the centrality of an event to a person, differentiating three independent characteristics. Whether the event is seen as (1) a reference point for everyday inferences, (2) a turning point in the life story and (3) as an element of the personal identity. Participants rate the 7 items of the short-term version on a 5-point Likert scale from 1 = ‘totally disagree’ to 5 = ‘totally agree’. With a Cronbach’s α of 0.88 the scale shows good internal consistency.85
Gratitude
The ‘Gratitude Questionnaire (GQ-6)’86 is used to evaluate the gratitude task within the expressive writing paradigm. GQ-6 measures the level of dispositional gratitude in participants. The GQ-6 is a 6-item self-report scale (eg, ‘I have so much in live to be thankful for’) using a 7-point Likert scale from 1 (‘strongly disagree’) to 7 (‘strongly agree’). Two items are negatively keyed to inhibit response bias. Total scores can range from 6 to 42 with higher scores indicating greater levels of dispositional gratitude. Internal consistency is high (Cronbach’s α=0.87).86
Postwriting questionnaire
To assess the paradigm of expressive writing after every writing session the participants answer four questions about their feelings and thoughts during and after the writing experience. Answers are rated on a 5-point Likert scale (1 = ‘not at all’, 3 = ‘few’, 5 = ‘very much/extremely’). The questionnaire was adapted from the English version of Pennebaker et al87 by the authors.
Intervention use
The minddistrict platform collects data on user activity. Data include the time of the start and end of a module as well as the previously described postwriting questionnaire and participants narratives.
Sample size
Primary endpoint of this study is the standardised mean difference between the IG and TAU +in diabetes distress at T2. A meta-analysis on ACT in comparison to (active) controls found an effect of g=0.42 favouring the ACT condition.88 Spijkerman et al found an effect for guided mindfulness-based IMIs of g=0.43.89 For an IMI comparable to ours targeting diabetes distress and depressive symptoms, Nobis et al90 found an effect size of d=0.58 (intention-to-treat, ITT) for the reduction of diabetes distress at post-treatment. A meta-analysis on ACT interventions for the reduction of diabetes distress revealed a reduction of Standardized Mean Difference (SMD) =0.37 in favour of IGs in comparison to TAU or TAU +controls.38 As a consequence the pooled effect size of d=0.45 is being expected. Power analysis with G*Power91 recommend a sample size of 105 participants per group on the assumption of two-tailed testing, an alpha error probability of α=0.05 and power of 1−β=0.90. Thus, we aim at recruiting n=105 per group, that is 210 randomised persons per total sample. As data analysis will be based on ITT principles, increasing sample size in order to compensate for drop-outs is not necessary.
Statistical analyses
Patterns of missing data will be examined and analyses will be adjusted accordingly (ie, multiple imputation), provided that no patterns of systematically missing data can be found.92 If the missing data mechanism will not be at least missing at random, sensitivity analysis will be employed. Analyses will be conducted on a two-sided level of significance (α=0.05). Participant characteristics will be described using descriptive statistics. No interim analyses will be performed to the primary outcome.
All statistical analyses will be performed based on (ITT principle. Additionally, per-protocol analyses will be conducted based on the subsample who substantially completed the intervention (at least 80% of the modules) until 10 weeks (T2), 6 months (T3) and 12 months (T4) after randomisation.
Linear regression analysis with robust SEs will be used to evaluate group differences between IG and CG on the primary outcome (reduction of diabetes distress) at T2 (10 weeks after randomisation), adjusting for baseline scores and also evaluating the baseline × group interaction. Standardised mean differences and 95% CIs at all measurement points will be calculated. Long-term effects will be evaluated using linear mixed-effect modelling.
Secondary outcomes will be analysed accordingly. Exploratory mediation and moderation analyses involving the primary and secondary outcomes as well as demographic data will be performed. Sociodemographic (eg, age, sex) and health-related variables (eg, baseline diabetes distress) will be analysed. Regression analyses will be applied with group as an effect-coded predictor along with the main effects of moderator variables and their interaction effects with group. Effect coding will be applied to categorical and z-standardisation to continuous variables. Each moderator will be tested in a separate regression model. Mediation analyses will be conducted to examine potential processes that explain effects on health outcomes (eg, psychological flexibility, emotion regulation, metacognition, working alliance). Analyses on cost-effectiveness will be performed from a societal (eg, all relevant costs) and public healthcare perspective (eg, direct medical costs) within a time frame of 12 months. Missing cost and effect data will be imputed (eg, multiple imputation by chained equations), given there are no patterns of systematically missing data.
Patient and public involvement
Patient and public involvement (PPI) representatives provide input to this study in several stages. Results of the feasibility trial on ACTonDiabetes were used to further develop and optimise study design and procedures. PPI representatives were included in the intervention development to improve content and usability of ACTonDiabetes.
Discussion
ACTonDiabetes has the potential to decrease diabetes distress following diabetes inpatient care. Considering the high prevalence rate of diabetes worldwide, amounting to 451 million and estimated to increase to 693 million adults until 2045 as well as the prevalence of 36%–41% of people with diabetes affected by diabetes distress15 16 the possible population targeted with ACTonDiabetes is substantial.93 Adults experiencing elevated diabetes distress hold a threefold risk of developing depressive symptoms,17 which illustrates the psychological burden that often comes along with living with diabetes as well as increased macrosocial cost that arise for comorbid psychosocial issues in people with diabetes.28 These findings support a high need and potential for improvement of an easily accessible and potentially cost-effective treatment for the large and growing diabetes population.
The planned study is characterised by a number of strengths: First, ACTonDiabetes has been successfully tested within a randomised controlled pilot trial and has shown its feasibility in people with diabetes.53 ACTonDiabetes could provide a suitable intervention for patients with diabetes and diabetes distress. It may help people maintaining psychosocial health and further decrease diabetes distress. Second, we will systematically collect data on potential adverse events/negative effects and investigate if they could be related to the intervention. Third, long-term effectiveness of ACTonDiabetes will be investigated. To our knowledge, there are no data from previous studies regarding long-term effectiveness of an ACT-based intervention for people with diabetes. This trial will gather information on cost-effectiveness of an IMI programme over a follow-up period of 12 months.
Potential obstacles need to be taken into account. One problem could arise from suboptimal treatment acceptance. Baumeister et al94 found that 91.5% of people with diabetes displayed a moderate or even low level of acceptance towards an IMI aiming at reducing depressive symptoms. However, the feasibility trial on ACTonDiabetes revealed neutral or positive average acceptance levels as reported by the participants.53 Implementing the ACTonDiabetes intervention immediately after an inpatient stay might even be more favourable for acceptance as patients might be more open to receiving an intervention and aiming for personal change.
Furthermore, moderate to high discontinuation rates are a general problem within online and offline psychological interventions, which has to be considered.34 In the feasibility trial on ACTonDiabetes, 42%of the participants dropped out at some point during the study which could be (partly) explained by unfulfilled expectations concerning the intervention contents.53 Another explanation for high drop-out rates might be the high temporal effort and textual content of the modules.53 To improve study adherence, the online training was therefore edited to shorten contents and text passages. More interactive and illustrative elements were included in the intervention. Besides this, guidance by trained e-coaches as well as an SMS coach were added to the intervention. Both components have shown to improve intervention adherence.95 96 In addition, standardised reminding procedures are applied. Reasons for intervention drop-out will be assessed via questionnaire to help improve future IMI for decreasing drop-out rates.
This trial enrols people with both type 1 and type 2 diabetes. This is because diabetes distress is a common concern in both types and we expect that the tested intervention may be effective for both of them. Furthermore, people with type 2 diabetes referred to the centre usually have long-standing diabetes treated with insulin, so they are likely to experience similar conditions as those with type 1 diabetes and the potential sources of diabetes distress may be similar. Nevertheless, specific requirements and burdens may vary with treatment regimens, thus there is a risk of heterogeneity due to the inclusion of more than one diabetes type, which will need to be considered.
Ethics and dissemination
This clinical trial has been approved by the State Medical Chamber of Baden-Württemberg (file no. B-F-2019-010). Written informed consent for participation in the study will be obtained from all participants prior to their involvement. Participants will receive written information on study conditions, data security, publication of anonymised results, voluntariness of participation and the right to leave the study at all times. This clinical trial will be reported in accordance with the Consolidated Standards of Reporting Trials Statement 2010, the extension for reporting pragmatic trials97 98 and the Standard Protocol Items: Recommendations for Interventional Trials guidelines for reporting protocols of RCTs99 as well as the guidelines for executing and reporting IMI research.100 Trial results will be submitted for publication in a peer-reviewed journal and presented at conferences. Central results will be communicated to the DDS. External researchers may get access to the final trial dataset (from HB) on request depending on to be specified data security and data exchange regulation agreements. According to German law, data will only be shared with parties outside the project team in de facto anonymised form.
Ethics statements
Patient consent for publication
Acknowledgments
We kindly thank Ayla Aydin, Sofia Ring and Tim Dretzler for performing the allocation procedure. We kindly thank Lisa Biermann and Fabienne Schmid for collecting and informing possible participants about the study and for documenting the participant flow at baseline. We kindly thank Pauline Meyer for supporting the trial start and Ayla Aydin and Pauline Meyer for e-coaching participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @EileenBendig
Contributors ACTonDiabetes was developed by the Department of Clinical Psychology and Psychotherapy based on ACTonPain with a lead of EB at the University of Ulm. EB, AS, HB, BK and NH designed and planned the study. HB and EB supervised the study. AW and EB operatively performed the study. AS and AW enrolled the participants. EB drafted the manuscript, all other authors critically revised the work for important intellectual content (HB, AS, AW, BK, NH and MM). All authors (HB, AS, AW, BK, NH and MM) approved the final version to be published and agree to be accountable for all aspects of the work.
Funding This work was supported by the German Diabetes Foundation (Deutsche Diabetes Stiftung (DDS)), grant number FP-0431-2020 and budget funds (Grant no: N/A) of Department of Clinical Psychology and Psychotherapy, Institute of Psychology and Education, Ulm University, Germany.
Competing interests HB reports to have received consultancy fees and fees for lectures/workshops from chambers of psychotherapists and training institutes for psychotherapists in the e-mental-health context. NH reports fees for consultancy fees and fees for lectures/workshops from Novo Nordisk, Sanofi and Abbott. BK reports that he received consulting fees and fees for lectures and the preparation of the 'Digitalisation and Technology Report Diabetes' from Berlin Chemie AG. All other authors declare not to have competing interests.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.