Article Text

Abstract
Introduction The COVID-19 crisis has led to the adoption of strict and coercive preventive measures. The implementation of these measures has generated negative impacts for many communities. The situation is especially worrisome for Indigenous communities in Peru. Therefore, it is necessary to recognise the contribution of the experiential knowledge of Indigenous communities and to implement innovative approaches. The use of art can be a promising avenue for working in partnership with Indigenous communities.
The goal of this research is to (1) develop an intervention promoting barrier measures and vaccination to limit the transmission of COVID-19 among Indigenous communities using an arts-based and community-based knowledge translation and exchange (ACKTE) model; and (2) understand the contextual elements and mechanisms associated with the process of developing a preventive intervention using the ACKTE model.
Methodology and analysis This research will take place in Indigenous communities in Peru and will be based on a developmental evaluation guided by the principles of realist evaluation. Members of two Indigenous communities, local authorities, health professionals and artists will participate in the intervention development process as well as in the developmental evaluation. For data collection, we will conduct modified talking circles and semistructured individual interviews with stakeholders as well as an analysis of documents and artistic works produced.
Ethics and dissemination of results This research received the approval of the Université du Québec à Rimouski’s research ethics board. In addition to scientific articles, the results of this research will be disseminated through videos and during an artistic performance.
- PREVENTIVE MEDICINE
- QUALITATIVE RESEARCH
- COVID-19
- PUBLIC HEALTH
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitation of this study
By focusing on equity and engaging Indigenous communities, this project will promote shared problematisation and cocreation of interventions while promoting complementarity among science, art and local knowledge.
Developmental evaluation and realist evaluation are relevant and complementary for health research with Indigenous communities because they have congruences with Indigenous ontologies and perspectives.
Modified talking circle that will be conducted are a recognised data collection method in line with discussion methods used in Andean Indigenous communities.
Language and cultural barriers, the current pandemic context and the remoteness of targeted Indigenous communities may influence or delay data collection and analysis.
Introduction
The COVID-19 crisis has led all countries to adopt strict and coercive containment measures in order to reduce the transmission, morbidity and mortality associated with SARS-CoV-2, but without real intersectoral collaboration adapted to local realities.1–3 In Peru, as in other Latin American countries, a national state of emergency was declared, instituting restrictions on rights to personal freedom, security, inviolability of the residence and freedom of assembly and transit;4 enacting laws granting extensive powers to law enforcement officers and the military5 to enable the enforcement of a lockdown6 and leading to arrests and detentions by the military of those violating or protesting against preventive measures related to COVID-19.5 These measures have sometimes had negative consequences for many rural7 8 and Indigenous9–11 communities,3 thus contributing to increasing health inequities.11 12 This situation is worrisome in Latin American countries,13 including Peru,14 where Indigenous communities are disproportionately affected by COVID-19.15 16
In Peru, Indigenous people are four times more affected by COVID-19 than non-Indigenous people, and in some regions, the death rate is four times higher among Indigenous people.16 In addition to a health system ill-suited to the needs of Indigenous people,14 they had to travel outside of their territory to benefit from support measures during the pandemic, contributing to the spread of COVID-19 in their communities.17 Moreover, the imposition of barrier and coercive measures has exacerbated Indigenous communities’ historical fear and mistrust of public authorities.17–20
Although the involvement of communities is central to the prevention of infections,21 some public health authorities, faced with the urgency to act, have not always consulted them, taken their concerns into account or adapted preventive measures to their needs. This can lead to rejection of preventive measures, acts of violence18 and vaccination resistance.22 Considering the maintenance of preventive measures and the anticipated acceleration of the vaccination campaign in Peru, it is necessary to mobilise and integrate Indigenous experiential knowledge and cultural practices in the development of protection, promotion and prevention (PPP) interventions in health.23
Although existing community health models propose mechanisms for mobilising communities, their scope is limited in terms of adaptation to local contexts and ownership by Indigenous communities. Additionally, power inequalities, mistrust of authorities and previous negative experiences with consultation do not foster effective participation of Indigenous communities in the design, implementation and evaluation of health interventions for these populations.11 24 Rethinking the community-based knowledge translation and exchange (KTE) process to integrate approaches that are sensitive to local contexts and adapted to Indigenous realities is central to ensuring the effectiveness of interventions.
KTE by and for communities should be implemented in close collaboration with Indigenous communities, clinicians and decision-makers to increase the social acceptability of preventive measures as well as health and social benefits for communities.25 In the current pandemic context, decision-makers must involve Indigenous communities while respecting their rights to self-determination, health and equity. To achieve this, we propose mobilising artistic approaches sensitive to local realities and associating them with a KTE process inspired, codeveloped and driven by the communities.
Limitations of traditional KTE models among marginalised populations
Traditional PPP public health interventions during a pandemic are developed using a top-down approach, directly designed by certain key stakeholders and then applied in communities.26 These interventions integrate characteristics common to the general population and do not take into account the differentiated needs of various groups. The reach of these interventions is also limited by linguistic, socioeconomic and cultural barriers.27 28 The early involvement of local stakeholders, that is, potential knowledge users,29 30 the continuous presence of researchers in the environment and the development of concrete solutions that can be observed by communities29 are KTE success factors. In practice, KTE implementation has its share of challenges. Some national public health strategies do not always target the needs of Indigenous populations,29 and few implemented KTE approaches have demonstrated their effectiveness in terms of health equity and25 changing long-term user behaviour.31 32 In addition, although new models of community-based KTE are increasingly being developed and tested,25 33–36 there is little information on KTE processes specifically integrating tacit knowledge from communities.25 27 To be socially acceptable and beneficial to the health of communities, community-based KTE must be more flexible, dynamic and innovative to overcome barriers to involvement in the implementation of interventions.34 37 The integration of artistic approaches could help to bridge this gap.
Potential of artistic approaches to improve protection, promotion and prevention (PPP) interventions in public health
The use of artistic approaches for PPP in health promotes full community participation and diversity of perspectives,24 38 increasing social acceptability, encouraging community ownership and strengthening the sustainability potential of outcomes.39 Due to their participatory nature, artistic methods take into account sociocultural factors, involve all participants in an iterative process of action-reflection and bring about a new, in-depth understanding of the phenomenon studied,40 41 thus contributing to the empowerment of individuals and communities.42 In health science, building knowledge through an artistic process that makes it accessible to various audiences is increasingly recognised43 because the use of arts-based KTE approaches in health offers real opportunities for transformation.44 However, there is little scientific literature currently available to guide such a complex process.43
Research goal and objectives
The goal of this project is to study the process of implementing an arts-based and community-based knowledge translation and exchange (ACKTE) model and to generate rigorous knowledge to enable its replication in order to foster social acceptability and contribute to improving the health of Indigenous communities. More specifically, it will involve (1) mapping the artistic stakeholders and the cultural and artistic practices of the targeted Indigenous communities; (2) developing and implementing preventive intervention promoting barrier measures and vaccination to limit the transmission of COVID-19 in Indigenous communities based on an ACKTE model and (3) documenting the contextual elements and understanding the underlying mechanisms associated with developing an intervention using the ACKTE model.
Conceptual model of ACKTE
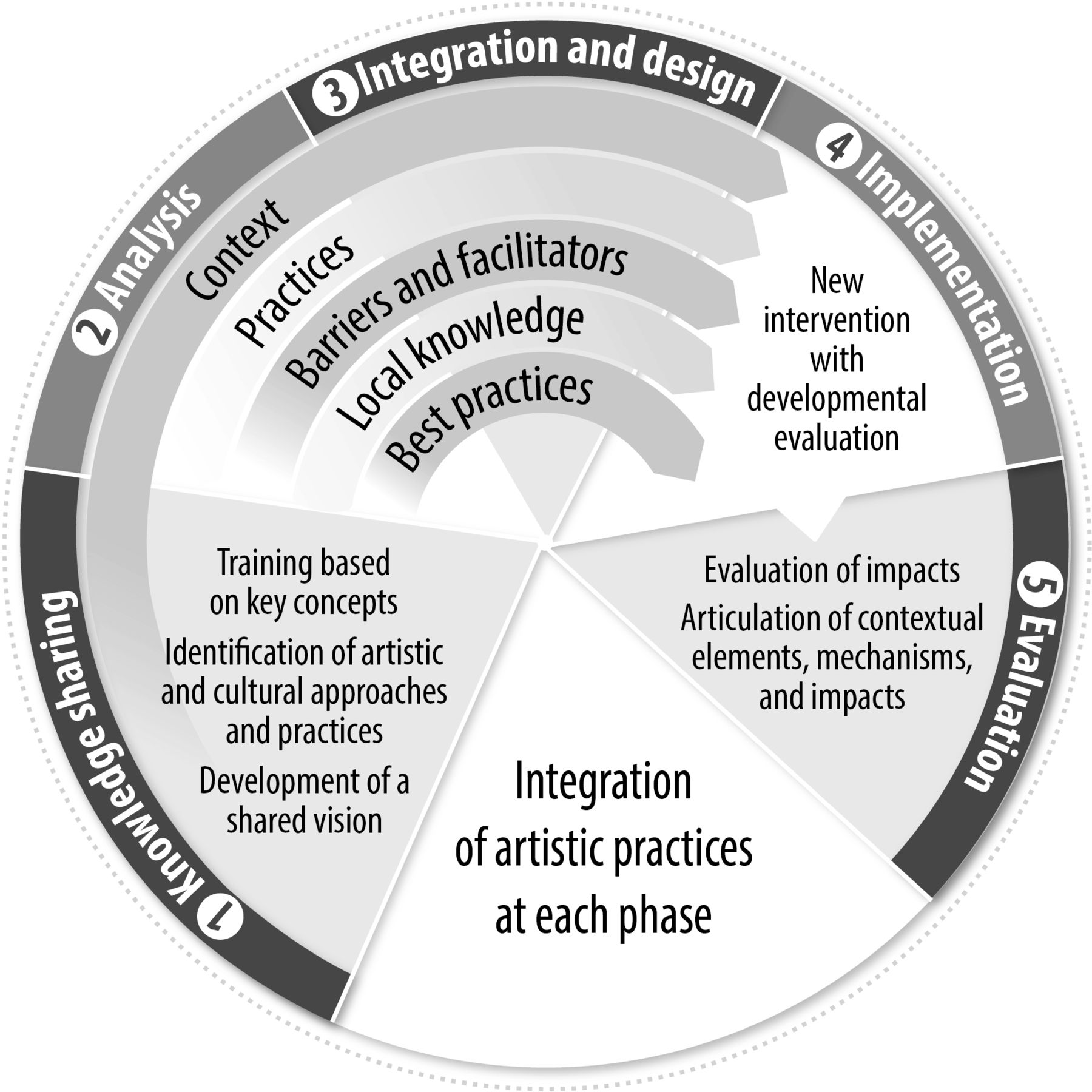
As part of previous reflective and theoretical work, many members of our team contributed to the development of the ACKTE model,45 which will be used to guide the conduct of this project (see figure 1). This model, inspired by Kontos and Poland’s conceptual framework on the use of the arts in KTE46 and Jenkins and collaborators’ reference framework for community-based KTE,36 was developed to promote dialogue between stakeholders and the full integration of their tacit knowledge in the KTE process.45 The ACKTE model is an integrated, community-based KTE model that uses the arts (techniques and tools) at different stages of the process: (1) knowledge sharing; (2) situational analysis; (3) integration and design; (4) implementation of interventions by and for communities and (5) evaluation of impacts. Given the time constraints, our project will not include the evaluation of impacts, but that of the processes.
{kind=link}
Visual representation of arts-based and community-based knowledge transfer and exchange (ACKTE) model. Source: Bergeron et al (2019).45
Methodology and analysis
This research project will be implemented in two rural Andean Indigenous communities from Quispicanchi Province, in the Cusco Region of Peru.47 These communities were selected because three members of the research team developed a partnership there during previous projects and continue to work with stakeholders from these communities. Descriptive data on the two participating communities are presented in table 1.
Descriptive data on the two participating rural Andean Indigenous communities
Summary of project phases and methodological approach
The project will take place over 12 months and consists of four distinct phases, some of which will be carried out concomitantly.
Phase 1—training of team members and local partners on the theoretical foundation
Members of the research team and local partners will be trained on the theoretical foundation to anchor and support a common multidisciplinary vision for the project. A first training will focus on the KTE process and the ACKTE model (carried out in collaboration with the InterS4 Consortium, a partnership between healthcare institutions and universities centred around a knowledge transfer and brokerage platform, focused on the organisation of local care and services in non-metropolitan areas). A second training will be developed on the types of artistic tools and approaches and their uses for the creation of new interventions. These trainings will be offered to research teams and local partners virtually, synchronously and asynchronously, in Spanish. A translated version will be available for people speaking Quechua.
Phase 2—mapping of cultural and artistic practices, review of practices to promote barrier measures and vaccination
Based on the reference framework developed by Evans and Foord,48 a mapping of local cultural and artistic practices and influential artistic stakeholders will be carried out in each of the targeted communities to identify the cultural initiatives that reach various generations in each environment. This mapping will make it possible to target cultural and artistic practices already present in the communities in order to reinvest them in the development of the intervention while preserving the cultural identities of the environments.49
In parallel with this rapid mapping, we will review practices for raising awareness of barrier measures and vaccination among populations and synthesise the most relevant evidence-based literature that can be applied to the contexts of rural Andean Indigenous communities.
Phase 3—cocreation of a public health intervention using the ACKTE model
The intervention cocreation process will be guided by an ACKTE model combined with a human-centred design (HCD) approach. This creative problem-solving framework is based on the philosophy that people facing specific challenges daily hold the key to their solution.50 According to the HCD, the participation of communities and local stakeholders in artistic creation processes promotes ownership and increases the likelihood that the resulting intervention will resonate more with its target audience.51 52 The intervention cocreation process will result from the collaboration between members of Indigenous communities, Peruvian and Quebecois artists, health professionals, local government employees and decision-makers and researchers.
We plan to carry out four artistic cocreation cycles that will ultimately serve to develop an intervention to promote barrier measures and vaccination against COVID-19 which will be implemented by the health centre responsible for the Quispicanchi health micronetwork. The cocreation cycles aim to leverage the local knowledge of Indigenous communities and integrate it into the practices identified in scientific literature to create a new intervention.
Phase 4—evaluation of the intervention design process
A developmental evaluation approach guided by the principles of realist evaluation (RE) will be used to evaluate the ACKTE-based intervention development process.
The developmental evaluation approach supports the deployment of social innovations in complex environments,53 including Indigenous communities.54 RE, a theory-based approach to evaluation, is also recommended for evaluating complex situations, as it makes it possible to relate the context and underlying mechanisms that can influence the effectiveness of a process in a given setting.55–57 Studies have shown that RE is relevant for health research with Indigenous communities because it is based on a holistic approach congruent with Indigenous ontologies.58
Development of an initial programme theory: prior to phase 3, an initial programme theory will be jointly developed with coresearchers and collaborators based on the ACKTE model45 and on a framework identifying the context and potential mechanisms,59 explaining the potential influence of contextual factors and underlying mechanisms on the intervention development process.
Sampling, participants and selection criteria
Participants will be recruited using purposive sampling. Four types of participants will be involved in the research project: (1) members of the two targeted Indigenous communities (minimum of six people per community, including one executive committee representative of each community’s asamblea comunal) (The asamblea comunal is a proximity-based political structure ensuring, in consultation with community members, the management of the common good in Indigenous communities in Peru); (2) health sector personnel providing care in the two target communities (minimum four professionals and two managers); (3) employees of the provincial municipality involved in the COVID-19 committee (minimum two representatives) and (4) people from the cultural community of Quispicanchi Province (artists, workers in the arts: at least two representatives). The only inclusion criterion will be to speak Spanish or Quechua while the exclusion criterion will be the presence of diseases or cognitive or sensory deficits limiting social interactions. The target sample size is 22 participants.
We will make sure to have an equal number of men and women among the participants and a majority of participants from Indigenous communities. In order to facilitate intergenerational exchanges within the two Indigenous communities, we will recruit participants from various age groups, including young adults and elders. Considering that Spanish is not the language spoken in the targeted Indigenous communities, all the discussions will be carried out in Quechua in addition to Spanish, to allow the full participation of members from Indigenous communities (at least two local research assistants will be fluent in Quechua).
Participant recruitment process
Before the start of phase 2, a meeting will be held with members of each community and the people working in the other institutions involved in the research project (health centre and provincial municipality) to present the research project and the different stages. At the end of these meetings, people wishing to participate in the research project will be invited to meet a research assistant who will be able to answer their questions and provide them with the information and consent form for signature.
Data collection
Data collection will take place during three of the four phases of the project (phases 2, 3 and 4). The data collection process for each phase is described below and summarised in table 2.
Approaches and data collection methods for each phase of the project
Phase 2—mapping of cultural and artistic practices
The mapping of cultural and artistic practices will be carried out using semistructured interviews of approximately 15–30 min in Spanish or Quechua conducted by a research assistant with all the participants. Interviews will be conducted using an identification chart for cultural and artistic practices, and the questions will focus on artistic and cultural practices, places, events and artists present in the targeted Indigenous communities.
During this phase, a short sociodemographic questionnaire will be completed individually by the participants to obtain data on place of residence, gender (female, male and non-binary), marital status, religious practice, number of children and occupation. For illiterate persons, the questionnaire will be completed with the support of a research assistant. We will keep this information strictly confidential.
Phase 3—cocreation of a public health intervention using the ACKTE model
As previously mentioned, at least four artistic cocreation cycles will be carried out in phase 3. These cocreation cycles will be facilitated by local artists and will bring together different types of participants. For each cocreation cycle, participants will be divided into groups of up to eight people to facilitate interactions. Indigenous participants will make up the majority of each group. The choice of the location for the cocreation cycles will be made by the members of the Indigenous communities so that they can choose a place where they feel safe. Each cycle will include group discussions—that we will refer to as group dialogue—led by the artist guiding the cocreation to foster openness and exchanges between participants.60 Each cycle will begin with an initial discussion, followed by another at the halfway mark during the coffee break, and then a final one to close the cycle. The discussion points in each of the cocreation circles will be related to the objective of each circle and the participants’ perceptions of that objective.
The artist who will facilitate the cocreation cycles will provide an inclusive, safe and rewarding environment so that all participants feel able and comfortable to share their opinions and contribute to the current creation project. Therefore, it will be essential that the artist–facilitator establish a dynamic that promotes everyone’s participation and respectful listening during the group dialogues.60 The researchers will train the artist in dialogic principles that promote sharing and reciprocity within the group.61
Various techniques will be used and artistic activities will be chosen collaboratively with the communities following the mapping of cultural and artistic practices. These include stories (drawn, narrated, sung or filmed), visual art projects inspired by local practices and intervention theatre. They will mostly be led by the participants and will adapt to their own cultural codes while featuring local knowledge. With the consent of the participants, the artistic products produced will be archived and considered qualitative data.
The main objective of the first two cocreation cycles will be to analyse the context of the target Andean Indigenous communities, current practices for promoting vaccination among Andean Indigenous communities, as well as the barriers and facilitators that may affect the implementation of a new vaccination promotion intervention. The subsequent cocreation cycles will aim to explore local knowledge in health promotion and identify avenues for integrating local knowledge and best practices (identified during phase 2) to design a new vaccination promotion intervention adapted to the context of target Andean Indigenous communities and taking into account existing barriers and facilitators.
Phase 4—evaluation of the intervention design process
During the phase 3 cocreation cycles, we will conduct a real-time collection and analysis of useful data for rapid feedback to the research team to enhance project implementation.53 62 Two research assistants will conduct participant observation sessions during the cocreation cycles. During participant observation sessions, the research assistants will observe specifically the exchanges and dynamics among different types of participants and between the participants and the artists, noting the factors that may explain the exchanges and dynamics. The research assistants will not have any verbal exchanges with each other during the cocreation cycles. Each observer will individually complete an observation table in Spanish at the end of the sessions.
After each cocreation cycle, a modified talking circle will be conducted with members of the Indigenous communities63—as these circles are a recognised data collection method in line with discussion methods used in Andean Indigenous communities64—and one with non-Indigenous participants. A few days after the modified talking circle, additional semistructured individual interviews could be conducted with some members of the Indigenous communities or non-Indigenous participants to further explore the themes that emerged during the modified talking circles.
The interview guide for modified talking circles will be refined throughout the project. Evaluative questions associated with the process evaluation will be identified by stakeholders and integrated into the interview guide. For additional semistructured individual interviews with members of Indigenous communities or non-Indigenous participants, the interview guide will be developed following the preliminary analysis of the previous modified talking circle.
A research assistant will conduct modified talking circles and interviews in Spanish or Quechua, according to the preference of the participants. Modified talking circles and interviews will be recorded with the consent of participants. Considering that the developmental evaluation approach aims to support the development of the intervention, feedback loops will also be conducted regularly with the participants and the research team during the project53 62
Data analysis
Data collection and analysis will be iterative and non-linear.65 A directed content analysis approach66 adapted for RE67 will be used. A semiopen analysis chart developed from the initial programme theory will enable causation coding.68 Memos related to the identification of the links between the concepts will be written during the coding69 and coding will be performed based on the Spanish version in collaboration with a research assistant from a local Indigenous community.70 For artistic works, there will be a formal analysis (including identification of the characteristics and objects represented or described) and a conceptual analysis (including the symbolic imagery and affects expressed).71 Data interpretation will be supported by verbatim transcripts68 and artistic works.72 Matrix queries will be produced with NVivo V.12 to explore recurring trends in the data73 and identify connections.74 Real-time data collection and analysis53 62 will make it possible to refine the initial programme theory on an ongoing basis.75–77 The preliminary results will also be validated with Indigenous community members participating in the project.
Sex and gender considerations
Sex and gender will be considered during the recruitment of participants, collection and analysis of data and dissemination of results.78 For this project, gender is an intersectional concept consisting of multiple gender identities and distinct lived experiences of communities.79 Therefore, the project aims to create a safe space where community members with gender-diverse identities can express themselves freely.
We are aware that the colonial legacy has profoundly transformed the relationship of Indigenous communities in Peru with the concept of gender from a conception that includes a third gender with a sacred role to a binary conception.80 In Peru, people who identify with diverse gender identities experience various forms of violence,81 82 which makes the process of accepting their own identity difficult.82 We will increase awareness of gender diversity and inclusive practices among all members of the research team. A statement will be made that this project is an inclusive space, and group rules will be established by the participants at the beginning of the project. The statement and group rules will be reiterated at the beginning of each cocreation circle.
For the qualitative data analysis, we will verify whether any specific themes emerge from the data according to the gender of the participants.83 Furthermore, one of the approaches retained (RE) will allow us to identify patterns in contextual factors and underlying mechanisms influencing the participation of members of Indigenous communities according to gender84 during the implementation of the ACKTE model. Finally, considering that researchers, collaborators and partners could have unconscious biases regarding sex-related and gender-related issues, a sustained effort will also be made throughout the research process to address these issues.85
Patient and public involvement
This research project stems, in part, from planning and dissemination work (funded by the Canadian Institutes of Health Research) that was conducted in 2018 with members of the Indigenous communities participating in this research project. This planning and dissemination work allowed the identification of health promotion research priorities for the communities.86 The research questions and objectives as well as the study design were developed in collaboration with an indigenous coresearcher from one of the communities. As a community-based project, participants will be involved throughout the study.
Framework for the use and dissemination of artistic processes
In partnership with executive committees of the Indigenous communities’ asambleas comunales, we will develop a local framework agreement regarding copyright and intellectual property rights. This signed agreement will define the framework for the use of artistic processes used in the project and all of the shared expertise will be used within this framework. Any other usage not included in the initial agreement must be authorised by all of the executive committees of the Indigenous communities’ asambleas comunales. The agreement will also specify that the expertise, works created and resulting research data shall not be used for any purpose or in any setting that is disparaging or defamatory, invades individuals’ privacy, is obscene, abusive or threatening or violates applicable intellectual property laws or any other applicable law. Clear ethical rules regarding the respect and protection of personal data and cultural or intellectual property rights will be established in partnership with the executive committees of each Indigenous community’s asamblea comunal at the start of the project. All of the above-mentioned documents will be available in French, Spanish, and Quechua.
The artistic works produced during this project will be archived and may only be displayed at artistic events with the consent of participants. The display methods will be specified in the agreement signed with the asambleas comunales executive committees.
Set up of an advisory committee
An advisory committee composed of members of Indigenous communities (two men and two women from each community, including at least one member from each community’s asamblea comunal executive committee) will be set up to identify and discuss potential blind spots, biases and culturally sensitive issues. This committee will attend a virtual meeting with the research team at least once every 2 months.
Ethical considerations and dissemination of results
Ethical considerations
The research protocol was approved in Canada by the Université du Québec à Rimouski’s research ethics committee (project# CÉR-117-919) and in Peru by the Universidad Nacional San Antonio Abad del Cusco’s research bioethics committee (CBI-UNSAAC-2021-005). All participants will be required to sign an information and consent form before participating in the study. During recruitment, no undue pressure will be put on people to participate in the project.
Hard copies of research files will be kept in Peru, while digital data will be stored in a secure cloud-based file accessible only to research team members. Research files and data will be kept for a period of 5 years following the publication of results. Only the principal investigators will have access to data that can identify participants such as the information and consent forms and the code key.
In order to preserve the identity of participants and ensure confidentiality, participants will be identified by a code number and data will be decontextualised. No publication or scientific communication will contain data that could identify participants. Individuals who agree to be filmed or to have their artistic works displayed may be identified and it may not be possible to fully ensure confidentiality.
Dissemination of results
A workshop including an artistic performance (in Quechua and Spanish) will be held to present the results to participants and civil society stakeholders. We will invite an equal number of men and women to this workshop. Two videos (available in Quechua, Spanish, French and English) presenting the ACKTE model as well as its operationalisation and potential uses will also be produced and posted during the project (on the websites of collaborating institutions and social media). Only people who have consented to be filmed for these videos will be visible.
Expected outcomes
This project will contribute to reflections on the relevance of KTE, and ACKTE model specifically, in the implementation of public health interventions during a pandemic. We believe that the innovative nature of our interventions based on transmitting health knowledge through artistic creation may encourage future initiatives combining art and community health. The project will also enable the implementation of a participatory and interdisciplinary approach favouring a common problematisation and the cocreation of interventions while balancing and fostering complementarity between science, art and local knowledge.87 From a practical point of view, this approach could be replicated for the resolution of complex issues affecting Indigenous communities by creating an environment conducive to exchange and dialogue. These results could guide actions to improve the deployment of KTE in collaboration with Indigenous community stakeholders and provide alternative models to develop preventive interventions against COVID-19. Moreover, the intervention model that we will codevelop with the communities will foster a sense of belonging, recognition and empowerment among participants. More generally, given the need in Latin America to conduct more research in partnership with vulnerable groups or communities and to facilitate stakeholder participation,88 we also believe that the ACKTE model could be replicated in different settings in the region to facilitate the KTE process and foster the full integration of local community knowledge in the development of new health interventions.
By focusing on equity and mobilising Indigenous communities in the development of interventions integrating evidence-based data and local knowledge, we believe that this project has the potential to transform KTE practices in health. At the end of this research project, knowledge that can be used for community-based KTE actions and decision-making will be produced, which will enable its translation to similar contexts, at local, national and international levels.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to acknowledge the Canadian Institutes of Health Research and the Collectif de recherche sur la santé en région (CoRSeR) for the financial support. We would also like to thank the members of the indigenous communities of Callatiac and Urin Ccoscco, Dani Miriam Tardif, David Buetti, Dioni Gabriela Cavassa Berrío, Vilma Apaza Quispe, Raimunda Ccoyo Quispe, Marivel Yauri Zea, Niel Wilson Ccanahuire Saire, Rolando Levita Humani, Jairo Alexis Morveli Quispe, Gueu Sylvain Deli, Xavier de Léséleuc, Hélène Desperrier and Louise Marquis of Théâtre Parminou, Joel Sack Roque Roque of the Gerencia Regional de Salud—Cusco, Emmanuelle Jean of the Consortium InterS4 and Teresa Chong Campos of the Dirección Desconcentrada de Cultura de Cusco for their help and advice.
References
Footnotes
Contributors DAB, LR, FMS, AMM and FCL contributed to the development of the study design. DAB, LR, FMS and AMM were involved in the research protocol development. DAB is responsible for the drafting of this paper, although LR, FMS, AMM and FCL have read and approved the final version.
Funding This work is supported by the Canadian Institutes of Health Research through an Operating Grant for Emerging COVID-19 Research Gaps and Priorities-Indigenous Health Research (grant number: GA7-177786) and by the Collectif de recherche sur la santé en région (CoRSeR) of Université du Québec à Rimouski.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.