Article Text

Abstract
Objectives This study aimed to investigate adherence to Consolidated Standards of Reporting Trials (CONSORT) for abstracts in reports of randomised trials on child and adolescent depression prevention. Secondary objective was to examine factors associated with overall reporting quality.
Design Meta-epidemiological study.
Data sources We searched MEDLINE, EMBASE, PsycINFO, PsycArticles and CENTRAL.
Eligibility criteria Trials were eligible if the sample consisted of children and adolescents under 18 years with or without an increased risk for depression or subthreshold depression. We included reports published from 1 January 2003 to 8 August 2020 on randomised controlled trials (RCTs) and cluster randomised trials (CRTs) assessing universal, selective and indicated interventions aiming to prevent the onset of depression or reducing depressive symptoms.
Data extraction and synthesis As the primary outcome measure, we assessed for each trial abstract whether information recommended by CONSORT was adequately reported, inadequately reported or not reported. Moreover, we calculated a summative score of overall reporting quality and analysed associations with trial and journal characteristics.
Results We identified 169 eligible studies, 103 (61%) RCTs and 66 (39%) CRTs. Adequate reporting varied considerably across CONSORT items: while 9 out of 10 abstracts adequately reported the study objective, no abstract adequately provided information on blinding. Important adverse events or side effects were only adequately reported in one out of 169 abstracts. Summative scores for the abstracts’ overall reporting quality ranged from 17% to 83%, with a median of 40%. Scores were associated with the number of authors, abstract word count, journal impact factor, year of publication and abstract structure.
Conclusions Reporting quality for abstracts of trials on child and adolescent depression prevention is suboptimal. To help health professionals make informed judgements, efforts for improving adherence to reporting guidelines for abstracts are needed.
- STATISTICS & RESEARCH METHODS
- MENTAL HEALTH
- PAEDIATRICS
- Child & adolescent psychiatry
- Depression & mood disorders
Data availability statement
Data are available in a public, open access repository. https://osf.io/ahzwn/?view_only=e2f08c5c0d2d4936ba88d38968aba5d9.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- STATISTICS & RESEARCH METHODS
- MENTAL HEALTH
- PAEDIATRICS
- Child & adolescent psychiatry
- Depression & mood disorders
Strengths and limitations of this study
This study is the first to systematically assess the reporting quality for abstracts of randomised trials on paediatric depression prevention.
Our extensive, reproducible search strategy identified 169 eligible journal articles reflecting the available evidence from such trials published in 2003–2020.
Two reviewers independently screened abstracts and extracted data using standardised methods, but the reviewers were not blinded to meta-data such as study authors, journal name or year of publication.
Since no method has so far been established for determining overall reporting quality of abstracts, we approximated overall reporting quality by calculating a summative score based on Consolidated Standards of Reporting Trials items.
Because we applied a topic-based approach without restricting the information source to specific journals, our study findings offer insights into general reporting quality in trials on childhood depression prevention.
Introduction
Reports of trials should provide all necessary information allowing readers to evaluate the reproducibility, validity and utility of studies and findings.1 2 Poor reporting of health research leads, at the very least, to avoidable waste of resources3 and can ultimately jeopardise patient care.4 The same applies to abstracts of trials. Due to time, access and language constraints, health professionals often use abstracts as the primary source of information to learn about a trial,5 6 and the way abstracts report study details can influence their decisions in patient management.7 Researchers conducting systematic reviews and meta-analyses may incorrectly exclude eligible studies in title and abstract screening due to poor reporting which can distort evidence synthesis.8 Moreover, indexers of literature databases rely on adequate title and abstract reporting to correctly determine search terms such as medical subject headings, otherwise relevant journal articles cannot be found, read and quoted to affect medical practice.
For these reasons, authors of randomised trial reports are encouraged to follow the Consolidated Standards of Reporting Trials (CONSORT) guidelines5–8 and its extension for abstracts (CONSORT-A).9 10 CONSORT-A was published in 2008 to provide guidance to authors on information to be reported in abstracts of randomised controlled trials (RCTs). In 2012, the guidelines were further complemented by a module for cluster randomised trial (CRT) abstracts (CONSORT-C).11 Although some improvement in reporting quality of trials has been observed over recent years,12 general adherence to CONSORT guidelines remains suboptimal in articles published both in general medicine13–17 and psychiatry/psychology journals.18–20 Similar results have been reported from studies on adherence to CONSORT-A for abstract reporting in various health disciplines including one previous study on abstracts of psychiatric RCTs.21 However, no prior study has investigated the abstract reporting quality of depression prevention trials in young people. We, therefore, aimed to evaluate to what extend CONSORT-A and CONSORT-C criteria are met by abstracts of reports on child and adolescent depression prevention trials. Secondary objective of our study was to explore trial and journal characteristics associated with the abstracts’ overall reporting quality.
Methods
Eligibility criteria
We included reports on RCTs and CRTs assessing universal, selective and indicated interventions aiming to prevent the onset of depression or reducing depressive symptoms in children and adolescents under 18 years with or without an increased risk for depression or subthreshold depression. A detailed list of the eligibility criteria is provided in online supplemental file S1. We only included research articles published in peer-reviewed journals, the primary source of information for paediatric health specialists,22 and we considered the period between 1 January 2003 and 5 August 2020 to assess reporting quality before and after the publication of CONSORT-A and CONSORT-C guidelines.
Supplemental material
Information sources
We searched the electronic literature databases MEDLINE (via PubMed and Ovid), EMBASE (via Ovid), PsycINFO (via EBSCOhost), PsycArticles (via EBSCOhost) and CENTRAL (via Cochrane Library) on 9 March 2019 and updated the search on 8 August 2020. Search strings were developed in collaboration with a trained librarian. The electronic search strategy for MEDLINE via PubMed is shown in online supplemental file S2. Electronic search strategies for the other databases are provided in an online repository.23 Additional articles were retrieved by handsearching four specialty journals and the reference lists of systematic reviews (online supplemental file S3).
Study selection and data collection
The study selection process consisted of a title and abstract screening, a full-text screening and a discussion and consensus phase (figure 1). Two independent reviewers extracted information from articles into piloted spreadsheets with drop-down menus. The reviewers first determined whether randomisation was performed on an individual (RCT) or cluster level (CRT) and subsequently assessed all abstracts according to CONSORT-A and CRTs additionally according to CONSORT-C.10 11 For each item, the reviewers judged whether the abstract reported information adequately, inadequately or not at all.

PRISMA flow chart depicting the study selection process. PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses. (Source: https://www.bmj.com/content/372/bmj.n160)
For items with multiple dimensions, we operationalised each dimension separately and then created item variables for analysis based on the extracted information. For example, CONSORT-A item 03 Participants requires reporting the eligibility criteria for participants and settings where the data were collected. Thus, if both dimensions were reported adequately (or not at all), then the item was judged as adequately reported (or as not reported). However, if either the eligibility criteria for participants or for settings was reported inadequately, the item was judged as inadequately reported.
Based on earlier studies, we prespecified seven study characteristics previously associated with overall reporting quality (online supplemental file S4). We operationalised these study characteristics using the variable definitions in online supplemental file S5.
Statistical analysis
We used descriptive statistics to summarise the extent to which RCT and CRT abstracts adhered to the 15 CONSORT-A items and CRT abstracts adhered to the additional eight CONSORT-C items. For each CONSORT item, we thus present the proportion of trial abstracts adequately, inadequately or not reporting the item information as required by the appropriate guideline.
We calculated summative scores of overall reporting quality grading CONSORT items as follows: (1) adequately reported (two points), (2) inadequately reported (one point) and (3) not reported (0 points). Depending on the study design, these overall reporting quality scores (RQS) could thus theoretically range from 0 to 30 for RCTs (15 CONSORT-A items) and from 0 to 46 for CRTs (8 additional CONSORT-C items). We transformed RQS to standardised percentages with possible ranges from 0 (lowest reporting quality) to 100 (highest reporting quality). We compared unstructured (1 section), structured (2–4 sections) and highly structured (>4 sections) abstracts24 in relation to RQS using the Kruskal-Wallis test. We fitted separate linear regression models to quantify associations between overall reporting quality and (1) number of authors, (2) sample size, (3) number of sampling points, (4) abstract word count, (5) journal impact factor and (6) year of publication. Because of heavily skewed distributions (online supplemental file S6) we log-transformed (log 10) the first five above-mentioned variables for analysis. We used RStudio (R V.4.1.1) for data analysis.
Patient and public involvement
Instead of patient data we used information of previously published trial reports. Thus, no patients or public were involved in this study. Yet, our results can inform authors, editors, reviewers and readers of the scientific literature.
Results
Included abstracts
We screened the title and abstract of 4279 articles and the full text of 520 articles, and we ultimately included 169 articles in the data synthesis (figure 1). Inter-rater reliability as assessed by Cohen’s kappa (unweighted) for the agreement between the three reviewer pairs (article eligible vs non-eligible) was moderate in the title and abstract screening with κ=0.39, κ=0.47 and κ=0.55 and higher in the full text screening with κ=0.59, κ=0.73 and κ=0.67. For interrater reliability on CONSORT items, please refer to online supplemental file S7.
Of all 169 articles, 61% were reports on RCTs (n=103) and 39% reports on CRTs (n=66). More than half of these articles were published between 2015 and 2020 (online supplemental file S8). Median number of authors was five (range: 1–24, Q1: 4, Q3: 8). Sample size ranged from 23 to 12 391 participants, with a median of 271 (Q1: 120, Q3: 670). Twenty-one of the reported studies were performed at a single site, while 117 were reports of multicentre studies. Median abstract word count was 225 words, with range from 68 to 623 (Q1: 175, Q3: 253). The median journal impact factor was 3.2 (Q1: 2.1, Q3: 4.3). Fifty-seven per cent of the included abstracts were unstructured (n=97), one-third of the abstracts were structured with two to four sections (n=56), and the remaining 10% were highly structured (n=16), that is, with more than four sections.
Adherence to CONSORT for abstracts
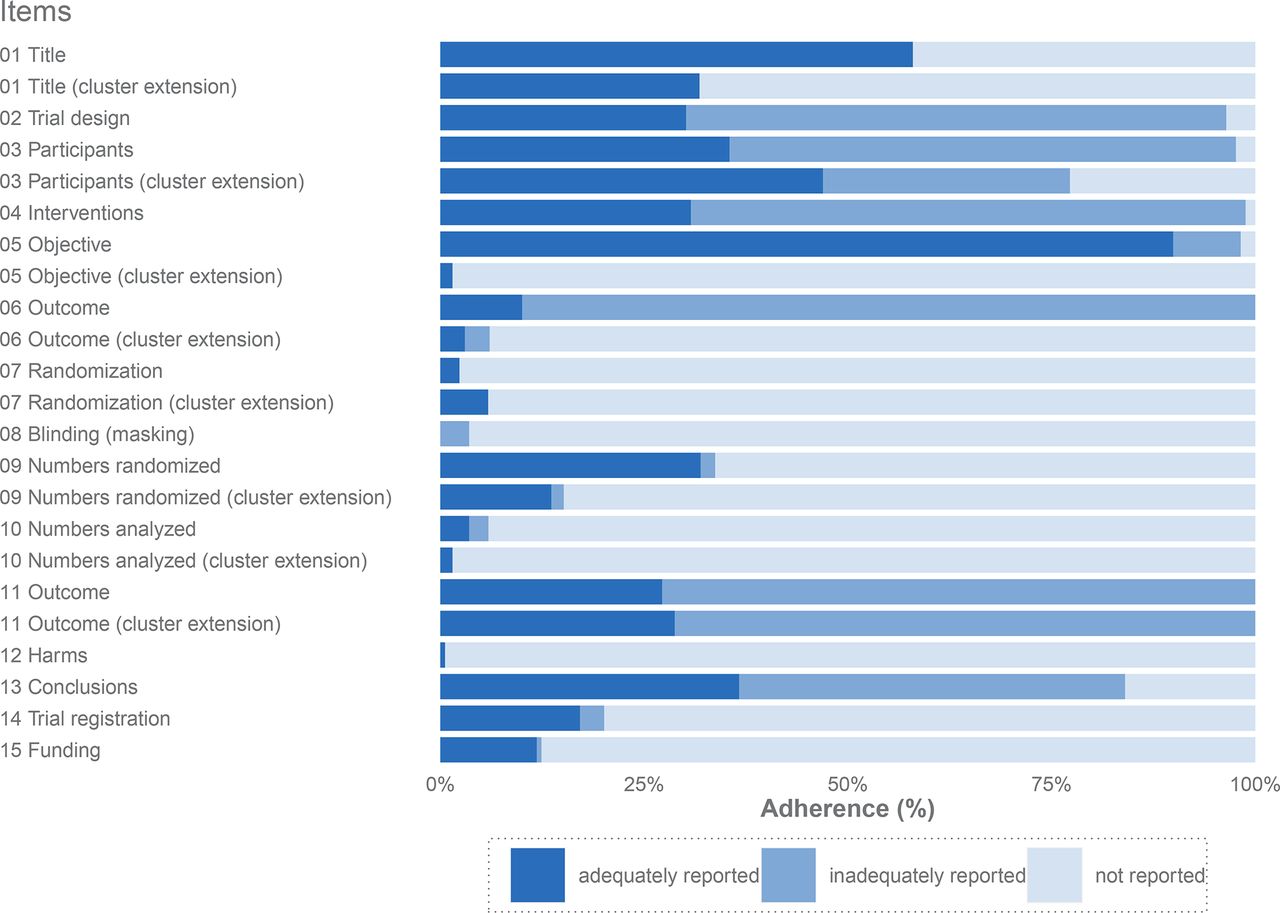
Figure 2 summarises the results on adherence to CONSORT for abstracts items, that is, the proportion of trial abstracts reporting item information adequately, inadequately and not at all (please see also online supplemental file S7 for exact figures). The percentage of adequate reporting among general items ranged from 58.0% (item 01 Title) to 30.2% (item 02 Trial design). With regard to trial methodology, the highest percentage of adequate reporting was in item 05 Objective and the lowest in item 08 Blinding. Regarding trial results, item 13 Conclusions had the highest percentage of adequate reporting (36.7%) and item 12 Harms the lowest (0.6%).

Percentage of abstracts adhering to CONSORT items in 169 trial reports on the prevention of depression in children and adolescents. CONSORT, Consolidated Standards of Reporting Trials.
Overall reporting quality and associated factors
The distribution of the RQS among all abstracts and stratified by study design is depicted in figure 3.

Distribution of overall reporting quality by study design. CRT, cluster randomised trial; RCT, randomised controlled trial.
The graphs in figure 4 visualise the relationship of trial and journal characteristics with RQS. Number of authors, abstract word count and journal impact factor were positively associated with RQS. For example, for every 10% increase in the journal impact factor, the RQS increased by about 1.9 percentage points (calculation: coefficient 5.6×log(1.10) ≈ 1.9). Structured (2–4 sections) and in particular highly structured abstracts (>4 sections) had a higher RQS than unstructured abstracts (1 section). Sample size and number of sampling points were not related to RQS. Finally, after publication of CONSORT-A in 2008, RQS annually increased by 0.57 units.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Associations of overall reporting quality with abstract and journal characteristics.
An additional before-and-after comparison illustrates that the RQS was higher in the period from 2008 to 2020 (median: 36.7, Q1: 30.0, Q3: 43.5) than in the period from 2003 to 2007 (median: 32.0, Q1: 22.9, Q3: 41.8).
Discussion
In this study, we assessed reporting quality for abstracts of child and adolescent depression prevention trial reports. Overall, we found that adherence with CONSORT-A and CONSORT-C for abstracts is suboptimal in journal articles reporting on such studies between 2003 and 2020.
Comparison with previous studies
Meta-epidemiological studies of reporting quality follow two distinct methodological approaches. In the journal-based approach, one or more journals are selected, usually top journals in a specific field with a high-impact factor and the published articles are assessed. Examples comprise studies on the abstract reporting quality in general15 16 25–27 and internal medicine,28–30 anaesthesiology,31–33 surgery,34 35 nursing36 and critical care.37 The only prior study on abstracts of psychiatric trials followed this approach as well.21 However, the restriction to top journals could affect generalisability, as a higher impact factor may be associated with better reporting quality.21 28 36 38–42 Thus, journal-based meta-epidemiological studies might overestimate the quality of abstract reporting. On the contrary, in the topic-based approach, no constraints are made regarding the journals. Instead, literature databases are systematically searched for articles on a specific disease, therapy or other topic.38 39 42–48 This increases the variety of journals, making it difficult to draw conclusions about reporting quality of specific journals. However, the topic-based approach increases generalisability by also including journals with a lower impact factor and thus provide a more complete picture of reporting quality.
General items
In our study, the general items 01 Title and 02 Trial design were adequately reported in about 60% and 30% of trial abstracts, respectively. Similarly, Song et al reported in their study that 66% of trials stated ‘randomised’ in the title but only 14% of trials described the study design in the abstract.21
CONSORT-C requires that abstracts are denoted as cluster randomised in the title (item 01 Title (cluster extension)). In our study, however, only one-third of all CRT abstracts adequately reported this item. To our knowledge, this study is the first to examine adherence to CONSORT-C guidelines in CRT abstracts. Yet, some meta-epidemiological studies examined adherence to CONSORT-C for full texts, which includes the same item. For example, Chan et al showed that about two-thirds of pilot or feasibility CRT reports published between 2011 and 2014 adequately met this CONSORT item.49 Similarly, Ivers et al, Diaz-Ordaz et al, and Walleser et al found that 48%, 60% and 98% of CRTs, respectively, state in the title or abstract that the study is a CRT.50–52
Trial methodology
Among all 169 included abstracts, 36% adequately reported both eligibility criteria for participants and setting. In line with many previous studies,16 21 28 33 37 53 we extracted the originally combined information for CONSORT item 03 Participants using separate dimensions: (1) eligibility criteria for participants and (2) eligibility criteria for settings. In contrast, other studies assessed reporting of eligibility criteria for participants only.26 43 54 55 It is not surprising that these studies show the higher proportions of adequate reporting for this item.
We found that 98% of abstracts failed to adequately include information on how participants were assigned to interventions and that 96% of abstracts lacked complete information on whether participants, programme deliverer and data collectors/analysts were blinded. With a few exceptions,16 36 42–44 48 most previous studies reported adherence to these items of well below 10%.15 21 25 26 28–35 37–41 45 46 55–60
Trial results
The number of participants randomised to each group was adequately reported in approximately one-third of all abstracts and only 4% of the included trial abstracts adequately reported the number of participants analysed in each group. This gap between item 09 Numbers randomised and item 10 Numbers analysed has also been observed in previous studies.57
Only one article in our sample elaborated on adverse or unintended effects in the abstract, whereas all other 168 abstracts failed to mention important adverse events or side effects (item 12 Harms). Other meta-epidemiological studies found considerably higher proportions of adequate reporting for this item, particularly trials that also included pharmacological interventions.26 34 44
Finally, our study showed that about 12% of abstracts adequately reported the item 15 Funding. Many meta-epidemiological studies even found the proportion of abstracts that adequately report funding is in the single digits21 30 33 37 40 46 59 61 or even zero per cent.29 31 32 34 35 38 41 45 55–57 60 However, it may be rather the journal regulations than CONSORT to influence whether funding information appears in the abstract or in another place, for example, at the end of the manuscript.
Associations with overall reporting quality
In line with previous findings,28 39–41 46 59 we observed that overall reporting quality increases with the number of authors. In contrast, some studies found no such relationship.21 36 46 56–58 Other studies suggest, although not consistently,62 that the involvement of methodologists is associated with higher reporting quality.51 63 64 However, number of authors may reflect at least to some extent whether author groups include methodologists.
Furthermore, overall reporting quality seems to be positively related with the abstract word count. This observation is consistent with the results of previous meta-epidemiological studies.39–43 46 48 56 61 It seems that the more words authors have at their disposal, the more information they can provide.
Our data suggest that a higher journal impact factor correlates with increased overall reporting quality. If the impact factor is an indicator for journal quality,65 journals with a higher impact factor may apply more rigorous quality control to reporting. This result would thus underline that restricting studies to top journals may hamper generalisability.
We observed that structured abstracts showed higher overall reporting quality compared with unstructured abstracts. With some exceptions,16 40 46 48 57 many meta-epidemiological studies have shown similar results both since21 28 36 39 41 42 56 61 and before the publication of CONSORT-A.66–72 However, a few studies also suggest that structured abstracts are not superior73–75 and that abstract structure was unrelated to reporting quality.76
In line with previous studies, we found that abstract reporting quality was higher in the period since the publication of CONSORT-A as compared with the period before.21 26 29 34 38 40 41 However, our data do not allow causal conclusions. Our data indicate that overall reporting quality is improving since 2008: in contrast to the period from 2003 to 2007, the RQS increased between 2008 and 2020. Chhapola et al observed a similar trend comparing the reporting quality of trial abstracts published in high-impact paediatric journals in 2003–2007 and 2010–2014.77
Strengths and limitations
This study is the first on reporting quality of trial abstracts in childhood depression prevention. Key strength of our study is the topic-based approach we have chosen; compared with journal-based studies, our results provide a more complete picture of abstract reporting in the field. We carried out an extensive, reproducible methodology to screen the literature for eligible studies and retrieve study information. We analysed abstracts published over a broad timespan allowing for comparison of reporting quality before and after publication of CONSORT guidelines. We assess adherence not only to CONSORT-A for RCT abstracts but also to CONSORT-C for CRT abstracts, which was not evaluated by any prior study.
We applied CONSORT to measure reporting quality, although it was not designed for this purpose. However, in the current absence of standardised tools for assessment, validated guidelines such as CONSORT are the best available choice to evaluate reporting quality. Moreover, CONSORT for social and psychological interventions were not checked for adherence.78 79 However, these guidelines were only published in 2017 and 2018, respectively, and thus a few studies could have considered these standards. We assess the reporting quality of trial abstracts and cannot draw conclusions about the quality of reporting in the main text. Reviewers were not blinded to trial and journal characteristics such as authors, publication date and impact factor, during the study selection and the data extraction. We can, therefore, not exclude the possibility of bias in the evaluation due to metadata insight of the judging reviewers.
When we calculated overall RQS, we treated each CONSORT item equally, although some items could be more or less relevant than others.30 37 43 These scores are simplified proxies to represent reporting quality with a single measure. The assessment of reporting quality should however primarily be based on the individual items.31
We did not assess associations between overall reporting quality and journal requirements, such as word count limits and format structure. However, the word count and structure of the included abstracts may largely reflect these journal requirements.
We used descriptive modelling to explore factors associated of reporting quality; neither predictive nor causal conclusions can be derived from this. Unmeasured factors such as journal endorsement of CONSORT80 may also be associated with reporting quality. Findings from our secondary research aim may thus be incomplete and should be interpreted with caution.
Conclusions
Reporting quality plays a crucial role in generating and translating scientific evidence as it increases transparency and accuracy and thereby enables health professionals to identify, evaluate and replicate trial results. CONSORT extensions are valuable tools for authors, reviewers and editors to formulate trial abstracts in a transparent and comprehensible way. Although these tools have been openly available for years, the reporting quality of RCT and CRT abstracts on the prevention of depression in children and adolescents is suboptimal. According to our results, some CONSORT-A and CONSORT-C items are adequately reported in most depression prevention trial abstracts, and this should be the benchmark for all items. Interventions aimed at strengthening abstract reporting quality are thus needed.81 These efforts will very likely not only benefit the scientific community and practitioners in the field, but may ultimately improve mental healthcare for children and adolescents worldwide.
Data availability statement
Data are available in a public, open access repository. https://osf.io/ahzwn/?view_only=e2f08c5c0d2d4936ba88d38968aba5d9.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We would like to thank Dr Jan Taubitz at the Medical Library, Charité - Universitätsmedizin Berlin, who with his expertise provided support for the research project in the development and evaluation of the literature search strategy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JW is the guarantor. JW conceived the idea for the project. JW and CP developed the concept and methods. JW and JN performed the data selection and extraction. CP gave final instructions when consensus could not be reached. JW performed the statistical analysis and interpreted the study findings. JW drafted the first version of the manuscript. CP contributed to data interpretation, writing and editing. All authors reviewed and approved the final manuscript before submission.
Funding We acknowledge financial support from the Open Access Publication Fund of Charité – Universitätsmedizin Berlin and the German Research Foundation (DFG).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.