Article Text

Abstract
Objectives To compare opioid prescription rates between patients enrolled in coordinated ambulatory care and patients receiving usual care.
Design In this retrospective cohort study, we analysed claims data for insured patients with non-specific/specific back pain or osteoarthritis of hip or knee from 2014 to 2017.
Setting The study was based on administrative data provided by the statutory health insurance fund ‘Allgemeine Ortskrankenkasse’, in the state of Baden-Wurttemberg, Germany.
Participants The intervention group consisted of patients enrolled in a coordinated ambulatory healthcare model; the control group included patients receiving usual care. Outcomes were overall strong and weak opioid prescriptions. Generalised linear regression models were used to analyse the effect of the intervention.
Results Overall, 46 001 (non-specific 18 787/specific 27 214) patients with back pain and 19 366 patients with osteoarthritis belonged to the intervention group, and 7038 (2803/4235) and 963 patients to the control group, respectively. No significant difference in opioid prescriptions existed between the groups. However, the chance of being prescribed strong opioids was significantly lower in the intervention group (non-specific back pain: Odds Ratio (OR) 0.735, 95% Confidential Interval (CI) 0.563 to 0.960; specific back pain: OR 0.702, 95% CI 0.577 to 0.852; osteoarthritis: OR 0.644, 95% CI 0.464 to 0.892). The chance of being prescribed weak opioids was significantly higher in patients with specific back pain (OR 1.243, 95% CI 1.032 to 1.497) and osteoarthritis (OR 1.493, 95% CI 1.037 to 2.149) in the intervention group.
Conclusion Coordinated ambulatory healthcare appears to be associated with a lower prescription rate for strong opioids in patients with chronic musculoskeletal disorders.
Trial registration number German Clinical Trials Register (DRKS00017548).
- GENERAL MEDICINE (see Internal Medicine)
- Back pain
- Health & safety
Data availability statement
Data are available upon reasonable request. Data are available upon reasonable request and can only be used in cooperation with the authors and the AOK health insurance.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The strengths of the study include the use of real-world data from multiple healthcare sectors and the large number of patients included in the analysis.
Advanced statistical modelling (generalised linear regression models) was used to analyse the intervention effect.
Logistic and negative binomial regression models were used, depending on the outcome variable.
Our analysis relies on the assumption that the claims data—that is, coding quality, data availability and data transfer—are of high quality.
Clinical information, as well as information on pain levels, functional impairment and patient preferences, were not available.
Introduction
Musculoskeletal diseases account for a high burden of disease1 2 and are common among older and multimorbid patients.2–4 Pain management is a cornerstone of symptomatic treatment in patients with back pain and osteoarthritis (OA).5 Although conservative treatments and exercise interventions that take a biopsychosocial approach6 are gaining importance,7 pharmacological pain management is still common in patients with chronic musculoskeletal diseases.8 Precaution should be taken when managing pain in these patients, especially since they are usually taking other medications, which may increase the risk of harmful interactions or side effects. Once patients with chronic musculoskeletal conditions are accustomed to pain medication, it is difficult to manage the disease by non-pharmacological means. It is also known that prolonged opioid use can lead to habituation and the need for more and stronger analgesics,9 which can produce both dependency and decreased quality of life.10 Unlike several other countries, there is no immediate risk of an ‘opioid epidemic’ in Germany.11 However, although opioid treatment is not strongly recommended in patients with OA,5 the number of prescribed opioid analgesics and their long-term usage in Germany rose between 2006 and 2010.12
Healthcare strategies that increase the role of non-pharmacological conservative treatments and reduce pharmacological treatment in patients with chronic musculoskeletal disorders should therefore be considered. These strategies have already proven themselves to be beneficial, for example, multidisciplinary treatment was found to be more effective in reducing pain intensity than no treatment and active treatment/exercise interventions.12 However, studies on single interventions are rare, and most studies investigate the effects of complex interventions.13 Participation in similar healthcare programmes to the one we are considering here is associated with raising the appropriateness of pharmacological treatment for common diseases like diabetes and cardiovascular diseases.14 15 In this study, we evaluated a healthcare programme for patients with musculoskeletal disorders in southern Germany to see whether structured coordinated collaborative care involving general practitioners (GPs) and orthopaedists is associated with differences in opioid prescription rates.
Methods
Study design and setting
We carried out a retrospective observational cohort study based on administrative data provided by the statutory health insurance fund ‘Allgemeine Ortskrankenkasse’ (AOK), in the state of Baden-Wurttemberg, Germany, for the years 2014–2017. In the study period, Baden-Wurttemberg had about 11.1 million inhabitants. AOK, the largest health fund in the state, provided health insurance to around 40% of the insured population, or 5.1 million persons.16 17 In 2016, about 550 orthopaedic surgeons who provide outpatient care, and 350 000 patients insured with AOK, had enrolled in the collaborative orthopaedic care programme.18
Intervention
Coordinated ambulatory healthcare
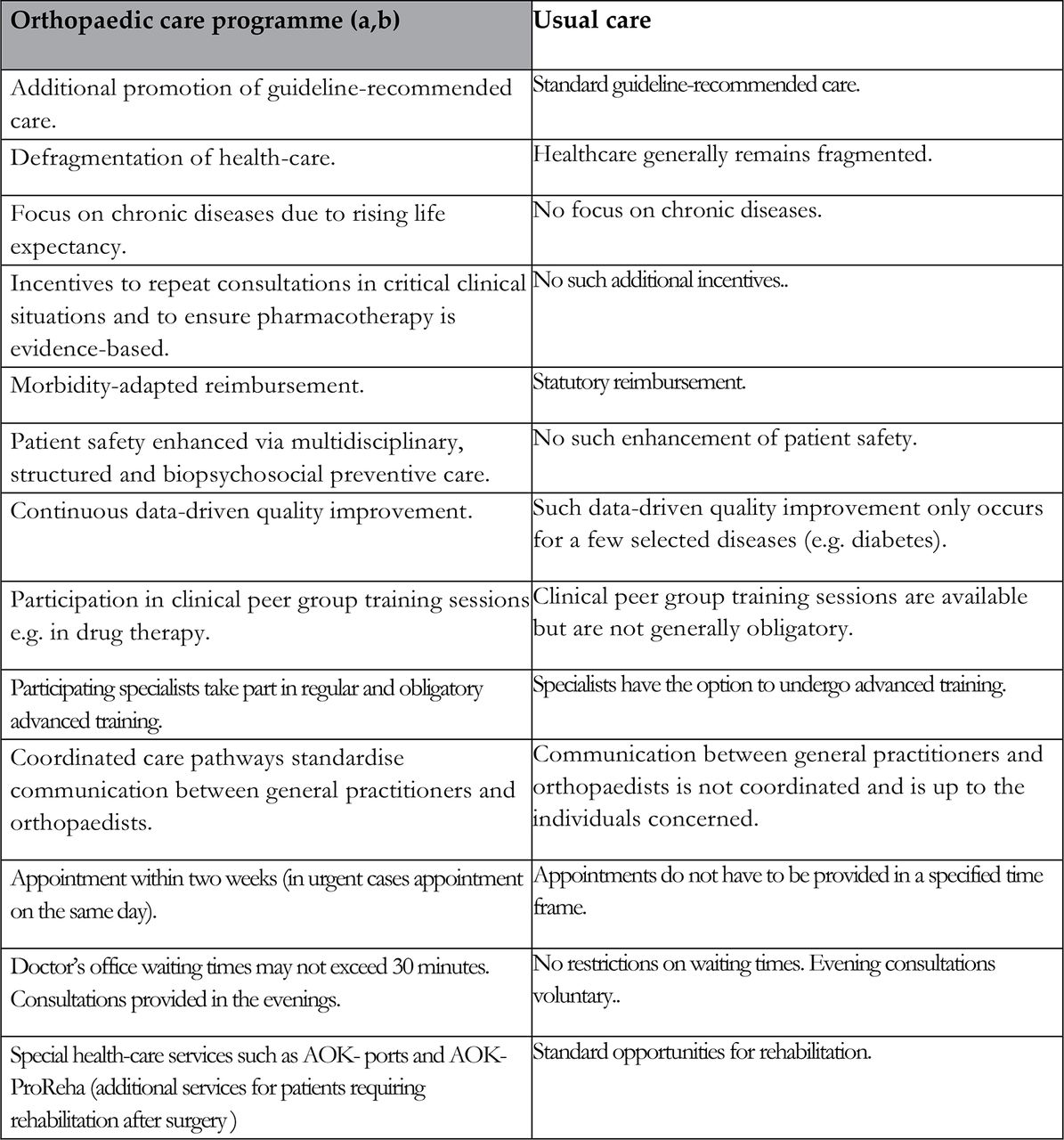
The coordinated ambulatory healthcare referred to here is the orthopaedic collaborative care programme in Baden-Wurttemberg. It was launched in 2014 for outpatients with specific and non-specific back pain, OA of hip and knee, osteoporosis and rheumatoid arthritis.19 Further details and the legal framework can be found in the German Social Code, Book 5 §73c. The contracting partners in the programme are AOK, Bosch BKK (health insurance), MEDIVERBUND AG (controlling service), BVOU (Professional Association of Orthopaedic Specialists and Orthopaedic Surgeons), BNC (Federal Association of Surgeons), BDRh (Federal Association of German Rheumatologists) and Rheumaexperten BW eG (an association of practices specialising in rheumatology). Participation is voluntary for both physicians (GPs, orthopaedists and orthopaedic surgeons in private practice) and patients. However, participants had to have previously enrolled in the GP-centred healthcare programme20 in which the orthopaedic programme is embedded.14 21 The GP-centred programme is available throughout the study region. Patients wishing to enrol are required to first consult their GP, who will refer them to a specialist where necessary and coordinate further treatment. The GP is not only involved in the referral stage but continues to support patients while they are receiving treatment from specialists. Participating physicians share clinical and other patient information with their colleagues electronically to ensure information is not lost. Regular quality circles on drug therapy (ie, small groups of physicians who receive feedback on their prescribing behaviour, evidence-based information and suggestions for improvements)14 and continuous data-driven quality improvements are features of the programme’s quality management. Compared with usual care, patients profit from shorter waiting times for appointments and higher continuity of care.21 Furthermore, in the orthopaedic collaborative care programme, orthopaedists are encouraged to take more time for consultations, discuss difficult cases with, for example, social workers, and to offer exercise interventions. All of these aspects are found in usual care as well, but are not incentivised. In Germany, usual care gives patients the right to seek care from GPs and orthopaedists independently. Although most consultations with orthopaedists follow a GP’s referral, it is worth noting that referrals are not incentivised in usual care. An overview of the differences between the orthopaedic collaborative care programme and usual care is shown in figure 1.
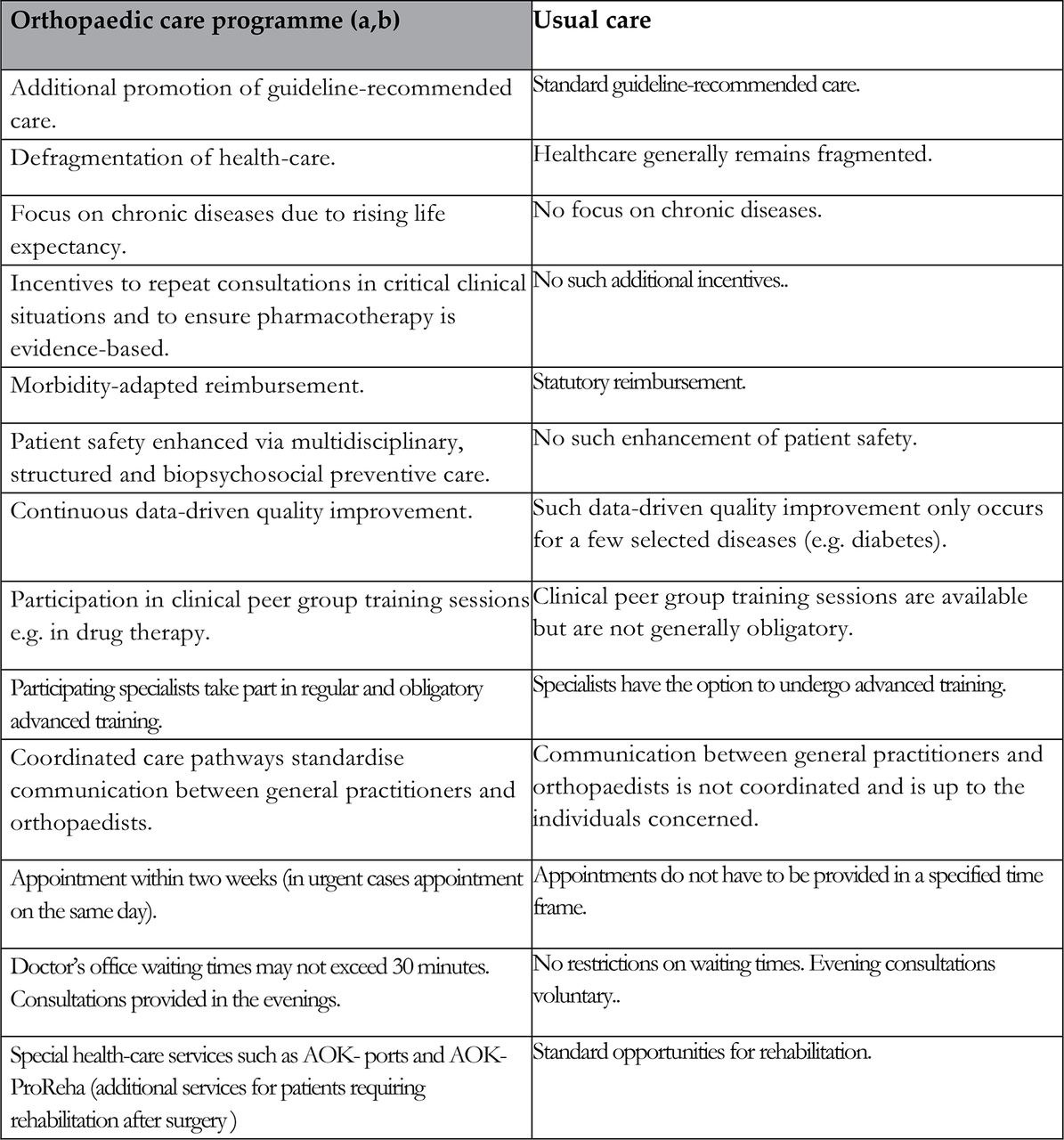
Special characteristics of the orthopaedic care programme as compared with usual care. (a)https://www.aok.de/pk/bw/inhalt/facharztprogramm-orthopaedie/ (b)https://www.aok.de/pk/fileadmin/user_upload/AOK-Baden-Wuerttemberg/05-Content-PDF/aokbw-facharztprogrammf-flyer-englisch.pdf.
Participants
Participants were selected according to their insurance status, relevant diagnoses and availability of International Classification of Diseases (ICD-10-M). Patients who fulfilled the following criteria were included: diagnosis of hip or knee OA (ICD-10-code M16.0–16.7 or M17.0–17.5) or back pain (online supplemental file 1), uninterrupted health insurance, residency in Baden-Wurttemberg and aged over 18 years. We included patients who were diagnosed with OA or back pain in the first or second quartiles of 2016. To be considered as patients with chronic musculoskeletal disorders, they were required to have been additionally diagnosed with OA or back pain in 2014 or 2015. We excluded patients who were diagnosed with any type of malignancy (online supplemental file 1), as they were most likely to receive opioids for the underlying disease and would probably require stronger pain medication than patients without cancer. This was also necessary because information on the precise indication for pain medication was unavailable. Baseline characteristics of patients and relevant comorbidities were assessed during the baseline period in 2015 and are presented in table 1.
Supplemental material
Baseline characteristics for all cohorts
The intervention group included patients who had enrolled in the orthopaedic care programme at any time during the study period, and who had consulted an orthopaedist enrolled in the programme. Contact with the orthopaedist was operationalised using the corresponding billing code. The control group included patients who had not enrolled in either the orthopaedic programme or the GP-centred care programme, and who had consulted an orthopaedist who was not enrolled in the programme.
Patients who switched groups during the observation period were excluded, as were patients who had enrolled in GP-centred care but not in the orthopaedic care programme, and who had consulted an orthopaedist who provided usual care. Inclusion and exclusion criteria and a detailed description of the study population are displayed in figure 2. Patients may have been diagnosed with more than one disease, for example, back pain and OA. In this particular case, they would appear in both the back pain and the OA cohorts. Patients in the non-specific back pain cohort may later have been diagnosed with specific back pain. All patients provided their written informed consent before participation in the programme.

{kind=link}
{kind=link}
Inclusion criteria for study groups. AOK, Allgemeine Ortskrankenkasse.
Reports on this observational study were prepared in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology statement and the German reporting standard for secondary data analysis.22
Outcomes
Outcomes were assessed between 1 July 2016 and 31 December 2017 (six quartiles). We assessed prescription rates for strong and weak opioids based on the WHO analgesic ladder.23 Strong opioids were defined as those used to treat strong to moderate pain and weak opioids as those used to treat moderate to weak pain. The Anatomic Therpeutic Chemical (ATC) codes are shown in table 2.
ATC codes
To confirm the correct implementation of the healthcare programme, we observed the rate of uncoordinated contacts to an orthopaedist in private practice, as well as the continuity of orthopaedic care. Uncoordinated contacts were defined as those that occurred without prior referral by a GP, and continuity was operationalised by quartiles in which an orthopaedist was consulted at least once.
All measures were based on routinely available claims data. This study is part of an evaluation of the entire orthopaedic care programme, in which further outcomes are being assessed.
Statistical analysis
Initially, all target and influencing variables were analysed descriptively. The number of non-missing values, mean, standard deviation (SD) and median was specified for continuous variables, and absolute and relative frequencies calculated for categorical variables.
Generalised linear regression models were used to analyse the intervention effect. The group variable and other covariables (potential confounders) were included in the model as fixed effects. Logistic and negative binomial regression models were used, depending on the outcome variable. Results were presented as ORs for binary variables and rate ratios (RRs) for count variables, with 95% CIs and two-sided p values (<0.05).
The selection of covariables was based on the advice of experts, current literature24–27 and previous experience.28 The Charlson Comorbidity Index (CCI) score29 in combination with level of care (extent of need for nursing care) was used to adjust for comorbidities and frailty. High-prevalence diseases and common comorbidities30 were also included when they were not covered by the CCI. The following covariables were chosen for the model: age, sex, participation in a disease management programme, CCI, level of care (>0), cardiovascular diseases, diabetes, stroke, malignancy, obesity, depression, psychosocial risk factors (ICD-10 codes: Z55.—Z65.-), burnout, smoking, somatoform disorders (ICD-10 codes: F45.-, F54.- and F62.8) and a history of disease-related healthcare utilisation at baseline. The history of disease-related healthcare utilisation was operationalised using the musculoskeletal-disorder-prior-to-observation (MDPTO) score. The MDPTO score is a non-standardised score we developed and used in the model to approximate the level of musculoskeletal disease prior to the observation period. The score takes into account the following factors during the pre-observation period: hospitalisation related to a musculoskeletal disorder, diagnosis of musculoskeletal disease, sickness note for a musculoskeletal disorder, prescription of physical therapy or aid, and use and prescription of an opioid.
All descriptive and comparative analyses were carried out in accordance with Good Practice in Secondary Data Analysis,31 using SAS (V.9.4) and IBM SPSS Statistics (V.25).
Patient and public involvement
The study design was based on our experience in the analysis of claims data from statutory health insurance funds. Patients were not directly involved in designing the study. We interpreted claims data in cooperation with various GPs in order to ensure that we were at all times aware of the influence of differing patient circumstances. We communicated the results to the health insurance fund and our cooperation partners, who will inform the patients and disseminate relevant findings online.
Results
Overall, 18 787 patients with non-specific back pain, 27 214 patients with specific back pain and 19 366 patients with OA were assigned to the intervention group, and 2803 patients with non-specific back pain, 4235 patients with specific back pain and 963 patients with OA to the control group. Patient characteristics are displayed in table 1.
Coordinated ambulatory healthcare
In all cohorts, coordination and continuity of care was significantly higher in the intervention group. For detailed results, see table 3.
Results for coordination of care
Opioid prescriptions
Descriptive data: 16.1% of patients with non-specific back pain were prescribed opioids in the intervention group, and 13.8% in the control group. Of patients with specific back pain, 20.3% were prescribed opioids in the intervention group and 17.0% in the control group. In patients with OA, 21.8% were prescribed opioids in the intervention group and 20.6% in the control group.
There was no significant difference in overall opioid prescription rates between groups (values for the control group are presented first). The number of overall opioid prescriptions in patients with non-specific back pain was 0.7±3.1 vs 0.8±3.0 (RR: 0.942, 95% CI: 0.810 to 1.095); the number of overall opioid prescriptions in patients with specific back pain was a non-adjusted 0.9±3.1 vs 1.1±3.8 (RR: 0.971, 95% CI: 0.870 to 1.082); the number of overall opioid prescriptions in patients with OA was a non-adjusted 1.1±3.2 vs 1.2±3.9 (RR: 1.064, 95% CI: 0.860 to 1.316). Results of the descriptive and multivariable analysis for strong and weak opioid prescription are displayed in table 4.
Results of the multivariate analysis for strong and weak opioid prescriptions
Discussion
Our investigation revealed that strong opioids were prescribed significantly less often and weak opioids significantly more often in all intervention groups, except for the non-specific back pain group, in which there was no significant difference in prescriptions of weak opioids. Since participants’ clinical circumstances were unknown, the correlation between participation in coordinated healthcare and the replacement of strong with weak opioids can only be taken to indicate that the non-pharmacological treatment offered in the programme may help mitigate pain to such a degree that weak opioids are sufficient to control symptoms. One possible explanation of this is that coordinated healthcare may encourage physicians to adhere to the WHO analgesic ladder scale and prevent them from prescribing stronger painkillers before treatment with weaker analgesics has proven insufficient.32
The main goal of the orthopaedic care programme is the implementation of guideline-oriented care for patients with musculoskeletal disorders in an outpatient setting by, for example, enhancing biopsychosocial anamneses and strengthening motivational consultations. Patients enrolled in the programme may thus profit from both the coordination of care and improved therapeutic strategies. Financial incentives for extended consultation times are intended to encourage physicians to practise evidence-based medicine and to empower their patients. Boosting the use of non-pharmacological and non-surgical treatments is considered a cornerstone of the programme. However, we did not assess whether consultation quality differed between groups.
This is the first study to describe opioid prescription rates for a study group enrolled in coordinated care in Germany. Data on the prevalence of opioid treatments in Germany are sparse,33 but the opioid prescribing process is specific to Germany33 and was identical in both our study groups. It should be noted that in 2010, M54 was the most common pain diagnosis to be treated with weak or strong opioids in Germany.34 The authors of that study noted an increasing trend in the number of opioid prescriptions, and that one-third of all opioid prescriptions were issued for back-related pain.34 Furthermore, 13.1% of patients with non-specific back pain were prescribed mild opioids and 4.8% strong opioids.34 These numbers are consistent with our findings (14.3% received either weak or strong opioids). Other reports on the prevalence of strong opioid prescriptions indicate that Baden-Wurttemberg is the German state with the lowest number of defined daily doses.35 Prescription rates on a national level can therefore be expected to be higher than those described in our study.
The strengths of the study are based on the use of real-world data from multiple healthcare sectors and the large number of patients included in the analysis. This, in turn, allowed us to perform advanced statistical modelling. The review period was chosen after the programme had been implemented for almost 2 years. It can therefore be assumed that the programme had been fully implemented when our observations took place. Furthermore, the observation period of six quartiles minimised seasonal effects on healthcare utilisation, as well as bias resulting from changes in coding regulations. Avoidance of contamination of study groups by excluding non-enrolled patients who had consulted an enrolled orthopaedist is an additional benefit. Correspondingly, we also excluded patients who were enrolled in the programme but had consulted an orthopaedist who was not. The high participation of orthopaedists in the programme (the majority of orthopaedists in private practice in the study region is enrolled in the programme) may explain the relatively few observations in the control group. Additionally, to be eligible for the control group, patients were not permitted to have enrolled in both the orthopaedic care and GP-centred care programmes, but to have consulted an orthopaedist offering usual care. Nonetheless, it is impossible to determine whether the observed effects reflected enhanced orthopaedic, enhanced primary care or perhaps bias, as mentioned below. Furthermore, we did not assess whether the GP or the orthopaedist prescribed the medication.
The limitations of secondary data analysis based on insurance claims data have been described in previous evaluation studies.36 37 Our analysis relies on the assumption that the claims data—that is, coding quality, data availability and data transfer—are of high quality. Clinical information, as well as information on pain levels, functional impairment and patient preferences, were not available. Furthermore, despite an extensive set of covariables, bias due to unmeasured confounders cannot be ruled out.
Since patients and doctors participated in the programme voluntarily, we cannot rule out self-selection bias in both GP-centred and orthopaedic care. Patients who enrolled in the programme may therefore have been more adherent and consequently more likely to benefit from consultation-oriented therapeutic strategies. It is further possible that the intrinsic motivation behind the decision of GPs and orthopaedists to participate in the healthcare programmes resulted in improved healthcare. Medication could not be assessed specifically for back pain or OA, which means it is possible that patients observed in our study received analgesics for other conditions. Additionally, as we did not analyse clinical data and do not know what occurred during consultations, it is difficult to assess how specific factors contributed to our observations. Besides differing patient characteristics, health service, service level and social backgrounds may also have influenced whether patients decided to enrol in the orthopaedic collaborative care programme. It should also be borne in mind that these factors may also have affected prescription patterns. It is to be hoped that qualitative studies aimed at assessing and, if possible, measuring the effects of consultations, along with randomised controlled trials applying core outcome sets,13 provide further insights.
Conclusion
Enrolment in the orthopaedic collaboratory care programme appears to be associated with a lower chance of being prescribed strong opioids in patients with chronic musculoskeletal disorders. As opioids can have severe adverse effects and lead to dependency, strategies improving prescribing patterns and thereby enhancing patient safety should be further investigated.
Data availability statement
Data are available upon reasonable request. Data are available upon reasonable request and can only be used in cooperation with the authors and the AOK health insurance.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Goethe University Ethics Committee (reference number: 338/18). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We wish to thank Phillip Elliott for editing the manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Deceased December 2021
Contributors KK, MB and FMG drafted the project application and supervised the underlying study. AM is responsible for the original study concept and data interpretation. AG analysed the data and prepared the figures and tables. CW is responsible for data management. RK-M performed statistical analysis. AM drafted the paper. MvdA, OAA and RB made critical revisions, AM (a.mueller@allgemeinmedizin.uni-frankfurt.de) and KK (karimova@allgemeinmedizin.uni-frankfurt.de) as guarantors take responsibility for the integrity of the work as a whole.
Funding Innovation Fund of the Federal Joint Committee, Germany (01VSF17002).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.